
What "Good Control" Actually Looks Like (and Why It Isn't Perfect Numbers)
Claire Greenway
BVM&S MRCVS
There's a particular worry I see in diabetic pet owners a few months in. The injections are happening, the pet seems well, and yet the owner is anxious, because they've been checking glucose at home, or reading a forum, and the numbers aren't "normal." Their own blood sugar would sit around 5 mmol/L. Their dog's morning reading was 12. So they lie awake convinced they're failing, and the temptation forms to nudge the dose up, just a little, to get the number down.
I want to take that worry off you, because it rests on a misunderstanding that the language of human diabetes quietly pushes onto us. A perfect, textbook-normal blood glucose was never the goal for your pet. It isn't what we aim for, it isn't what success looks like, and chasing it is dangerous. Good control is kinder and far more reachable than that, and once you can see it clearly you can stop grading the meter and start enjoying a well animal again.
What success actually means
The 2018 AAHA diabetes guidelines define a controlled diabetic in terms of exactly two things, and a normal glucose is not one of them. The aim is "decreasing the clinical signs of DM while avoiding hypoglycaemia, the two conditions that represent the definition of a controlled diabetic" (Behrend et al., 2018). That's it. Are the symptoms settling, and is the pet safe from dangerous lows? Resolve those two and your pet is, by definition, controlled, whatever the meter says on a given morning. The canine literature is blunter still: practitioners "should not strive for perfect blood glucose control; rather, the goal should be good clinical control" (Ward, 2019), and the current feline consensus insists "assessment of clinical signs must be prioritised in any monitoring strategy" (Taylor et al., 2025).
There's a deeper reason for this than bedside manner. How your pet looks and behaves often reflects their true glucose control better than the lab does. Owner-reported clinical signs "have been shown to provide information that often reflects the patient's true state of glycaemic control better than most biochemical analyses" (Bugbee & Fujishiro), and "for many patients, these factors are more predictive of diabetic control than glucose measurements" (Ward, 2019). You, watching your pet over breakfast, hold the most predictive information there is. We treat the pet, not the spreadsheet.
Five signs your pet is doing well
So if the number isn't the scorecard, what is? Here is the checklist that actually tells you your pet's diabetes is well controlled:
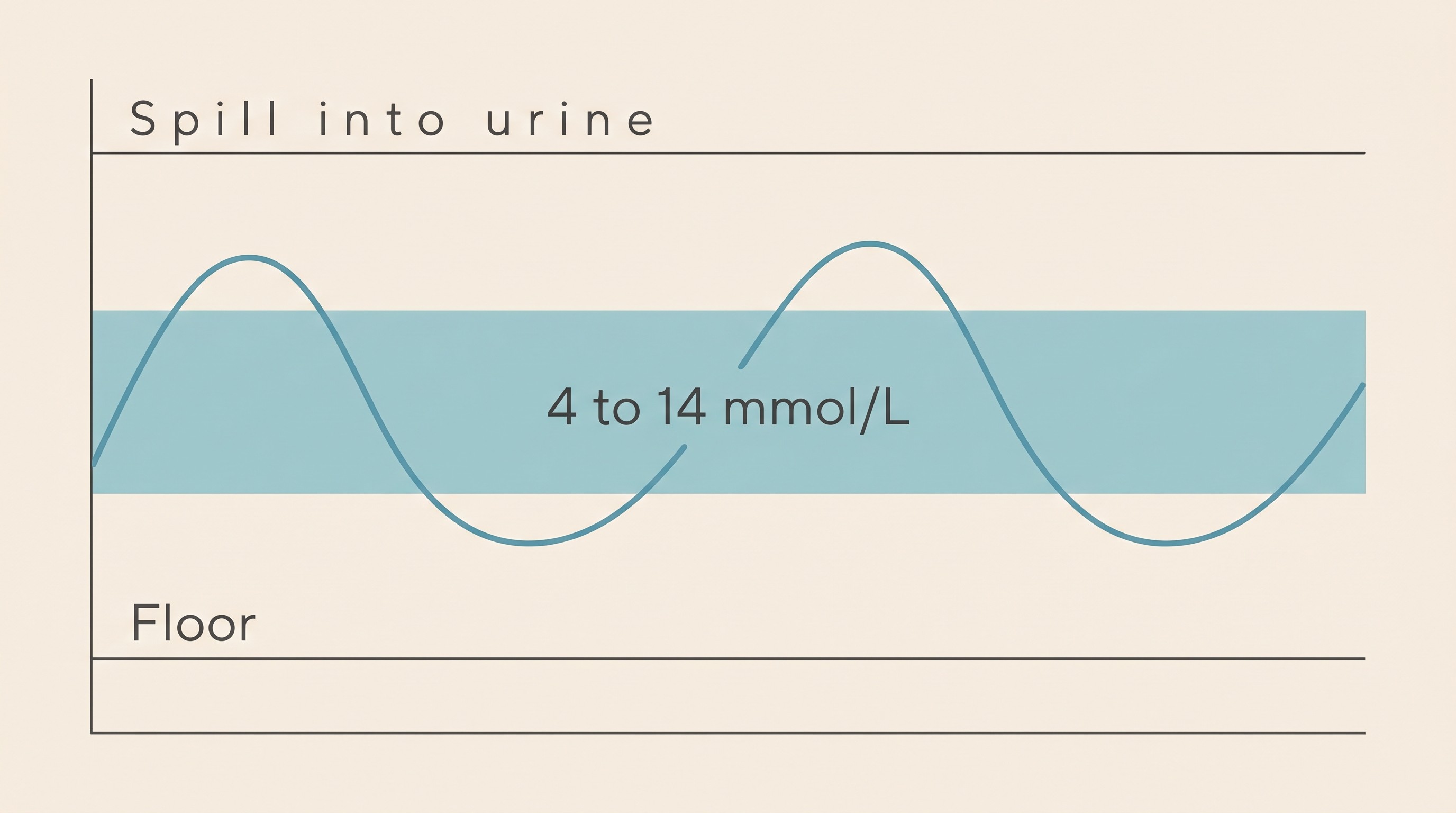
- Normal thirst and weeing. The relentless thirst and the puddles or overflowing litter tray have settled back to ordinary. This is usually the first thing owners notice lifting, and a reliable sign glucose is staying mostly below the level where it spills into urine and drags water with it.
- A stable, healthy weight. The frightening weight loss has stopped, and a thin pet is filling back out toward where they should be. A steady weight at rechecks is one of the clearest signals things are working (Behrend et al., 2018).
- A normal appetite, eating with interest, not the desperate, never-satisfied hunger of an uncontrolled diabetic whose cells are starving in a sea of unusable glucose.
- Good energy and a good coat, bright and comfortable, back to their normal selves. A dull, flat, scurfy-coated animal is telling you something the meter might not.
- No hypoglycaemic episodes: no wobbliness, weakness, dullness, trembling or collapse. This half of the definition matters every bit as much as the symptoms easing (Behrend et al., 2018; Ward, 2019; Taylor et al., 2025).
I'm giving you the checklist rather than the method on purpose. How to measure each of these properly, weighing your pet the same way each week, working out water intake in millilitres per kilo, watching the litter tray with a clinician's eye, belongs in what to watch at home. You're grading the animal, and these five things are the report card.
A modest band, kept off the floor
"But surely there's a number," I hear you think. There is a target range, and it reveals the whole philosophy: we deliberately run your pet a little sweet.
For cats, the consensus describes the aim as glucose "that ranges from normal (4.5 to 5.5 mmol/L, 80 to 100 mg/dL) at its lowest to 14 to 19 mmol/L (250 to 350 mg/dL) at the peak," with readings "in the range of 5 to 20 mmol/L (90 to 360 mg/dL) typically associated with good clinical control" (Taylor et al., 2025). The feline practice literature agrees, putting the low around 5.6 mmol/L (100 mg/dL) and the day's range at roughly 5.6 to 16.7 mmol/L (100 to 300 mg/dL) (Bugbee & Fujishiro). Look at the top of those ranges. We are content for a controlled diabetic to spend part of the day up at 14, 16, even 19 mmol/L, because the symptoms only really kick off once glucose climbs above the kidney's threshold for spilling into urine, around 14 to 16 mmol/L (250 to 290 mg/dL in cats) (Bugbee & Fujishiro). Keep most of the day under that ceiling and the thirst, weeing and weight loss melt away. Reaching instead for a flat, non-diabetic 4 to 6 mmol/L would mean running them so close to empty that any small thing tips them into a hypo.
And here is the line from the feline consensus that ought to lift the weight off you: "evidence that any particular glycaemic target is associated with any particular outcome is lacking" (Taylor et al., 2025). After decades of research, nobody has shown that a tighter, prettier number buys your pet a better or longer life. What we do know, with certainty, is that chasing one buys hypoglycaemia.
Never trade a hypo for a tighter number
A single high reading is not an emergency. Hypoglycaemia is. The closer you push glucose toward normal, the higher the risk of overshooting into a low, and a low is the acute danger in a diabetic's life, the one that can cause collapse or seizures within an hour. The guidelines bake the trade-off straight into the goal: aim for the best clinical control "without an unacceptably high risk of hypoglycaemia" (Taylor et al., 2025). Avoiding hypos isn't a footnote to good control. It is, quite literally, half the definition of it (Behrend et al., 2018).
So let this rule overrule every forum instinct: you never push the dose up to chase a high number, and you never adjust off a single reading. React to the trend and to how your pet is, never to one figure on one morning. If anything, the readings that should make you ring the vet are the low ones, which is exactly what the Glucose Companion's hypo flag is there to catch. The hypo itself, how to spot it and the gums-and-glucose rescue that can save a life, is owned by the hypoglycaemia emergency guide, the one piece I'd ask every owner to read and keep to hand. When a dose genuinely does need changing, how dose titration works covers the careful, vet-led way. Good control means you can mostly stop fiddling.
Time-in-Range: more good hours, not a flat line
If you've moved to a continuous sensor, you'll have met a more humane way of reading control: Time-in-Range. Instead of judging one nadir off one stressful curve, it asks a gentler question, what fraction of the whole day did glucose spend in a sensible band? In a study of 85 diabetic dogs, Time-in-Range was the percentage of the day glucose sat between 3.9 and 13.9 mmol/L (70 to 250 mg/dL), and a higher Time-in-Range tracked with genuinely better clinical control, correlating with the validated clinical-signs score vets now use (Del Baldo et al., 2025).
But hold on to one figure above all, because it dismantles the perfectionism in one stroke. The dogs with optimal control spent a median of just 49.5% of the day in range, against 35.0% for the suboptimal dogs (Del Baldo et al., 2025). Even brilliantly controlled diabetic dogs spend only about half the day in the ideal band. Good control was never meant to be 100% perfect numbers. It is more time in a sensible range than not, fewer dangerous lows, and a well pet to show for it. If you've been holding your pet to a standard that even the best-controlled animals in the research don't meet, you can let that go tonight.
Formal Time-in-Range targets for cats aren't standardised yet, so for a cat we still lean on that sensible daily-excursion picture from earlier (Taylor et al., 2025). The sensor itself, and the art of reading a curve's shape, live in the CGM guide and reading a glucose curve; here I just want the concept to land: aim for more good hours, not a flat line.
And mind the trap on the other side, the one the "lower is better" instinct walks straight into. A reading that looks beautifully low, or a fructosamine bang in the middle of the normal range, is not a prize. In an insulin-treated pet it can mean time spent hypoglycaemic or over-dosing, and in a cat it can be the first quiet sign of remission, the point at which the dose may need reducing (Taylor et al., 2025). So an unexpectedly good number is a reason to talk to your vet, not to relax: the fructosamine detail is fructosamine and the vet rechecks, the cat remission story feline diabetic remission. This is where the two diseases part company. A dog is insulin-dependent for life, so good control is the steady, permanent good state you settle into; a cat in lovely control may be heading off insulin altogether. One technical caveat if you check at home: a human glucometer reads pet blood falsely low, so trust a pet-calibrated meter or a sensor over a worrying low.
What all this effort is for
Step back from the meter and look at what all this effort is really for. Good control buys a good life, and that's data, not a platitude. In a study of diabetic cats, 97% of owners (140 of 144) whose cat was alive at the survey rated its quality of life as excellent or good (Rothlin-Zachrisson et al., 2023). In dogs, median survival from diagnosis was around 964 days, with the authors concluding that "diabetic dogs have a good life expectancy" (Tardo et al., 2019). The fuller outlook conversation belongs in is this a death sentence. Control also quietly heads off trouble over the years, fewer infections and a lower risk of the diabetic emergency, and in dogs it slows the cataracts that around 80% will develop within roughly sixteen months of diagnosis (Beam et al., 1999), all mapped in preventing complications.
Good enough protects you too. Diabetes is a real burden on the person at the syringe: the validated owner quality-of-life tool found 84% of dog owners reported a negative impact on their own quality of life, with worry about hypoglycaemia and worry about blindness among the heaviest of those burdens (Niessen et al., 2012; Niessen et al., 2010). The consensus draws the obvious conclusion: "micromanagement should be avoided and all management steps should serve the ultimate treatment outcome of a good quality of life for cat and caregiver alike" (Taylor et al., 2025). A regimen you can live with, that doesn't have you checking numbers at midnight and dreading every meal, is not a compromise. It is the goal, for the pet and for you.
So once the signs have settled and the weight is steady, the most clinically correct thing you can often do is leave the dose alone, even when a number looks high (Behrend et al., 2018), let the rechecks stretch from weekly to every few months, and let the diabetes recede into the background of an ordinary, well life. Keep logging your readings and sensor traces in the Glucose Companion and watch the trend settle, not so you can chase it, but so you can see the proof of what's already working and hand a clean report to your vet. The win you're aiming for isn't a flawless graph. It's the recheck where your vet feels your bright, steady-weighted, normally-drinking pet, looks at the trend, and says the best four words in diabetes management: carry on as you are.
References
- Behrend E, Holford A, Lathan P, Rucinsky R, Schulman R. 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association. 2018;54(1):1-21.
- Taylor S, Cannon M, Church D, Fleeman L, Fracassi F, Gilor C, Mott J, Niessen S. 2025 iCatCare consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery. 2025;27(11):1098612X251399103.
- Ward CR. Treating and Managing Diabetes Mellitus in Dogs. Today's Veterinary Practice. 2019 (Nov/Dec).
- Bugbee A, Fujishiro M. Managing Feline Diabetes Mellitus. Today's Veterinary Practice.
- Del Baldo F, Tardo AM, Gilor C, et al. Freestyle Libre-Derived Metrics in Assessing Glycemic Control in Diabetic Dogs. Journal of Veterinary Internal Medicine. 2025;39(4):e70151.
- Rothlin-Zachrisson N, Öhlund M, Röcklinsberg H, Ström Holst B. Survival, remission, and quality of life in diabetic cats. Journal of Veterinary Internal Medicine. 2023;37(1):58-69.
- Niessen SJM, Powney S, Guitian J, Niessen APM, Pion PD, Shaw JAM, Church DB. Evaluation of a quality-of-life tool for dogs with diabetes mellitus. Journal of Veterinary Internal Medicine. 2012;26(4):953-961.
- Niessen SJM, Powney S, Guitian J, Niessen APM, Pion PD, Shaw JAM, Church DB. Evaluation of a quality-of-life tool for cats with diabetes mellitus. Journal of Veterinary Internal Medicine. 2010;24(5):1098-1105.
- Tardo AM, Del Baldo F, Dondi F, Pietra M, Chiocchetti R, Fracassi F. Survival estimates and outcome predictors in dogs with newly diagnosed diabetes mellitus treated in a veterinary teaching hospital. Veterinary Record. 2019;185(22):692.
- Beam S, Correa MT, Davidson MG. A retrospective-cohort study on the development of cataracts in dogs with diabetes mellitus: 200 cases. Veterinary Ophthalmology. 1999;2(3):169-172.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine