
Hypos: The Emergency Every Diabetic Owner Must Be Ready For
Dr. Alastair Greenway
MRCVS
Of all the things I tell a new diabetic owner, this is the one I'd ask you to hold onto hardest. Most of the daily routine you're learning is forgiving: get the timing a bit off, run a little high for an afternoon, and your pet is fine. The one exception, and the reason this page exists, is a blood sugar that drops too low. A "hypo", short for hypoglycaemia, is the genuine emergency of insulin treatment, and unlike almost everything else it can hurt your pet in minutes rather than weeks.
I don't say that to frighten you, but because a hypo is one of the few emergencies you can largely fix yourself, at home, with something already in your kitchen, as long as you know what to do before it happens. So if your pet is wobbly in front of you right now, here is the rescue first and the explanation after.
If you think it's happening right now
A hypo robs the brain of fuel. The brain runs almost entirely on glucose, so when the blood sugar falls it suffers first, which is why the signs are mostly neurological and why you must act fast (Cornell Riney Canine Health Center). Here is the rescue, the same for a dog or a cat.
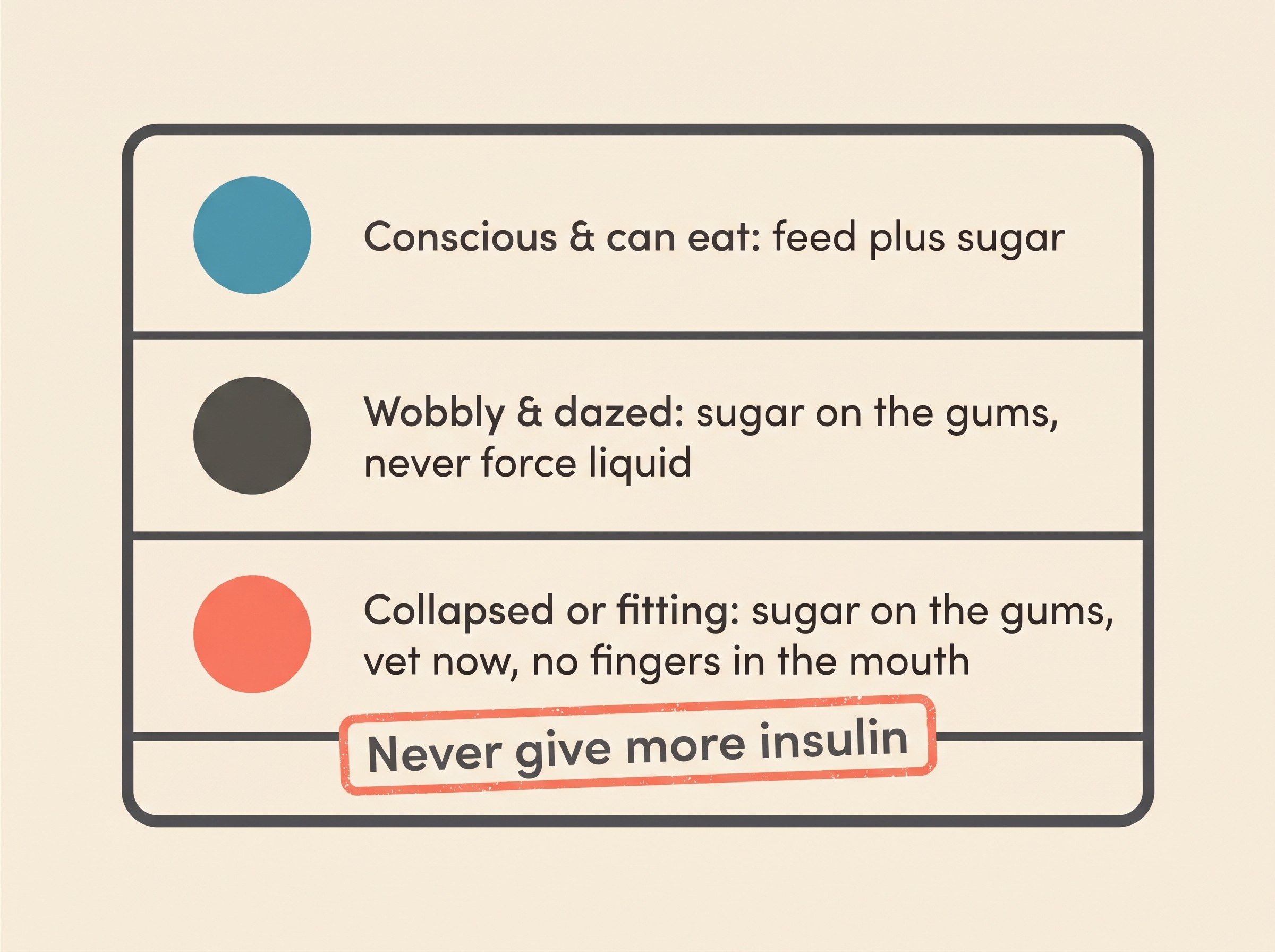
If your pet is conscious and can swallow, give sugar by mouth straight away: their normal food with a spoonful of honey or golden syrup stirred in, or a fast carbohydrate like plain white rice, bread or pasta (Bugbee et al., 2026; Cornell Riney Canine Health Center).
If your pet is dazed, weak, collapsed, twitching or fitting and cannot reliably swallow, do not try to feed them. Instead rub a sugar source onto the gums and inside the cheek: honey, golden syrup, jam, glucose gel (such as Glucogel), or sugar dissolved in a little water, roughly a teaspoon, with a cotton bud or syringe (Bugbee et al., 2026; Caninsulin/MSD Animal Health UK). This works because sugar is absorbed straight across the lining of the mouth within a minute or two, so your pet does not need to swallow it (Caninsulin/MSD Animal Health UK).
Never pour liquid into a mouth that can't swallow, and never put your fingers into the mouth of a fitting or unconscious pet (Bugbee et al., 2026). Forced liquid can go down the wrong way into the lungs, causing a pneumonia that turns one emergency into two. The gum-rub avoids that entirely.
Then ring your vet and go in. A home rescue buys time, it does not end the event: the sugar is short-acting and the insulin that caused the low is still working, so your pet can dip again (Bugbee et al., 2026).
And the rule beneath all of this: you never, ever give more insulin to a pet you suspect is low. A hypo is too much insulin, not too little. More insulin is the opposite of the cure.
Catching it at the mild end
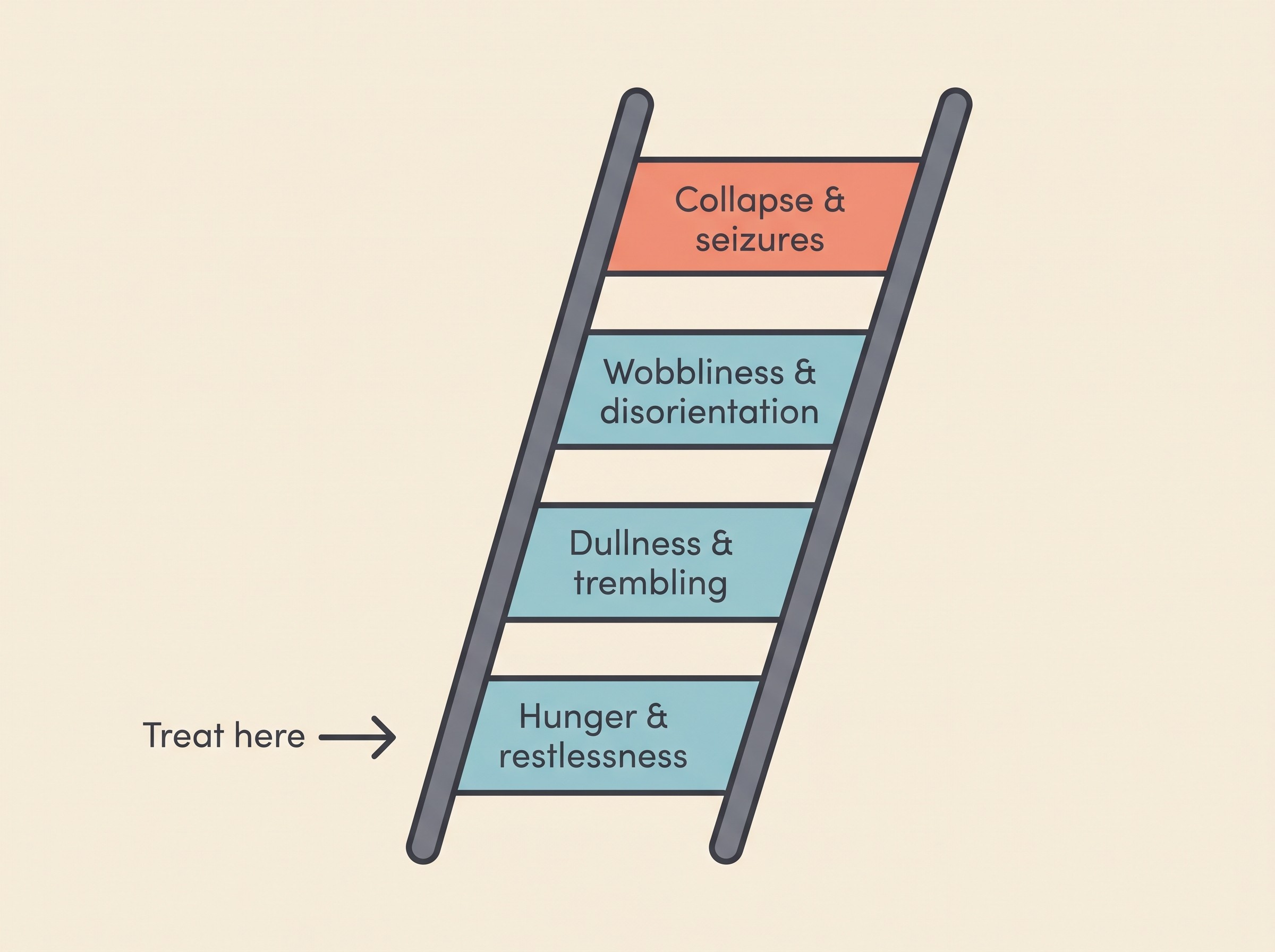
The skill that matters most here is spotting a hypo while it's still mild, before it becomes the dramatic end. The signs run along a ladder, and your job is the bottom rungs. Early: sudden hunger or scavenging, restlessness, a pet going quiet, dull, sleepy or "not themselves", and trembling. Moderate: weakness, a wobbly or drunken-looking walk, disorientation and muscle twitching. Severe: collapse, inability to stand, unresponsiveness, seizures and coma (Bugbee et al., 2026; Viebrock & Dennis, 2018). The shorthand I teach is simpler: wobbly, weak, dull, trembling, then collapse or seizures. See that end and you treat it as a hypo until proven otherwise.
Why does the early end matter so much? Because the data is sobering. In the best case series we have, 30 hypo presentations in cats, half were already in a stupor or coma by the time owners reached the clinic, so owners often don't notice until it's severe. Yet of the cats still responsive on arrival, 13 of 14 recovered neurologically within 12 hours, and prompt treatment made recovery far more likely (Viebrock & Dennis, 2018). Caught early, a hypo is very survivable, which is the whole reason to learn the mild signs now.
If you monitor at home, treat a reading below about 3.6 mmol/L (65 mg/dL) as "act", and below 3.3 mmol/L (60 mg/dL) as a marked, dangerous low (Viebrock & Dennis, 2018; Taylor et al., 2025). But don't wait for a number to give you permission: if your pet looks hypo and you can't measure quickly, treat. Sugar given to a pet that turns out fine does no harm; sugar withheld from one genuinely low can. One caveat: most human glucometers read a pet's blood lower than it really is, so an off-looking low on a human meter is worth confirming, never a reason to dose insulin.
What tips a pet into a low
A hypo is always a mismatch: more insulin working than there is glucose to balance it. Seen that way, the triggers make sense, and most are preventable.
A missed or reduced meal after insulin went in. The commonest trigger owners report: in the feline series, ten owners believed their cat had eaten less than usual on the day of the event (Viebrock & Dennis, 2018). The insulin went in expecting a meal that didn't fully arrive.
Vomiting after eating. The meal that should have balanced the dose comes back up. Three owners in that same series reported their cat vomited despite eating normally (Viebrock & Dennis, 2018), so a pet that vomits a meal it's just had insulin for is a reason to watch closely and ring your vet.
An accidental double dose. Two people in the house both injecting, a misread syringe, the wrong-strength syringe paired with the wrong insulin. Three owners in the series confirmed a double dose (Viebrock & Dennis, 2018), and the most dramatic case in the literature, a dog given ten times its dose, suffered cluster seizures from it (Park et al., 2023). Cats are especially vulnerable: diabetic cats, particularly overweight ones, are at greater risk of insulin overdose than dogs (Whitley et al., 1997).
Unusual or extra exercise. Working muscle pulls glucose out of the blood, so an unusually active day can tip a normally-fine dose into hypo territory: in dogs on insulin, interstitial glucose fell significantly for up to two hours after aerobic exercise (Mampe et al., 2025). Keep activity reasonably consistent, watch your pet for a couple of hours afterwards, and consider a small snack around heavy exercise.
Improving control, including a cat slipping into remission. This is the subtle one owners never see coming. As the diabetes settles and the same dose does more, it can quietly become too much: a hypo may occur with "unrecognized diabetic remission" (Bugbee et al., 2026), because good control rests the pancreas and lowers the body's own insulin need, so the injected dose becomes an overdose (Sparkes et al., 2015). This is one place dog and cat genuinely differ: a dog's diabetes is lifelong and won't remit, but a previously stable cat starting to have lows may be heading for remission, hopeful news that still needs an urgent vet call and a dose cut. The how-to belongs to the Stage 5 guides; here, just hold that getting better is itself a reason the dose may need to come down.
This is why it is safer to let a pet run a little high than to risk a low (Sparkes et al., 2015): glucose sitting consistently low-normal for several days is a prompt to talk to your vet about reducing the dose, not a target to celebrate (Taylor et al., 2025).
The golden rule, and the missed-dose trap
Almost every hypo I've treated traces back to a moment where someone gave insulin they shouldn't have. So the two rules below matter more than any technique.
Never increase or repeat an insulin dose on your own. The guideline is explicit: owners are empowered to decrease or skip a dose and seek help if they suspect a hypo, but must never increase the dose or its frequency without clear instructions from the vet (Bugbee et al., 2026). If the numbers look high, the answer is never "give a bit more and see", because chasing highs with extra insulin is exactly how you cause the low. An unseen low can even rebound into a high morning reading, a trap covered in Somogyi and dose-chasing; the short version is that a high number is never a reason to self-increase insulin.
If you're unsure whether a dose went in, skip it and wait for the next one. Your pet wriggled, you felt wet fur, you can't remember: whatever the doubt, do not "make it up" by injecting again. A missed dose is a minor, harmless blip; a double dose can be fatal. Wait until the next is due and carry on as normal, because a brief spell of high blood sugar is far less dangerous than a low from too much insulin (Caninsulin/MSD Animal Health UK). The "is it in?" mechanics live in your first insulin injection.
Once the danger has passed
A hypo doesn't end the moment your pet perks up, and treating it as "sorted" is a mistake I see often. Three things matter afterwards. Feed: once your pet is alert and can swallow safely, give a proper carbohydrate-containing meal, not just the dab of syrup that revived them, because the oral sugar is short-lived and the insulin is still active (Bugbee et al., 2026). Ring your vet, even if it resolved at home: the plan still needs reviewing, the dose almost always needs to come down, and a pet that collapsed or fitted needs assessing (Sparkes et al., 2015; Bugbee et al., 2026). Log it: the time, likely cause, signs, what you gave and how fast your pet responded. That record is what your vet needs to make the right dose change, and the Glucose Companion earns its keep here: its hypo flag and event log turn a frightening night into the data that prevents the next one.
It helps to know what waits at the vet's, because it makes the emergency feel survivable rather than hopeless. The team has tools you don't: intravenous glucose, and for stubborn lows an infusion of glucagon that raises blood sugar from another direction (Datte et al., 2016). The dog given ten times its dose was managed this way and discharged with no lasting neurological damage at all (Park et al., 2023). Even a serious overdose is very often survived when a pet reaches a vet promptly.
Building the safety net
Prevention is mostly habit, and the triggers above point straight to it: feed reliably before or with insulin, and treat any off-food, vomiting or unusually active day as a reason to check with your vet about that dose rather than giving it blind. Two extra habits earn their keep. Keep a fast sugar source, honey, golden syrup or glucose gel, where you inject and a second in your travel bag. And use a whiteboard, a log or the Glucose Companion so two people can't both dose the same pet, one of the easiest overdoses to make.
One last orientation: the two diabetic emergencies run in opposite directions. A hypo is too much insulin and too little sugar. Its mirror image, diabetic ketoacidosis, is too little insulin, and builds over hours to days rather than minutes; it has its own guide in diabetic ketoacidosis.
A hypo is the emergency to respect, but it's also the one you're most equipped to handle, because the rescue is sugar on the gums and a phone call, both within reach tonight. Keep it in proportion: the hazard is real, but it's the price of a treatment that genuinely works. Diabetes is a real commitment, not a death sentence, and treated pets live good lengths of life: UK figures put median survival for diabetic dogs who got past the first week of treatment at around 20 months, with untreated dogs faring far worse (Heeley et al., 2020). So stick the rescue card where you keep the insulin, make sure everyone who feeds your pet knows the wobbly-weak-dull signs and the never-give-more-insulin rule, and keep that jar of honey close. The owners who are ready for a hypo rarely have a bad one, and you just did the hard part by reading this before you needed it.
References
- Bugbee, A., Rucinsky, R., Alvarez, E., Cook, A., Lathan, P., & Panning, C. (2026). 2026 AAHA Diabetes Management Guidelines for Cats. Journal of the American Animal Hospital Association, 62(2), 65-93.
- Caninsulin / MSD Animal Health UK. (n.d.). Diabetes emergency and Diabetes FAQ (dog-owner guidance).
- Cornell University College of Veterinary Medicine, Riney Canine Health Center. (n.d.). Managing canine diabetes.
- Datte, K., Guillaumin, J., Barrett, S., Monnig, A., & Cooper, E. (2016). Retrospective evaluation of the use of glucagon infusion as adjunctive therapy for hypoglycemia in dogs: 9 cases (2005-2014). Journal of Veterinary Emergency and Critical Care, 26(6), 775-781.
- Heeley, A. M., O'Neill, D. G., Davison, L. J., Church, D. B., Corless, E. K., & Brodbelt, D. C. (2020). Diabetes mellitus in dogs attending UK primary-care practices: frequency, risk factors and survival. Canine Medicine and Genetics, 7, 6.
- Mampe, J. R., Stefanovski, D., & Hess, R. S. (2025). Aerobic exercise decreases interstitial glucose concentrations up to 2 h after exercise in dogs with insulin-treated diabetes mellitus: a preliminary study. Frontiers in Veterinary Science, 12, 1595952.
- Park, J.-H., An, J.-H., Kim, S.-H., Choi, H.-S., Kim, T.-H., Oh, Y.-I., Seo, K.-W., & Youn, H.-Y. (2023). Case report: Fatal insulin overdose in a dog with type 1 diabetes mellitus, characteristics and successful management. Frontiers in Veterinary Science, 10, 1255701.
- Sparkes, A. H., Cannon, M., Church, D., Fleeman, L., Harvey, A., Hoenig, M., Peterson, M. E., Reusch, C. E., Taylor, S., & Rosenberg, D. (2015). ISFM Consensus Guidelines on the Practical Management of Diabetes Mellitus in Cats. Journal of Feline Medicine and Surgery, 17(3), 235-250.
- Taylor, S., Cannon, M., Church, D., Fleeman, L., Fracassi, F., Gilor, C., Mott, J., & Niessen, S. (2025). 2025 iCatCare consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
- Viebrock, K. A., & Dennis, J. (2018). Hypoglycemic episodes in cats with diabetes mellitus: 30 cases (2013-2015). Journal of Feline Medicine and Surgery, 20(6), 563-570.
- Whitley, N. T., Drobatz, K. J., & Panciera, D. L. (1997). Insulin overdose in dogs and cats: 28 cases (1986-1993). Journal of the American Veterinary Medical Association, 211(3), 326-330.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine