
When the Insulin Just Won't Work: The Resistance Work-Up
Claire Greenway
BVM&S MRCVS
There's a sentence I hear when an owner has reached the end of their patience, and it always carries the same flat exhaustion. "We keep putting the dose up and it makes no difference." By then they've usually been climbing the dose for weeks, the numbers are still stubbornly high, and the fear underneath is that their pet is one of the unlucky ones the insulin simply won't touch.
So let me give you the reassuring half first, because it's also the clinically true half. "The insulin won't work" is, far more often than not, a fixable problem with a findable name, and that name is usually something dull and mechanical rather than a dreadful hidden disease. The way to it is not another dose increase. It's a methodical work-up, done in a deliberate order, that clears the common, boring causes before anyone reaches for the exotic ones. This page is that ladder. Its companion, The Unstable, Brittle Diabetic, is the calmer overview; this is the hunt underneath it.
When does a "high dose" actually count as resistance?
Not every pet that takes a while to settle is resistant, so it helps to know when this page is for you. Most diabetic dogs end up well controlled on modest insulin: the usual maintenance dose is around half a unit per kilogram twice daily, in a range of about 0.2 to 1.0 U/kg, started low at roughly 0.25 U/kg twice daily and crept up slowly (Behrend et al., 2018). True resistance, in the sense your vet means, is suspected once adequate control still can't be reached above roughly 1.5 units per kilogram per injection in either species, with a practical ceiling in cats of around 6 units per dose, or whenever the requirement keeps swinging without ever landing (Bruyette, 2015; Behrend et al., 2018).
Hold that number loosely: it is a flag to investigate, not a diagnosis, and certainly not a target to dose toward. Crossing 1.5 U/kg doesn't mean "give more," it means "stop and look for why." Plenty of pets who feel resistant to a worried owner haven't crossed it at all; they're under-covered, mis-measured, or running out of insulin between doses, each a more cheerful problem than true resistance.
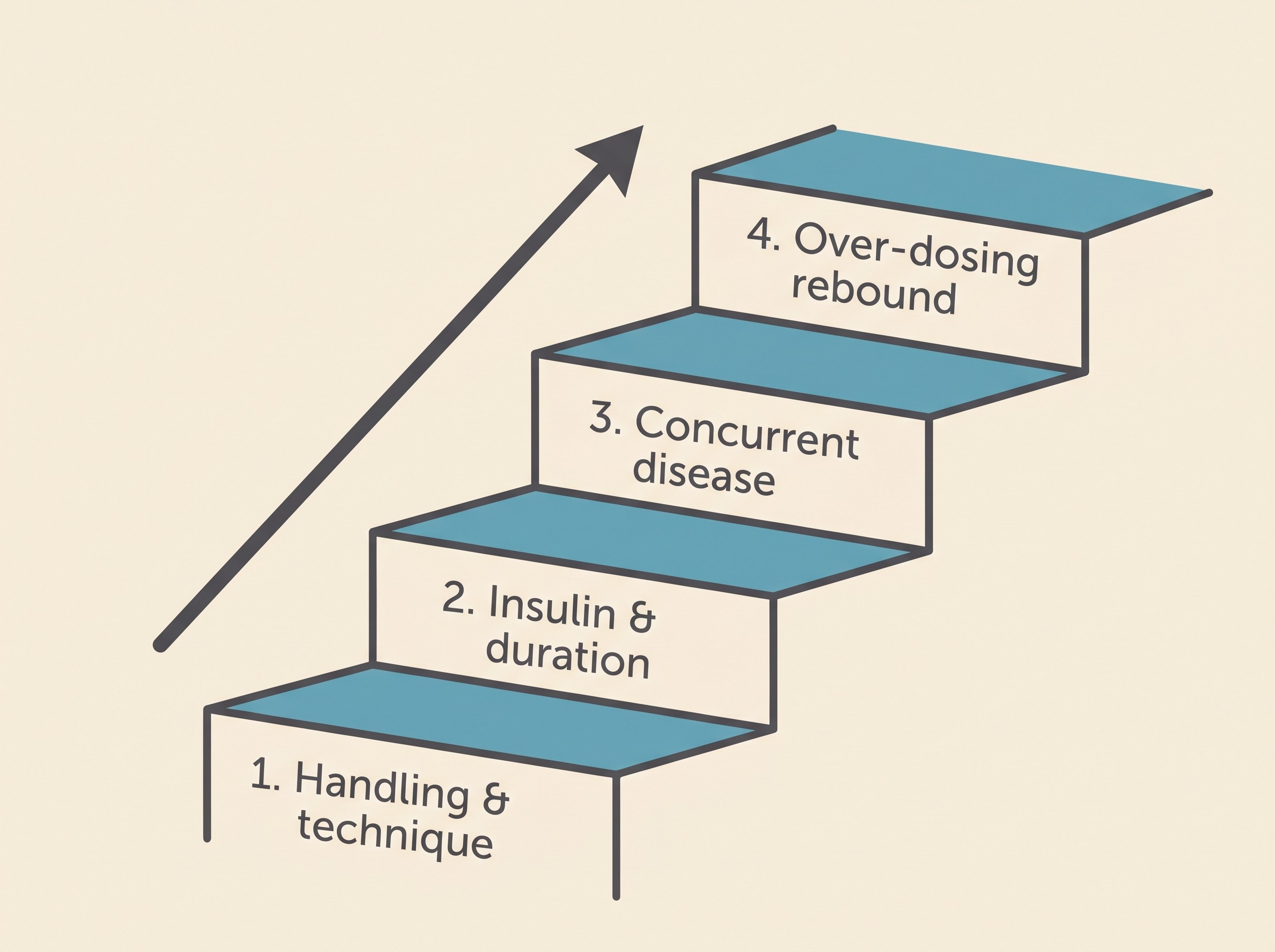
Bottom of the ladder first
Both main veterinary frameworks structure the hunt the same way, and it runs against instinct, so it's worth saying plainly. The order is: first the insulin and how it's handled, then the insulin's behaviour in that particular animal, and only then the patient's own body and any second disease (Behrend et al., 2018; Bruyette, 2015). A genuine concurrent disease is the commonest true cause of resistance, yet handling and technique are checked first, precisely because they are so common and so easily fixed (Bruyette, 2015). You do not climb to Step 3 before you've cleared Steps 1 and 2. That single discipline saves a pet from a dangerous spiral of dose increases chasing a problem that was never about the dose.
Step 1: the dull, fixable causes (where most of it lives)
This is the unglamorous rung, and the most productive. A surprising share of "the insulin isn't working" lives right here, in how it's stored, drawn up and given.
Has the insulin gone off? Insulin is a fragile protein. Heat, freezing at the back of a too-cold fridge, light and simple age can all denature it, so a quietly inactivated vial delivers far less than the syringe says (Thompson et al., 2015). Suspensions add a trap: if a cloudy insulin isn't re-mixed exactly as its label instructs, the dose drawn up can vary wildly day to day, and a vial gone discoloured or more cloudy than usual should be discarded (Thompson et al., 2015; iCatCare, 2025). The how-to belongs to Storing and Handling Insulin, and a fresh vial handled correctly is one of the first things I'd try.
Is it the right syringe for the insulin? This is the silent classic, common and completely invisible on a meter. Veterinary insulins like Caninsulin (Vetsulin in the US) and ProZinc are U-40, with 40 units per millilitre; most human-origin insulins used in pets, including Lantus (glargine) and Levemir (detemir), are U-100, two and a half times as concentrated (Thompson et al., 2015). The syringe must match the insulin. Put U-100 insulin in a U-40 syringe and you give roughly two and a half times the intended dose; put U-40 insulin in a U-100 syringe and you give only about 40% of it, a silent under-dose that masquerades perfectly as "the insulin doesn't work." U-100 syringes carry an orange cap, U-40 a red one. It's checkable in thirty seconds and explains more "resistant" pets than any tumour.
Is it actually going in? Faulty technique is common, expected and nobody's fault. An air bubble steals part of the dose; insulin can end up in the fur, or in a site gone lumpy from months of the same spot, where it absorbs poorly. The first thing a good vet does with a difficult diabetic is watch the owner draw up and inject, because so often the answer hides in that ordinary moment (Behrend et al., 2018); the technique, done without fear, lives in Your First Insulin Injection. Two safety lines belong right here: if you are ever unsure whether a dose went in, do not give it again to be safe. Skip it, wait for the next one, because a missed dose is far safer than a double, and never re-dose into a pet you suspect might be low. Under-dosing and too-infrequent dosing sit on this rung too: a pet given insulin once daily when theirs only lasts half a day spends the rest of it uncovered and high, looking like a dose problem when it's really a schedule one (Bruyette, 2015).
Step 2: the insulin's behaviour, especially how long it lasts
If Step 1 is clean and the pet still runs high, the next question isn't "is it enough?" but "is it lasting?" A pet can look completely resistant when the insulin simply wears off too soon for them, leaving hours of every day with no cover at all.
Porcine lente (Caninsulin/Vetsulin) is the textbook example. It gives two peaks, at roughly four and eleven hours, and lasts about sixteen hours in the average dog, but individuals vary enormously and many run far shorter, which is why twice-daily dosing is needed in most dogs (Thompson et al., 2015). A dog whose insulin is gone by hour ten reads high before the next injection no matter how big you make the dose. NPH is shorter still, four to ten hours in dogs and under eight in many cats, too short for reliable twice-daily cover (Thompson et al., 2015). The fix for a duration problem is a different insulin or interval, not more units, and the options sit in The Insulin Types Explained. You cannot tell a too-short duration apart from genuine resistance on a single reading: the pet looks high either way, so you need to see the whole day.
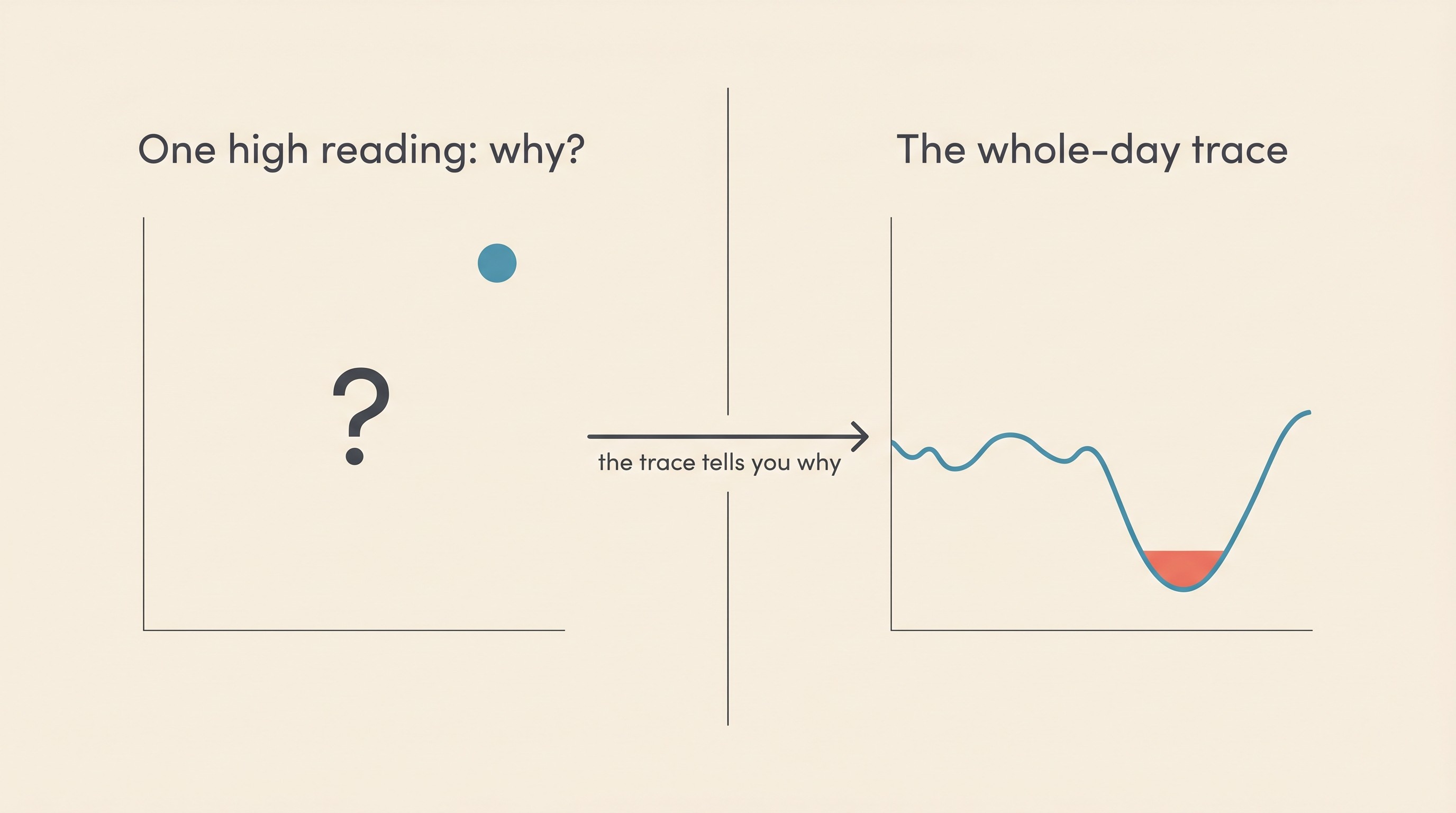
The instrument that tells the causes apart
This is the practical heart of the work-up. You cannot tell under-dosing, a too-short duration, an unseen overnight low and a falsely-high stressed cat apart from a single spot reading: the pet looks high on all four. What separates them is a picture of the glucose across the whole dosing interval, a blood glucose curve, or better still a continuous glucose monitor, a small sensor worn on the skin that reads day and night.
A serial curve shows the lowest point, how long the insulin is genuinely lasting, and where the glucose sits before the next dose (Behrend et al., 2018). A continuous sensor adds what a clinic curve can't: the unseen overnight nadir, the brief or nocturnal low a daytime check sails past (CGM small-animal reviews). That dip is what separates a truly resistant pet, high right across the interval, from one dropping too low at 3am and rebounding, or one whose insulin has simply run out. I won't teach you to read either here: Reading a Glucose Curve and Continuous Glucose Monitors on Pets own that. On this ladder they are simply the instrument that turns "unstable" into "diagnosable."
A feline trap lives here too. A cat who reads sky-high in the clinic on a seemingly large dose may not be resistant at all, just frightened, because stress alone can drive a cat's glucose up sharply (iCatCare, 2025; Behrend et al., 2018). This is why home and sensor data gathered where the cat is calm, plus fructosamine (a blood test reflecting the average glucose over the preceding week or so, immune to a single stress spike), belong in the work-up before anyone concludes the insulin "won't work"; the detail sits in Fructosamine and the Vet Rechecks (iCatCare, 2025). One last gremlin: human glucometers tend to read a pet's glucose lower than it truly is, so a poor-looking result can be a meter artefact rather than poor control (portable-meter validation studies). A pet-calibrated meter such as the AlphaTrak, or a sensor, avoids reading a quirk as a treatment failure, as Home Blood Glucose Monitoring covers.
Step 4: the over-dosing rebound, real but rare
One rung deserves its place precisely because it's so often put in the wrong place. An unseen low can prompt the body to rebound high, the so-called Somogyi effect, which is part of why a high reading must never automatically mean "give more." It's real, but far rarer than the forums suggest. In the largest dataset we have, 10,767 glucose curves from 55 glargine-treated cats, rebound consistent with the Somogyi effect appeared in only four isolated events, around 0.42% of curves, despite plenty of biochemical lows (Roomp & Rand, 2016). The rule to carry: do not reduce, or chase with more, insulin for a high reading unless there's actual evidence of a preceding low (Roomp & Rand, 2016). The physiology belongs to Somogyi and Dose-Chasing; here it's simply the reminder that a high number alone never justifies turning the dose by yourself, in either direction.
Step 3: only now, the hunt for a second disease
Once Steps 1 and 2 are genuinely clear, the handling sound, the syringe matched, the technique watched, the insulin fresh and lasting a sensible length, and a curve or sensor confirming the glucose really is staying high all interval, then it's time to screen for a concurrent disease driving true resistance. Reaching this rung is not bad news. It usually means we've found the explanation, and an explanation comes with a treatment.
I'll name the territory rather than tour it, because the disease-by-disease detail is owned elsewhere. In dogs, the leading drivers are obesity, Cushing's disease (hyperadrenocorticism), the hormone cycle in an entire female (dioestrus), hidden infection in the urinary tract, mouth or skin, pancreatitis, hypothyroidism, and steroid medication the pet may be on for something else (Bruyette, 2015; Behrend et al., 2018). In cats, the single leading cause of clinically relevant insulin resistance is hypersomatotropism, better known as acromegaly: a small growth-hormone-secreting pituitary tumour, present in something like one in five to one in three diabetic cats and screened with a blood test for IGF-1, alongside Cushing's, hyperthyroidism, infection and pancreatitis (iCatCare, 2025; Bruyette, 2015). The crucial point about every one is the same: treat the second disease, not the insulin. A hidden disease can multiply the requirement several-fold, and no amount of dose-climbing wins against it (iCatCare, 2025). The full roll-call and the tests that find them is the job of The Concurrent Diseases That Fight Your Insulin, the page to read next, while the everyday drivers (weight, dental disease, urinary infection) have their own guide in Weight, Dental Disease and the Other Things That Quietly Wreck Control.
Climbing this ladder with your vet, not at the kitchen table
You climb this ladder with your vet, not solo. The rising-dose reflex, answering every high number by adding units, is exactly the instinct the work-up exists to interrupt, and acting on it alone is how pets get tipped into a hypoglycaemic crisis. So don't self-increase insulin off single high readings; and if your pet ever goes wobbly, weak, dull or trembling, or collapses or fits, treat it as a possible low: rub a little glucose, honey or sugar onto the gums, never pour liquid into a mouth that can't swallow, and get to a vet straight away. That emergency has its own page, the hypoglycaemia emergency.
Dog and cat diabetes remain two different diseases here too. A diabetic dog is insulin-dependent for life, so a resistant dog is one whose control we work to recover, with no remission to chase. A resistant cat is often more hopeful, because the thing fighting the insulin is frequently a reversible second disease, and treating it can sometimes reopen the door to remission. Either way the ladder is the same, and the great majority of "the insulin won't work" pets are sitting on a rung near the bottom of it, waiting for someone to check the dull thing first. This is the job the Glucose Companion was made for: log the doses, plot the curve or import a sensor trace, see the nadir and a hypo flag, and export a tidy report. Walk in with a trend, not a guess, and you've already done the hardest and most useful part of the hunt.
References
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Roomp, K., & Rand, J. S. (2016). Rebound hyperglycaemia in diabetic cats. Journal of Feline Medicine and Surgery, 18(8), 587-596.
- Thompson, A., Lathan, P., & Fleeman, L. (2015). Update on insulin treatment for dogs and cats: insulin dosing pens and more. Veterinary Medicine: Research and Reports, 6, 129-142.
- Bruyette, D. (2015). Insulin resistance: diagnosis and management. WSAVA World Congress Proceedings.
- iCatCare/ISFM. (2025). 2025 Consensus Guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery.
- CGM small-animal reviews: Clinician's Brief, Application & Use of a Continuous Glucose Monitor in Cats & Dogs; and Continuous glucose monitoring in small animals. ; https://pubmed.ncbi.nlm.nih.gov/23522178/
- Portable-meter validation studies: AlphaTrak and glucometer-comparison data. ; https://www.tandfonline.com/doi/full/10.1080/01652176.2015.1092617
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine