
How Insulin Dose Titration Works (and Why It Takes Weeks)
Claire Greenway
BVM&S MRCVS
There's a question I can almost set my watch by. About two or three weeks after a pet starts insulin, the owner rings, and somewhere in the first minute it comes out: "I don't think the dose is right yet." Often there's a flicker of failure underneath it, as though they were meant to have cracked this by now. So let me take that weight off you straight away. Your pet's diabetes is not supposed to be sorted in a fortnight. Getting to a good insulin dose is a slow, monitored process that genuinely takes weeks to months, and not being there yet is not a sign anything has gone wrong. It's a sign the process is working.
This article is about the dose decision itself: why finding the right amount is gradual, what your vet adjusts it on, how big the steps are, and the one rule that keeps it safe. Collecting the readings lives in home blood glucose monitoring, and reading a curve's shape is its own skill in reading a glucose curve. If you're only days in, the first weeks on insulin is the gentler predecessor.
Why faster isn't better
Insulin isn't like a painkiller you take and judge an hour later. The intermediate and longer-acting insulins we use in pets, Caninsulin (Vetsulin in the US) in dogs, ProZinc or glargine (Lantus) in cats, reach a steady, predictable glucose-lowering effect only after the body has had several doses to settle around the new amount, so a dose has to be judged over days, not hours. The published figures are blunt. The UK manufacturer guidance for Caninsulin states plainly that "achieving stabilisation may take time (up to 6 months)" (Caninsulin dosing overview, MSD, 2024), and reaching the ideal dose in dogs typically takes anything from four to eight weeks (Nelson, WSAVA/VIN). Most dogs and cats take weeks to months to stabilise, so good control within the first few weeks is genuinely unlikely (Behrend et al., 2018). That is the normal timeline, not a measure of how well you're doing.
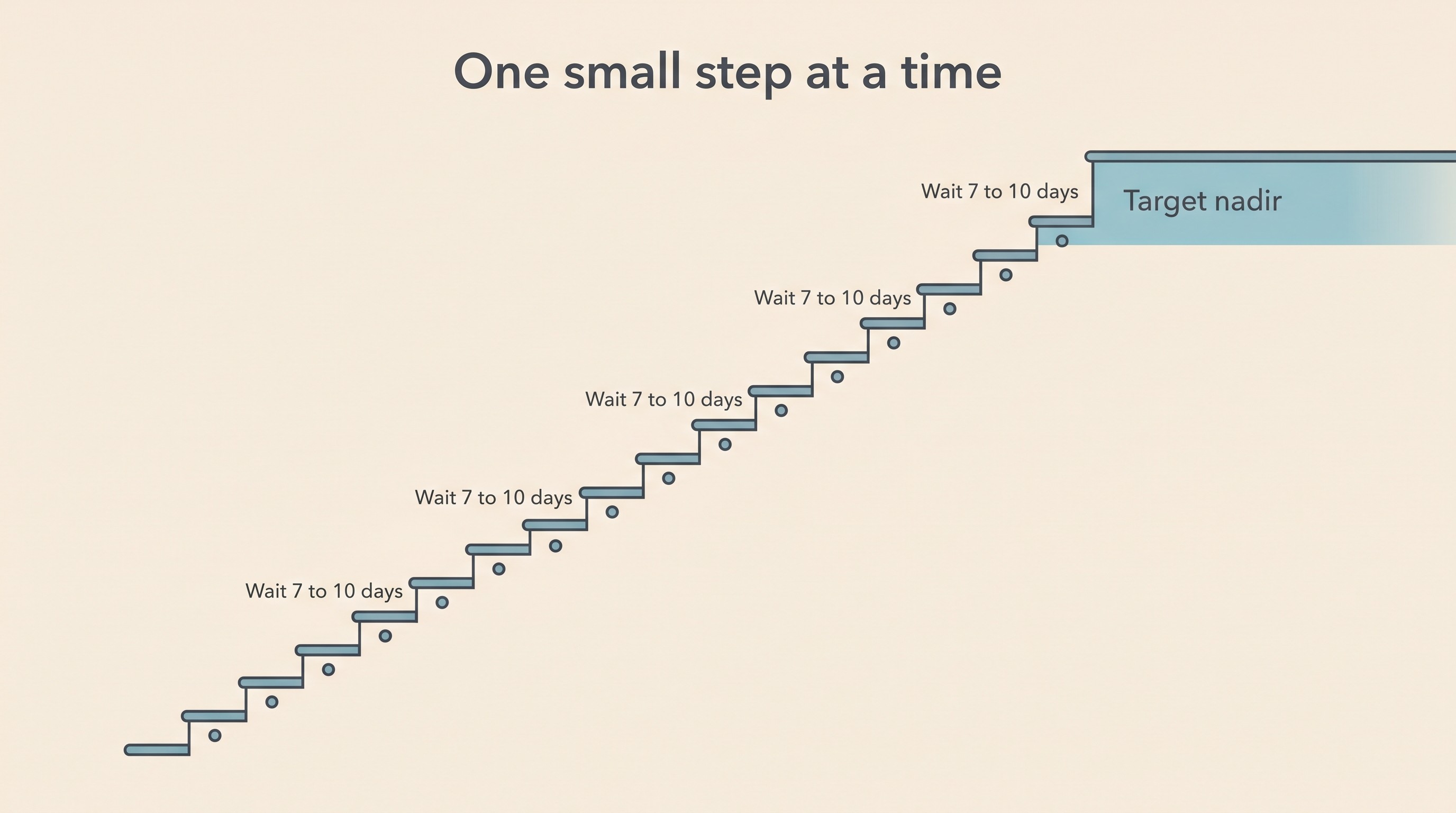
So when a dose looks like it "isn't working" at two weeks, the commonest explanation is simply that it hasn't been given long enough at the current step, and changing it sooner is the wrong move. The manufacturer guidance puts numbers on it: during stabilisation, changes "should not normally be made more frequently than every 3 days (ideally around 7-10 days)," and you wait until a new dose has run for at least three days before re-evaluating, unless signs of a hypo appear (Caninsulin dosing overview, MSD, 2024). Other canine guidance is firmer still: don't change the dose by more than 25% at a time, nor more often than weekly (Nelson, WSAVA/VIN).
This isn't bureaucratic caution. Adjusting too often actively destabilises the pet, because frequent changes raise the risk of the Somogyi response, the rebound where an unseen low triggers the body to push glucose high again (Behrend et al., 2018), covered in Somogyi and dose-chasing. So changing the dose every day or two doesn't speed things up; it can manufacture the very high readings that tempt you into another increase, and you end up chasing your own tail.
What goes into a dose change
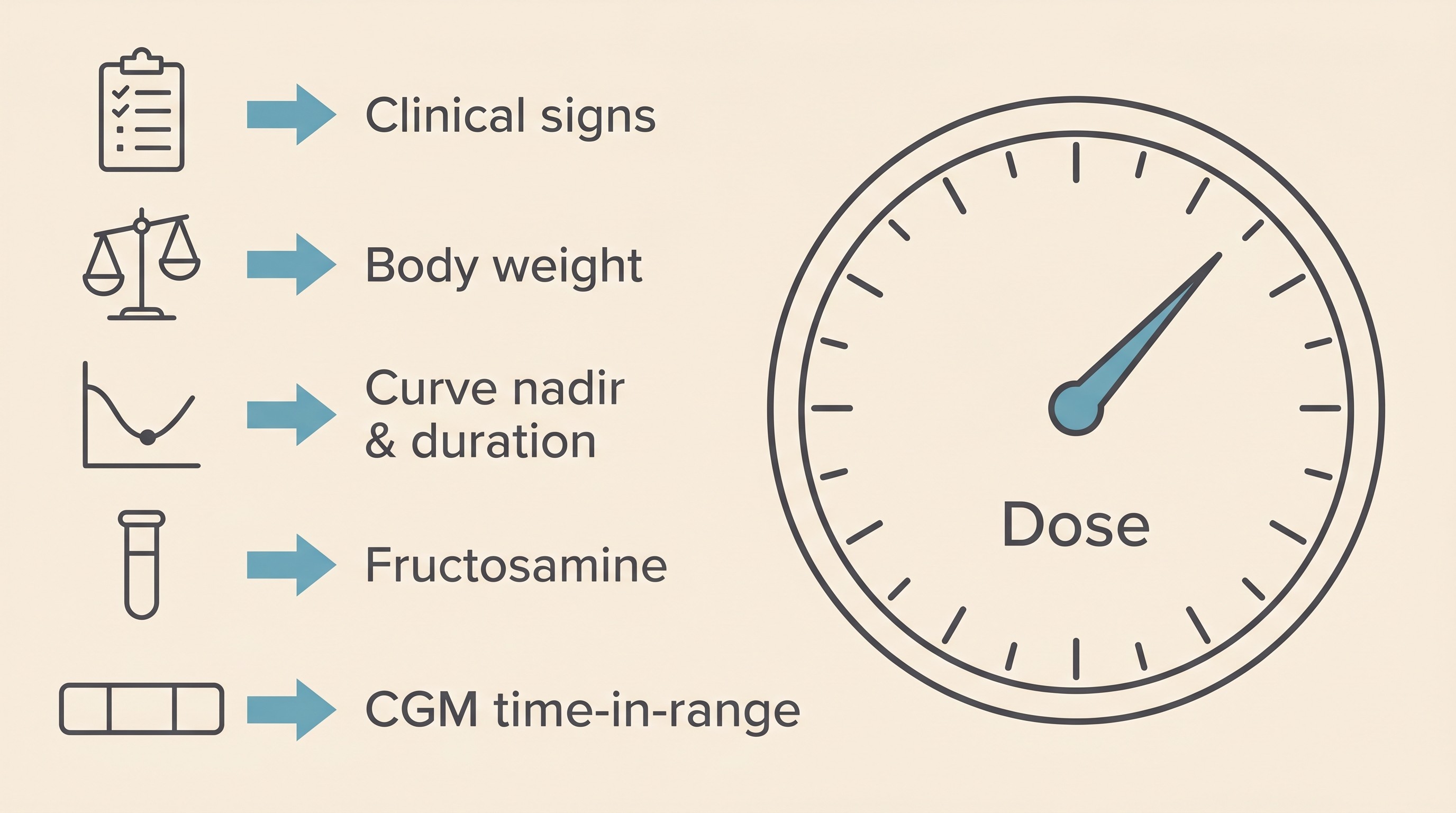
The dose is not steered by glucose numbers alone, and never by a single one. AAHA's central message reframes what "success" even means: clinical signs supersede all else, and when a pet has no clinical signs and a body weight that's steady or rising, the diabetes is likely well controlled (Behrend et al., 2018). So the first things your vet weighs are the everyday ones you see at home: is the thirst settling, has the constant weeing eased, is the appetite normal, the weight stable, the pet bright again. This is why your home log of signs, not just glucose, matters so much, and why "the number was high once" is not, by itself, a reason to give more.
On top of that sit the glucose data. The key number a dose is titrated to is the nadir, the lowest glucose reached after a dose, and it is steered toward a safe target window: for dogs on Caninsulin, a nadir between roughly 5.5 and 8.5 mmol/l (Caninsulin dosing overview, MSD, 2024); for cats, a glucose that troughs near-normal, around 4.5 to 5.5, and peaks at 14 to 19 (Taylor et al., 2025). The vet raises the dose if the nadir runs too high and lowers it if it dips too low (Nelson, WSAVA/VIN). What a curve actually looks like, and the cat-specific stress trap where a frightened cat reads falsely high, belongs to reading a glucose curve.
Then there's fructosamine, a blood test reflecting average glucose over the preceding two to three weeks, one more input immune to a single bad-day spike, with its timing in fructosamine and the rechecks. AAHA is firm that the only reliable way to know how to change a dose is to run a glucose curve and to make small, infrequent changes that you allow time to assess, the safest guard against an accidental overdose (Behrend et al., 2018). No single reading moves the dose; the pattern does.
Step size, and the data behind it
Insulin's margin for error is narrow, so the steps are small and rule-bound by design. In dogs, changes are typically around 10% per adjustment (Caninsulin dosing overview, MSD, 2024) and should not exceed 25% (Nelson, WSAVA/VIN), often about 1 unit. In cats, stepwise increases of around 1 unit may be needed, especially with insulin resistance (Taylor et al., 2025), and owner-led protocols for newly diagnosed cats use even finer 0.5 IU steps (Gottlieb et al., 2024). This is also why the first dose felt so low: vets deliberately start from a safe floor and build up, the "start low, go slow" principle, because briefly under-dosing is far safer than over-dosing (Behrend et al., 2018).
Modern monitoring has changed how well this works. Continuous glucose monitors, the FreeStyle Libre-type sensors, show trends across whole days rather than one in-clinic snapshot, so the 2025 feline consensus now recommends one be worn continuously to guide titration from diagnosis until the cat stabilises or remits (Taylor et al., 2025). In dogs, a sensor-guided glargine protocol reached glycaemic control in a median of just 16 days, but only because patients were monitored with a sensor from the start (Tardo et al., 2024), and time-in-range, the share of the day glucose spends in a sensible band, tracks clinical control better than any single reading (Del Baldo et al., 2025). Sensor mechanics belong to the CGM article; for titration, the point is just that good data makes good dosing possible. One caveat: a human glucometer reads pet blood low, so a pet-calibrated meter or sensor gives numbers your vet can trust. Whatever you log in the Glucose Companion becomes the trend your vet titrates on.
The one rule, and a real exception
You do not self-adjust insulin off a single reading or a hunch: changes are made with your vet, on a plan you've agreed together, because reacting to one high number by giving more insulin is one of the surest ways a pet gets hurt. And if you're ever unsure whether a dose actually went in, the safe default is to skip it and wait for the next one: a missed dose is far safer than a double, every time. Never give extra to "make up" for one you're unsure about, and never re-dose into a pet you suspect is going low. (A wobbly, weak, dull or trembling diabetic may be having a hypo: an emergency with its own rescue, sugar on the gums then vet now, set out in the hypoglycaemia guide.)
Now the exception, because you'll read about it and deserve the truth. There are real, evidence-based protocols in which owners adjust insulin from home readings, and they work. But look at how they run: owners adjust based on pre-insulin glucose measurements they take at home, following a written protocol provided to them, with veterinary guidance always available (Gottlieb et al., 2024). That is a vet's set of written rules with monitoring behind it, not solo dosing off a forum thread or a one-off high. And there's a reason even those steps stay small and spaced rather than aggressive: tight control raises the risk of a hypo, and the intensive feline protocols got their excellent results only with such close home monitoring that just one mild clinical hypo occurred across an entire study (Roomp & Rand, 2009). The killer risk here is the low, not the high, and a slightly-high-but-safe pet beats a perfect number bought with a hypo every single time.
Where this is heading
"Well controlled" does not mean textbook-perfect glucose. AAHA tells vets to rethink the goals of therapy: achieving specific numbers should not be the aim, and a controlled diabetic is simply one whose clinical signs have resolved while avoiding hypoglycaemia (Behrend et al., 2018). The feline consensus adds that micromanagement should be avoided, and every step should serve a good quality of life for the cat and the caregiver alike (Taylor et al., 2025). A happy, comfortable pet whose signs have settled is the goal, the fuller picture of which is in what good control actually looks like. For cats there's an extra incentive to dial the dose in promptly, because early good control is tied to far higher remission rates (Roomp & Rand, 2009), the story told in feline diabetic remission. For dogs, remission isn't on the table, but a long, well-managed life very much is.
Getting there is a marathon of small, monitored steps, and the data you bring is what moves it along. Keep logging in the Glucose Companion, bring the trend to each recheck, and when you're ready to read what it's telling you, reading a glucose curve is the next thing to learn. You're not behind. This is just meant to take time.
References
- Behrend E, Holford A, Lathan P, Rucinsky R, Schulman R. 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2018;54(1):1-21.
- Caninsulin dosing overview. MSD Animal Health (UK professional resource). Diabetes in Dogs: Dosing Overview. 2024.
- Taylor S, Cannon M, Church D, Fleeman L, Fracassi F, Gilor C, Mott J, Niessen S. iCatCare 2025 consensus guidelines on the diagnosis and management of diabetes mellitus in cats. J Feline Med Surg. 2025;27(11):1098612X251399103.
- Tardo AM, Fleeman LM, Fracassi F, Berg AS, Guarino AL, Gilor C. A dose titration protocol for once-daily insulin glargine 300 U/mL for the treatment of diabetes mellitus in dogs. J Vet Intern Med. 2024;38(4):2120-2128.
- Del Baldo F, Tardo AM, Gilor C, Mott J, Da Vela C, Pergolese V, Fracassi F. FreeStyle Libre-derived metrics in assessing glycemic control in diabetic dogs. J Vet Intern Med. 2025;39(4):e70151.
- Roomp K, Rand J. Intensive blood glucose control is safe and effective in diabetic cats using home monitoring and treatment with glargine. J Feline Med Surg. 2009;11(8):668-682.
- Gottlieb S, Rand JS, Anderson ST. Frequency of diabetic remission, predictors of remission and survival in cats using a low-cost, moderate-intensity, home-monitoring protocol and twice-daily glargine. J Feline Med Surg. 2024;26(4):1098612X241232546.
- Nelson RW. Canine Diabetes Mellitus. WSAVA Congress proceedings (VIN).
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine