
The Unstable, Brittle Diabetic: Why Control Slips, and What To Do
Dr. Alastair Greenway
MRCVS
There's a particular kind of tiredness I've learned to recognise across the consulting table, and it doesn't belong to the pet. It belongs to the person opposite: the one who's been up in the night checking the cat, who's turned down a weekend because nobody else can manage the injections, whose meter read 4 one morning and 22 the next. This page is for that person.
An unstable diabetic almost always has a findable reason for being unstable: it is rarely a pet that "just needs more insulin," and rarely one that's beyond help. The way out is not an ever-bigger dose chased off every high reading; it's a calm, ordered hunt for the thing getting in the way. This article is the map for that hunt, naming each cause and pointing you to the guide that owns it.
"Unstable" and "brittle", in plain terms
These are alarming words, so let me make them ordinary. An uncontrolled diabetic is a pet whose clinical signs aren't settling: still drinking and weeing too much, still ravenous, still losing weight despite being on insulin (Behrend et al., 2018). The classic "brittle" diabetic is a step beyond that, the pet whose insulin requirement keeps swinging between too low and too high, the dose forever pushed up and down without ever landing on a number that holds (Cook, 2012). Unstable doesn't mean broken or hopeless; it means the diabetes hasn't yet settled into a predictable pattern, and that pattern nearly always has a reason worth hunting for.
Fix one thing in place first: dog diabetes and cat diabetes are two different diseases. A diabetic dog is insulin-dependent for life and will not remit, so steady control is the whole goal. A cat is more like a person with type-2 diabetes and can genuinely remit with good early control, so "unstable" in a cat also means a missed chance at remission.
Why "give more insulin" is usually the wrong instinct
A common and costly misconception is that a pet who isn't responding to insulin must simply need more of it, when in truth a whole list of other, more fixable problems should be considered first (Behrend et al., 2018). In real cases, poor control caused by an unseen low driving a rebound high actually improves when the dose comes down, not up (Della Maggiore, 2017). So here is the rule: a single high value is not, by itself, a reason to increase a dose, because a number has to be read against the clinical signs and the chance of stress, on a plan agreed with your vet (Behrend et al., 2018).
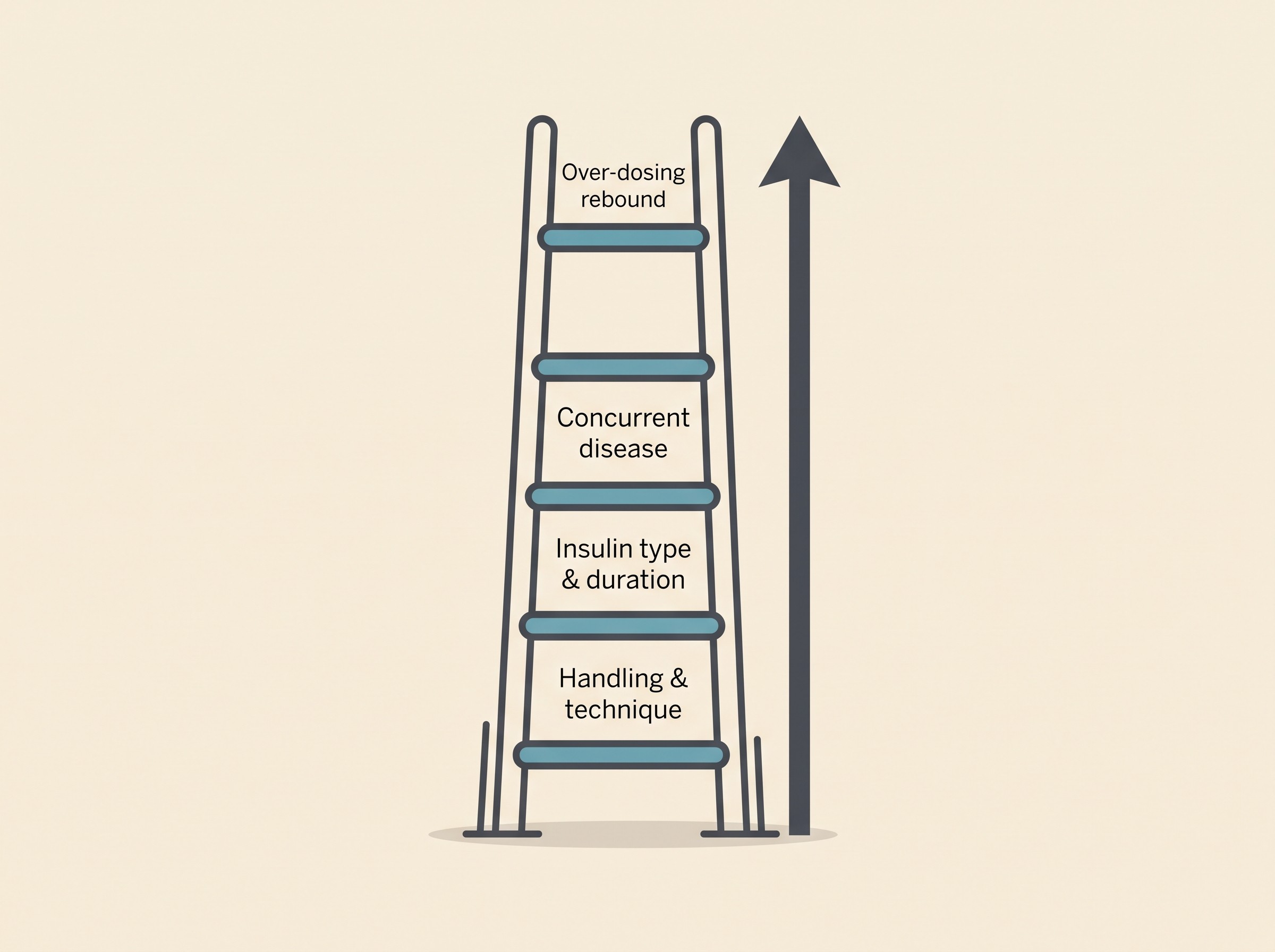
Start at the bottom of the ladder
The problems behind difficult control fall into three groups: the insulin itself, how it's given at home, and the patient's own body with whatever other diseases it carries. Although disease is the commonest true cause, it is wise to exclude the insulin and handling issues first, because they are so often easily found and fixed (Cook, 2012).
Rung one: handling, technique, and the vial in the fridge. This is the commonest culprit and the most fixable, with no blame attached. Even after careful teaching, many owners struggle to draw up exactly the right amount, and the usual hidden gremlin is an air bubble causing an accidental underdose, especially in the early weeks (Cook, 2012). The wrong syringe for the concentration, a vial frozen at the back of the fridge, a lumpy injection site, an insulin past its best: any one can make a good dose behave like a useless one, which is why a good vet checks it first, watching you draw up and inject and inspecting the vial (Behrend et al., 2018). The detail lives in storing and handling insulin, and it's where I'd start.
Rung two: the insulin itself, and how long it lasts. A pet can look "resistant" when the insulin simply wears off too soon for them. Recognised causes of poor control include a duration of action that is wrong for that animal, and an overlap where the glucose is still falling as the next dose goes in, pitching the pet into a low (Behrend et al., 2018). The classic example is lente insulin, Caninsulin in the UK and Vetsulin in the US. In many dogs it lasts a useful 14 to 24 hours, but in a lot of cats it's gone in around 8 to 12 hours (Caninsulin datasheet, MSD Animal Health). The cat's glucose dips, then climbs back up for hours before the next injection, and the owner watching that swing assumes the dose is too small. Often it isn't: this is a duration problem, and the fix is a different insulin or interval, not more units. The line-up sits in insulin types for dogs and cats.
Rung three: a concurrent disease fighting the insulin. Only now do we reach the thing owners fear first: the point at which a vet stops adding insulin and starts looking for something working against it. Most diabetic dogs and cats are controlled on around 1.0 unit per kilogram twice daily or less, and resistance is suspected once the dose climbs past roughly 1.5 units per kilogram in dogs, more than about 5 units per dose in cats, or whenever the requirement keeps swinging (Behrend et al., 2018; Nelson). A supporting lab clue is a high fructosamine, often over 500 and sometimes past 700 micromol per litre (Nelson). Past that threshold, the job is to hunt the hidden disease, not to keep climbing the dose. One example only: in cats the great hidden driver is acromegaly, thought to affect between one in three and one in five diabetic cats, most of whom look entirely ordinary across the room (Taylor et al., 2025). The full roll-call, and the tests that find it, is in the concurrent diseases that fight your insulin and the insulin resistance work-up.
Rung four: the over-dosing rebound, real but rare. An unseen low can prompt the body to bounce back high, another reason a high reading never automatically means "give more." But this rebound is far less common than the forums would have you believe: in the largest dataset we have, 10,767 glucose curves from 55 cats, curves consistent with rebound appeared just 0.42% of the time, and the authors warned against cutting a dose on a high number with no evidence of a preceding low (Roomp & Rand, 2016). The physiology, and how to recognise it, belong to the Somogyi effect and dose-chasing.
The tool that turns "unstable" into "diagnosable"
You cannot tell "not enough insulin" apart from "too much, with a rebound" apart from "wears off too soon" by a single reading or by how the pet looks. A blood glucose curve, or better still a continuous trace from a sensor worn on the skin, shows the lowest point, how long the insulin really lasts, and the hidden overnight dip nobody was awake to see, a far more useful picture than scattered single measurements ever give (Della Maggiore, 2017). And modern sensors are a genuine leap: in diabetic dogs, a flash glucose sensor picked up hypoglycaemic episodes in 60% of cases against just 9% for spot curves, catching the very lows that masquerade as instability (Del Baldo et al., 2025). There is a feline trap here too: a single high glucose in a cat frightened of the vet does not prove poor control, because stress alone can send a cat's glucose up by any amount (Taylor et al., 2025), one more reason the trend from home beats an in-clinic spike.
The Glucose Companion does exactly this job: log the doses, plot the curve or import a Libre trace, see the nadir and a hypo flag, and export a report to take in. Learning to read what it shows is in reading a glucose curve.
Two safety lines, stated plainly
Two more rules belong right next to "never chase a single number." First, if you are ever unsure whether a dose went in, do not give it again: skip it and wait for the next one, because a missed dose is far safer than a double. Second, learn the face of a low. A pet who goes wobbly, weak, dull or trembling, or who collapses or fits, may be hypoglycaemic, and that is the genuine emergency here: rub glucose, honey or sugar onto the gums, never pour liquid into a mouth that can't swallow, and get to a vet now. It has its own page: the hypoglycaemia emergency.
You are not failing, and the worry is legitimate
The toll on that tired person is real, and it has been measured. When researchers validated a quality-of-life tool for owners of diabetic dogs, 84% reported a negative impact of the disease on their own quality of life (Niessen et al., 2012). In the matching study of cat owners, the heaviest burdens were the difficulty of ever leaving the cat with someone else and the worry about hypoglycaemia; around 41% felt their cat's life would be a little better without the disease (Niessen et al., 2010). The worry you're carrying is close to universal: feeling overwhelmed is not a sign you're bad at this, and instability is a problem to solve with your vet, not a verdict on whether you're good enough.
Bringing in a specialist
If you've worked steadily up the ladder and your pet is still all over the place, asking about referral to an internal medicine or endocrinology specialist is a perfectly reasonable next step, especially for the harder feline cases and any pet stuck on very high doses. Hear that as a strength, not a defeat, and one with real grounds for optimism: in the case literature, when the underlying cause is found and treated, a favourable outcome is possible (Della Maggiore, 2015). Cases that feel hopeless at 2am turn out to be fixable once the right driver has a name.
Two signposts before I leave you. If your pet ever tips into a true crisis, going off their food, vomiting, profoundly lethargic, breathing fast or oddly, that can be diabetic ketoacidosis, a same-day emergency rather than something to puzzle over at home (see diabetic ketoacidosis). And if, after every avenue, control genuinely cannot be reached, there is a kinder, harder conversation in the quality-of-life decisions guide. This article stays on the solvable side of that line, because the great majority of unstable diabetics live there.
So where does this leave you tonight? With a map instead of a feeling. Instability has a findable reason, the hunt runs from handling up to the rare rebound, and the trend you build in the Glucose Companion is what tells the causes apart. The goal was never a flawless number on a meter; it's a steadier, more comfortable pet and a household that can breathe out again, often closer than it feels at half past ten at night.
References
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Cook, A. K. (2012). Identifying the reasons behind difficult-to-control diabetes in dogs. dvm360.
- Della Maggiore, A. (2017). Consider This Case: An Uncontrolled Diabetic Dog. Today's Veterinary Practice, March/April 2017.
- Della Maggiore, A. (2015). Consider This Case: An Uncontrolled Diabetic Cat. Today's Veterinary Practice, May/June 2015.
- Nelson, R. W. Insulin resistance. In Feldman, E. C., Nelson, R. W., Reusch, C., & Scott-Moncrieff, J. C. (Eds.), Canine and Feline Endocrinology (4th ed.). Elsevier.
- Roomp, K., & Rand, J. S. (2016). Rebound hyperglycaemia in diabetic cats. Journal of Feline Medicine and Surgery, 18(8), 587-596.
- Taylor, S., et al. (2025). 2025 iCatCare Consensus Guidelines on the Diagnosis and Management of Diabetes Mellitus in Cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
- Niessen, S. J. M., Powney, S., Guitian, J., Niessen, A. P. M., Pion, P. D., Shaw, J. A. M., & Church, D. B. (2012). Evaluation of a quality-of-life tool for dogs with diabetes mellitus. Journal of Veterinary Internal Medicine, 26(4), 953-961.
- Niessen, S. J. M., Powney, S., Guitian, J., Niessen, A. P. M., Pion, P. D., Shaw, J. A. M., & Church, D. B. (2010). Evaluation of a quality-of-life tool for cats with diabetes mellitus. Journal of Veterinary Internal Medicine, 24(5), 1098-1105.
- Del Baldo, F., et al. (2025). FreeStyle Libre-derived metrics in assessing glycemic control in diabetic dogs. Journal of Veterinary Internal Medicine, 39(4), e70151.
- MSD Animal Health. Caninsulin (porcine insulin zinc suspension) product information.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine