What Good Control Buys: Heading Off the Complications
Dr. Alastair Greenway
MRCVS
There comes a point, usually a few weeks in, when the injections and the meals and the logging stop being terrifying and turn into a chore. The fear fades, and what's left is the grind: two needles a day, every day, seemingly forever, for a pet who looks, frankly, fine. And a quiet question surfaces. Is all of this actually doing anything?
It is. The daily effort isn't busywork, and it isn't a vague "it's good for them." It's buying your pet something specific: fewer crises, slower and fewer complications, and more good years. This article is the map of what you're heading off. It gives you the overview rather than cataloguing every complication in frightening detail, because the dedicated guides do that better, and it covers the one almost nobody else explains well, the dropped-hocks stance in cats.
Setting the bar: what "control" actually means
Let me set the bar plainly first, because if you aim at the wrong target you'll exhaust yourself and put your pet in real danger. Good control does not mean perfect, textbook-normal numbers. The professional consensus is admirably plain: the goal is to decrease the clinical signs of diabetes while avoiding hypoglycaemia, the two conditions that together define a controlled diabetic (Behrend et al., 2018). That's the whole bar. A pet who is bright, eating well, holding their weight, drinking and weeing roughly normally, and who never has a hypo, is well-controlled, whatever a single reading says on a given afternoon.
This matters because chasing a flawless glucose is exactly how owners come to grief. Pushing the dose to flatten every high risks tipping the pet into a low, and hypoglycaemia is the genuine day-to-day danger, not the slowly-accruing complication. So everything below sits on that foundation: control buys protection from complications, but it's clinically-defined control, signs resolved and no hypos, never tight numbers won at the cost of a hypo. What that control looks and feels like day to day, and the targets behind it, is the subject of what good control actually looks like: that page is what control is, this one is what control prevents.
The two species sort themselves neatly. The signature complication of the diabetic dog is the cataract. The signature complication of the diabetic cat is the neuropathy. Same word, two genuinely different diseases. I'll take them in turn, then come to the two that threaten both.
Dogs: cataracts, and the real limit of control
If you have a diabetic dog you need to know about cataracts, and you need me to be straight, because this is the one place on the page where good control helps least. They are effectively the rule rather than the exception: around 80% of diabetic dogs develop them within roughly the first year to sixteen months of diagnosis (Beam et al., 1999). They can cloud the lens and take a dog's sight quickly, sometimes over a matter of weeks, and surgery can restore vision in suitable dogs. But the part I won't dress up is that tight blood-glucose control delays cataracts and does not reliably prevent them. Unlike almost everything else on this page, this is a complication your daily effort buys you less protection from.
I tell you that precisely so you aren't blindsided. An owner who watches their carefully managed dog go cloudy-eyed anyway can feel betrayed and start doubting the whole plan. Please don't. The cataracts aren't a sign you've failed; they're the one complication that marches to its own drum. Spotting them, the eye inflammation that can follow, and whether your dog is a surgical candidate all live in diabetic cataracts in dogs.
Cats: the dropped hocks, and why this is the complication control rewards most
This is the standout, it has no other guide to call home, and it's the complication where your effort pays the clearest dividend.
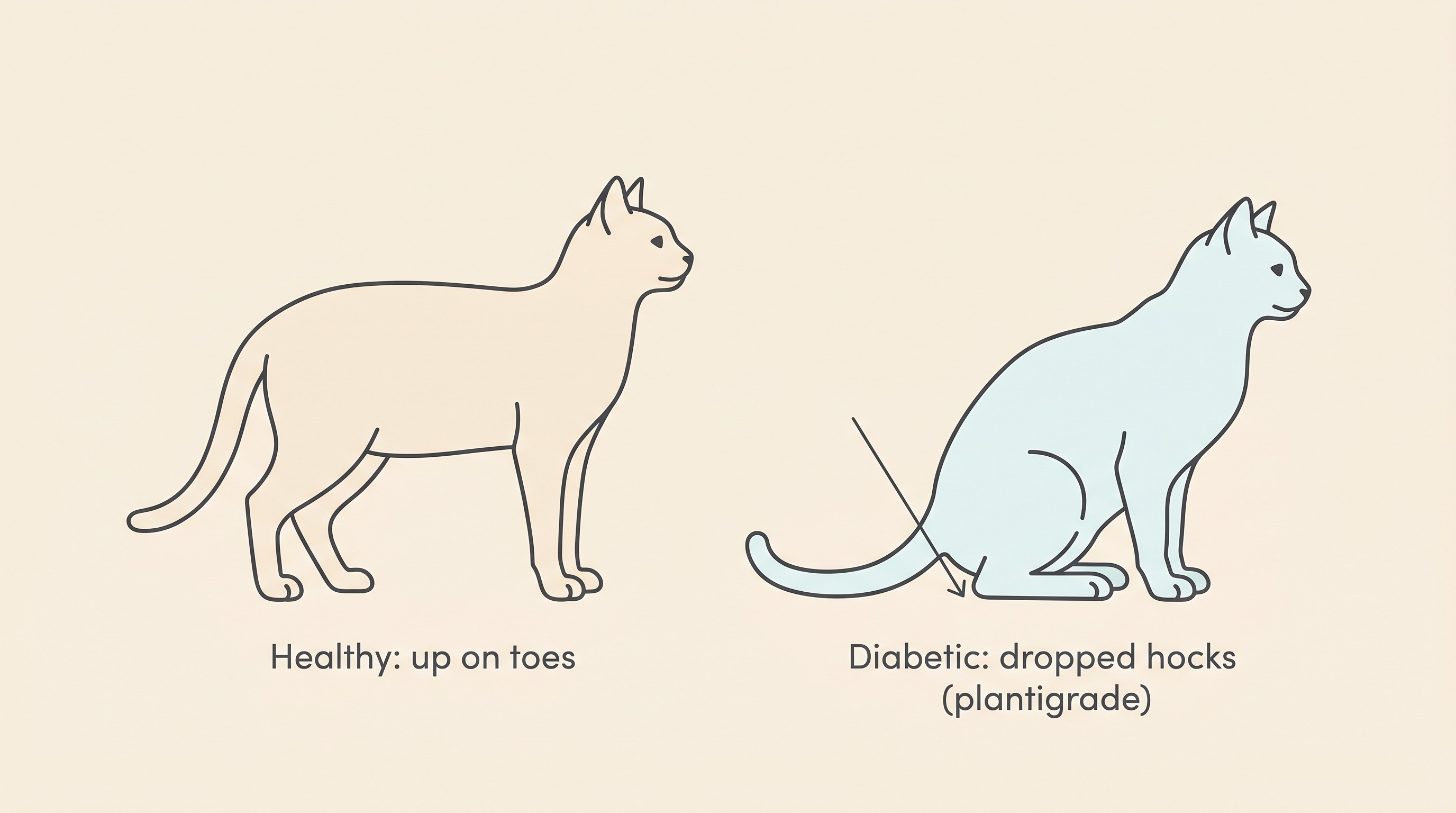
Cats get something dogs essentially don't: diabetic neuropathy. Prolonged high blood sugar slowly damages the peripheral nerves, worst in the back legs, and the result is a posture you can see across the room. A healthy cat walks up on its toes. A cat with diabetic neuropathy sinks back onto its hocks and walks flat-footed on the back legs, in what's called a plantigrade, or dropped-hocks, stance (Taylor et al., 2025). Alongside it you might notice hind-limb weakness, an unwillingness or inability to jump up where the cat used to spring easily, a wobbly narrow-based back end, muscle wasting over the hind legs, and sometimes irritability when you handle the feet. In advanced cases the front legs can drop onto the wrists too. The problem underneath is a sensorimotor polyneuropathy: the nerve fibres are injured, their insulating myelin splits and breaks down, and in severe cases the fibres degenerate (Mizisin et al., 2002).
How common is it? Overt, visible neurological signs turn up in roughly 10% of diabetic cats (Hughston, 2014). But that figure understates how widespread the nerve damage really is, because if you examine the nerves of diabetic cats closely under the microscope, the vast majority, around 90%, show some abnormality even when the cat looks perfectly steady on its feet (Hughston, 2014; Mizisin et al., 2002). Low-grade nerve change is almost universal in diabetic cats, and a minority cross the line into something you can see. And this really is a feline problem: diabetic neuropathy is seen in cats and only rarely in dogs (Thomas / MSD Vet Manual). If the biology interests you, chronic high glucose drives the polyol pathway, flooding the nerves with fructose, and even thickens the tiny blood vessels that feed them, by around 73% compared with healthy cats in one study (Estrella et al., 2008). But you don't need the histology. You need the one idea that follows from it.
The dropped hocks frequently get better when you get the glucose under control. Good glycaemic control isn't just damage limitation here; it is the treatment, and the nerves can heal. The classic series followed seven diabetic cats with neuropathy, and five of the seven had their clinical signs abate once insulin therapy brought the blood glucose under control, or once the diabetes itself resolved (Kramek et al., 1984). The authoritative texts agree: the prognosis is guarded, but partial or complete recovery can occur with insulin therapy (Thomas / MSD Vet Manual). So a cat sunk onto its hocks at diagnosis is not sentenced to walk that way. Bring the sugar down and steady it, and there's a genuine chance you'll watch your cat stand back up on its toes over the following weeks to months.
I have to keep that hope realistic. Recovery is gradual, weeks to months rather than days, and it isn't guaranteed or always complete. And a cat that already has neuropathy has by definition been running high for a while, which is itself a reason to act fast: cats already showing it are less likely to enter diabetic remission, presumably because the dropped hocks mark more prolonged hyperglycaemia (Taylor et al., 2025). That remission angle, the chance some cats come off insulin altogether, is its own large subject, told properly in feline diabetic remission. One last thing, because owners ask: you may read about vitamin B12 (methylcobalamin) for the nerves. There's no good evidence it treats feline diabetic neuropathy, and while some vets add it because it's low-risk, it is not a substitute for glucose control, which remains the only proven lever.
Both species: the infection loop, and why a wobble means hunt for one
Whichever animal you have, there's a quieter complication worth understanding, because spotting it protects your control. Poorly controlled diabetes and infection feed each other in a vicious circle: high tissue glucose and a blunted immune response leave a diabetic pet prone to infection, and infection in turn drives insulin resistance and worsens control. The everyday culprits are the ones the consensus lists among the commonest concurrent disorders of the diabetic patient: urinary tract infections, skin infections (dermatitis) and ear infections (otitis), alongside Cushing's disease, pancreatitis, neoplasia and an underactive thyroid (Behrend et al., 2018).
The urinary point carries a nuance owners almost never hear. In diabetic dogs these infections are often completely silent: in one study, 14% of diabetic dogs had a positive urine culture, and of those, 73% showed no urinary signs at all (Nelson et al., 2023). Nothing you'd notice from the outside, yet a hidden infection quietly nudging the glucose up. So the take-home is twofold. Good control lowers the infection risk in the first place, and an unexplained slide in a previously-steady diabetic should prompt your vet to go hunting for a brewing infection rather than simply reaching for a bigger dose. The systematic side of all this, the dental disease, the obesity, the proper work-up, belongs to the everyday things that wreck control. The principle to hold here: a wobble in control is a clue, not only a dosing problem.
DKA in dogs and cats: the one that kills, and the one control prevents
The complication that genuinely takes diabetic pets' lives is diabetic ketoacidosis. When there isn't enough working insulin, the body breaks down fat for fuel, producing acids called ketones, and the blood turns dangerously acidic. It's the life-threatening end of uncontrolled diabetes, and steady control is largely how you stay out of it. DKA is usually set off by a concurrent illness or stressor rather than appearing out of nowhere: a concurrent disease is present in around 70% of dogs and roughly 90% of cats that develop it, most often pancreatitis, a urinary or other infection, or, in dogs, Cushing's disease (Veterinary Partner / VIN). That's exactly why the infection loop above matters, and why the sick-day rules matter: a vomiting, off-colour diabetic is one at risk of tipping over.
I'm not teaching the warning signs or ketone testing here; that's the job of diabetic ketoacidosis (DKA), and the what-to-do-when-they're-ill side belongs to travel and sick-day rules. The message for this page is the hopeful one: steady control, never skipping insulin without veterinary advice, and following your vet's sick-day plan are precisely how you keep a diabetic pet out of the complication most likely to kill them.
One safety line for cat owners specifically. If your cat is managed on one of the newer oral drugs, an SGLT2 inhibitor (Senvelgo or Bexacat) rather than insulin, you need to know one particular risk. These drugs can cause euglycaemic DKA, ketoacidosis with a near-normal glucose, which is dangerously easy to miss precisely because the sugar reading looks fine. It affects roughly 1 in 15 newly-diagnosed cats started on them and around 1 in 10 cats previously treated with insulin (Taylor et al., 2025). They are for cats only, only certain newly-diagnosed cats not already on insulin, and they're a real safety conversation rather than a casual oral alternative. The full detail sits with the drug line-up in insulin types and oral options.
So what does good-enough control really buy?
Let me be straight about both halves of the bargain. Good control cannot promise zero complications. Most diabetic dogs will still get cataracts, control or not, and some cats will still show neuropathy. Anyone who offers you a guarantee is selling you something.
But what good, clinically-defined control buys is real and substantial. A bright pet, eating well, stable in weight, drinking and weeing roughly normally and never having a hypo, has measurably fewer crises: less DKA, less severe infection (Behrend et al., 2018; Veterinary Partner / VIN). The dropped-hocks cat is given its best chance of walking normally again (Kramek et al., 1984; Taylor et al., 2025). And the slide is slowed. UK primary-care data put median survival from diagnosis at 15.6 months across all diabetic dogs, rising to 20.2 months for dogs that got through the first week and into proper treatment (Heeley et al., 2020). Read that the right way round: the early window is the hazardous one, and many of those early losses are the untreated or the hardest to treat. A dog that comes through the first weeks and is reasonably controlled often does well for a couple of years or considerably longer, and these are good years, not borrowed time. The fuller reassurance on outlook lives in is it a death sentence. The feline consensus says the very same of early treatment in cats, that it improves outcomes by avoiding significant weight loss and the development of complications (Taylor et al., 2025).
So that's what the needles are for. Not nothing, and not a platitude, but this specific list: fewer emergencies, a real shot at reversing the dropped hocks, slower decline, more comfortable time on the right side of the disease. If you'd like to watch that payoff accumulate rather than take it on faith, the Glucose Companion plots your readings into a trend over weeks and months, so the steady line becomes something you can see take shape. On the days it all feels like a chore, that trend is the thing worth looking at. It's the shape of the good years you're buying, one injection at a time.
References
- Beam, S., Correa, M. T., & Davidson, M. G. (1999). A retrospective-cohort study on the development of cataracts in dogs with diabetes mellitus: 200 cases. Veterinary Ophthalmology, 2(3), 169-172.
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA diabetes management guidelines for dogs and cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Estrella, J. S., Nelson, R. N., Sturges, B. K., Vernau, K. M., Williams, D. C., LeCouteur, R. A., Shelton, G. D., & Mizisin, A. P. (2008). Endoneurial microvascular pathology in feline diabetic neuropathy. Microvascular Research, 75(3), 403-410.
- Heeley, A. M., O'Neill, D. G., Davison, L. J., Church, D. B., Corless, E. K., & Brodbelt, D. C. (2020). Diabetes mellitus in dogs attending UK primary-care practices: frequency, risk factors and survival. Canine Medicine and Genetics, 7, 6.
- Hughston, L. (2014). Feline diabetes red flags. Clinician's Brief, November 2014.
- Kramek, B. A., Moise, N. S., Cooper, B., & Raffe, M. R. (1984). Neuropathy associated with diabetes mellitus in the cat. Journal of the American Veterinary Medical Association, 184(1), 42-45.
- Mizisin, A. P., Shelton, G. D., Burgers, M. L., Powell, H. C., & Cuddon, P. A. (2002). Neurological complications associated with spontaneously occurring feline diabetes mellitus. Journal of Neuropathology & Experimental Neurology, 61(10), 872-884.
- Nelson, V., Downey, A., Summers, S., & Shropshire, S. (2023). Prevalence of signs of lower urinary tract disease and positive urine culture in dogs with diabetes mellitus: a retrospective study. Journal of Veterinary Internal Medicine, 37(2), 550-555.
- Taylor, S., Cannon, M., Church, D., Fleeman, L., Fracassi, F., Gilor, C., Mott, J., Niessen, S., et al. (2025). 2025 iCatCare consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
- Thomas, W. B. Metabolic disorders of the peripheral nerves and neuromuscular junction in animals. MSD/Merck Veterinary Manual (Nervous System), current online edition.
- Brooks, W. Diabetic ketoacidosis in dogs and cats. Veterinary Partner (VIN), reviewed edition.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine