Somogyi and Dose-Chasing: When More Insulin Is the Wrong Answer
Dr. Alastair Greenway
MRCVS
There's a logic that feels unarguable when you're holding the meter. The number is high. Insulin brings numbers down. So surely the answer is more insulin. I've watched careful, loving owners follow that thread into trouble, nudging the dose up week after week because the morning reading stays stubbornly high. It's the most intuitive move in the world, and one of the most dangerous instincts in diabetes care.
So let me say the headline plainly. A high glucose reading, on its own, is not a reason to give more insulin (Behrend et al., 2018). Sometimes a high number is the body's rebound from a low you never saw, and pushing the dose up then drives a deeper low and a bigger rebound. That trap has a name, the Somogyi effect, and a reputation far larger than it deserves: the rebound is real, but rare and badly over-diagnosed, and the lesson underneath it is bigger than Somogyi.
How the spiral runs
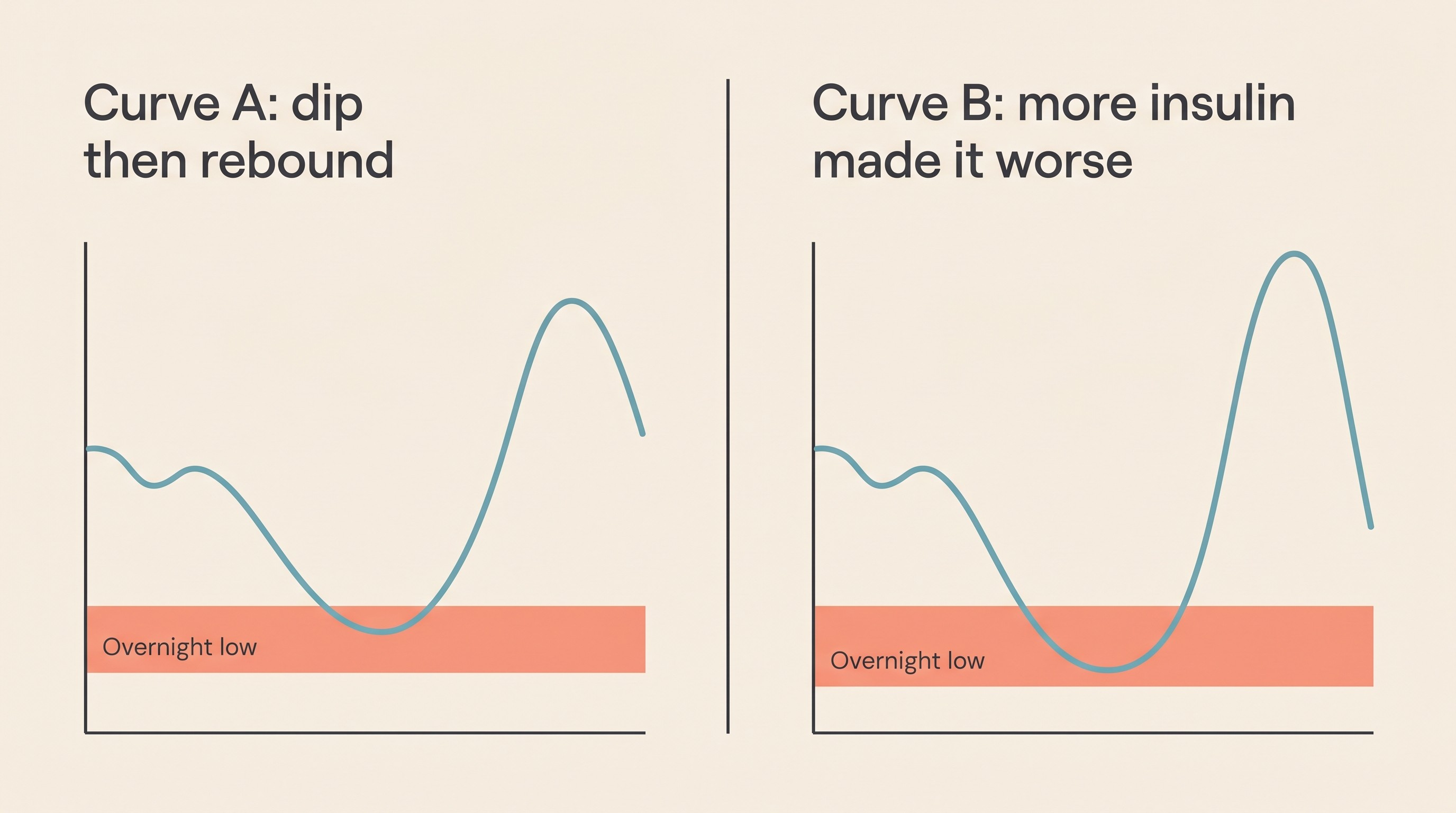
Picture how the spiral runs. Your pet's pre-breakfast glucose reads high, so the dose creeps up. That bigger dose pushes the glucose too low at some point in the day or, more often, in the small hours when nobody's watching. The body will not tolerate a dangerous low, so it fights back and overshoots, leaving a high number behind. You measure that high next morning, conclude the dose still isn't enough, and turn it up again. Round it goes, each loop adding insulin to a pet who is already, for part of the day, getting too much (Behrend et al., 2018; Della Maggiore, 2017). The cruel part is that you never see the low: the body catches it, so all you see is the high that follows, which looks exactly like under-treatment.
What the rebound actually is
The mechanism is real physiology, not folklore. When insulin drives blood glucose too low, or down too fast, the body releases a wave of counterregulatory hormones, chiefly cortisol, adrenaline and glucagon, which raise glucose back up by squeezing stored sugar out of the liver, ramping up new production and making the tissues temporarily resistant to insulin (Behrend et al., 2018; Della Maggiore, 2017). The result is post-hypoglycaemic hyperglycaemia: a low, then an over-corrected high. The trigger is a nadir below about 60 mg/dL (roughly 3.3 mmol/L), or a steep, rapid fall (Behrend et al., 2018).
That surge is deceptive. Its effect lingers in the order of 24 to 72 hours after a significant low, so the high you measure this morning may be the echo of a low you missed yesterday (Della Maggiore, 2017). And until the lowest point of the day climbs back above about 80 mg/dL (4.4 mmol/L), counterregulation muddies the picture so badly that you can no longer read the insulin's true duration from the curve (Behrend et al., 2018).
Real, but rare and over-diagnosed
Read the older texts and the forums and you'd think Somogyi was behind every awkward morning high; the modern evidence says the opposite. Researchers reviewed 10,767 blood glucose curves from 55 diabetic cats on glargine (Lantus), managed for tight control. Despite frequent biochemical hypoglycaemia across that enormous sample, curves consistent with rebound hyperglycaemia made up just 0.42% of the total, and the classic textbook picture, a rebound with a wave of insulin resistance behind it, was confined to four isolated events in four cats (Roomp & Rand, 2016). The authors' conclusion is the line every owner should hold: in glargine-treated cats, do not reduce, or chase upward, the insulin dose for a high reading without biochemical or clinical evidence of a low (Roomp & Rand, 2016).
The human evidence, where this has been studied longest, points the same way. In 88 people with type 1 diabetes monitored continuously, nocturnal hypoglycaemia was linked to morning hypo-glycaemia, not hyperglycaemia, and strongly so (odds ratio 3.95), the exact reverse of what the Somogyi model predicts (Guillod et al., 2007). The classic effect in people is now considered controversial and largely unproven, disputed by exactly this kind of monitoring; most morning highs are put down not to rebound but to the dawn phenomenon, a waning of overnight insulin and a normal morning hormone surge that lifts glucose without any preceding low (Rhea et al., StatPearls). The dawn phenomenon is common, true rebound is not, and the two are endlessly confused.
None of this means rebound never happens, and when it does it carries a message worth hearing. In a separate group of diabetic cats, post-hypoglycaemic hyperglycaemia occurred in about a quarter (33 of 133) of those that became hypoglycaemic, but tellingly not in healthy cats, whose physiology corrected the low cleanly (Zini et al., 2018). And the cats who rebounded were the ones in trouble: higher insulin doses (1.09 versus 0.65 IU/kg), higher fructosamine, far lower remission (10% versus 56%) and greater glycaemic variability (Zini et al., 2018). Read that the right way round: rebound clusters at the over-dosed, poorly controlled end, so it flags a pet getting too much insulin, not one needing more. Where it appears, it argues for stepping back, not pressing on.
Spotting it, and why one number lies
The fingerprint of rebound is specific: a documented low, then a high on the same trace, most often an unseen overnight dip surfacing as a puzzling morning or pre-dose high (Della Maggiore, 2017; Behrend et al., 2018). A suggestive history can be cyclic control, a day or two of lovely numbers then several poor ones, but history is only a flag: the diagnosis lives in the curve, never in a hunch (Della Maggiore, 2017).
This is exactly why a single reading cannot drive a dose change. The guidelines are blunt: a spot glucose value on its own is not a sound reason to increase insulin, though a verified one can sometimes justify a decrease (Behrend et al., 2018). On one spot check, rebound, genuine under-dosing and a short-acting insulin running out all read high and look identical, and in cats stress hyperglycaemia adds a fourth, a frightened cat reading sky-high in the clinic on a perfectly sensible dose (Behrend et al., 2018). One high number can mean several things, some of which call for less insulin.
The instrument that settles the question is a glucose curve, and better still a continuous glucose monitor. A CGM such as the FreeStyle Libre (used off-label in pets) records every few minutes for up to a couple of weeks, so it catches the unseen overnight nadir a 12-hour clinic curve sails straight past, the very evidence that separates real rebound from simple under-treatment (Behrend et al., 2018). One caveat: the Libre is least accurate at the bottom of the range, reading low across most of the hypo-to-normal band yet sometimes high in marked hypoglycaemia below about 55 mg/dL, so confirm a suspected critical low and treat the pet, not the dot on the screen (Tardo et al., 2025). The detail belongs to reading a glucose curve and the continuous glucose monitor guide; here, it's simply the only reliable way to know whether a low came first.
Why the fix is often less, and why it's your vet's call
When a genuine Somogyi rebound is suspected or proven, the counterintuitive answer is to reduce the insulin and assess the response over days, not hours. The usual step is a cut of roughly a quarter, or about half if there were clear signs of a low, never another increase (Behrend et al., 2018). And here is why signs alone can't guide you: an over-dosed, rebounding pet can look just as clinical as an under-dosed one, thirsty, weeing buckets, ravenous and losing weight. Too much insulin and too little can look identical, which is exactly why you never push the dose up on symptoms (Behrend et al., 2018).
There's a clear ceiling on the chase, too. The guidelines are explicit that you should not increase the dose more than two or three times without stepping back to consider Somogyi or true resistance (Behrend et al., 2018). The canine side rhymes with that: frequent dose changes and large increments are themselves risk factors for provoking a rebound, and a pet above roughly 1.5 U/kg and still poorly controlled warrants reassessment, often downward (Della Maggiore, 2017). Small, infrequent, vet-led changes are the antidote to dose-chasing, and how titration works is owned by insulin dose titration. If your pet truly seems to need ever-larger doses, the answer is far more often dull and findable than a rebound, a story for the insulin resistance work-up.
One rule that survives the controversy
The most useful instruction here doesn't depend on whether any given high is "really" Somogyi. Whether the morning number is rebound, dawn phenomenon, a stressed cat or plain under-treatment, the same discipline holds: react to trends and to a verified low, never to a single high, and never adjust insulin on your own. That guardrail is true regardless of the mechanism, so it outlasts the debate.
One safety note belongs here. A wobbly, weak, dull, trembling or collapsing diabetic may be hypoglycaemic: rub glucose, honey or sugar onto the gums (never pour liquid into a mouth that can't swallow) and get to a vet straight away. Never re-dose into a pet you suspect is low, and never double-dose to "catch up" a high. Not sure a dose went in? Skip it and wait. A missed dose is far safer than a double. The full rescue and aftercare are owned by the hypoglycaemia emergency guide.
One last point, because dog and cat are two different diseases. The rebound and remission data above are feline; remission is a cat story you should never read onto a dog, who stays insulin-dependent for life (Behrend et al., 2018; Della Maggiore, 2017). In dogs, Somogyi is described the same way but is likewise not the usual reason a diabetic is difficult: handling and injection technique, too-short insulin duration and concurrent disease are far commoner (Della Maggiore, 2017).
So if you're standing in the kitchen at seven in the morning, frustrated by another high reading and tempted to turn the dial, the most powerful thing you can do is the opposite of the obvious. Don't add a unit. Capture the day instead. The Glucose Companion does precisely this job: log the doses, plot a curve or import a Libre trace, see the nadir with its hypo flag, and walk into your vet with the trend and the low it might be hiding. You've turned an anxious guess into a fact someone can act on, and it almost never starts with more insulin.
References
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Roomp, K., & Rand, J. S. (2016). Rebound hyperglycaemia in diabetic cats. Journal of Feline Medicine and Surgery, 18(8), 587-596.
- Zini, E., Salesov, E., Dupont, P., Moretto, L., Contiero, B., Lutz, T. A., & Reusch, C. E. (2018). Glucose concentrations after insulin-induced hypoglycemia and glycemic variability in healthy and diabetic cats. Journal of Veterinary Internal Medicine, 32(3), 978-985.
- Della Maggiore, A. (2017). Consider the Case: An Uncontrolled Diabetic Dog. Today's Veterinary Practice, March/April 2017.
- Guillod, L., Comte-Perret, S., Monbaron, D., Gaillard, R. C., & Ruiz, J. (2007). Nocturnal hypoglycaemias in type 1 diabetic patients: what can we learn with continuous glucose monitoring? Diabetes & Metabolism, 33(5), 360-365.
- Rhea, D., et al. Somogyi Phenomenon. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (incorporating Hirsch et al., 1990).
- Tardo, A. M., et al. (2025). Accuracy of the FreeStyle Libre 3 Continuous Glucose Monitoring System in Hypo- and Euglycemic Cats. Journal of Veterinary Internal Medicine, 39(2), e70048.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine