Diabetic Cataracts in Dogs: Spotting and Managing the Blindness Risk
Claire Greenway
BVM&S MRCVS
There's a phone call I take more than almost any other from owners of newly diagnosed diabetic dogs. The dog was fine. Then, over a weekend, the eyes went cloudy and the dog started bumping into the coffee table. The owner is frightened, and underneath the fright there's usually a flicker of guilt: did I do this? Did I get the injections wrong?
So let me start where it matters most. You almost certainly did not cause this, and it is not a sign you've been managing the diabetes badly. Cataracts are by some distance the commonest complication of diabetes in dogs, and the great majority of diabetic dogs develop them whatever their owner does. The truth cuts both ways, though: cloudy eyes are expected and not your failure, and a cloudy diabetic eye is not something to simply watch and hope about. It needs looking at, and in most dogs sight can be given back. Diabetes brings other risks too, and heading those off with good control belongs in preventing diabetes complications; here I'm staying with the eyes.
What's actually happening inside the lens
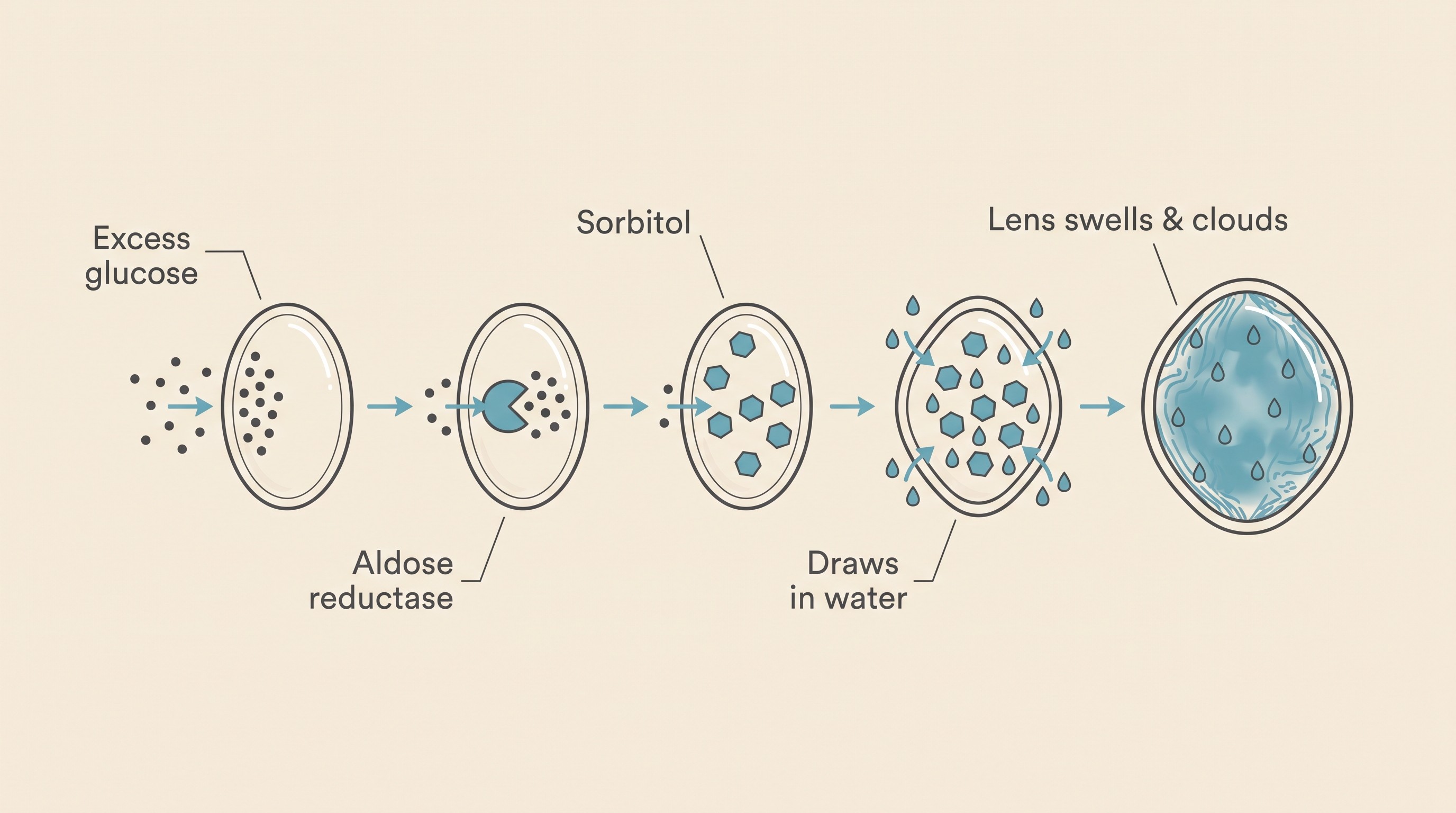
It helps to know what's going on inside the lens, because it isn't ageing and it isn't wear. The lens takes up glucose from the fluid it sits in, and in a healthy dog that's no problem. But when blood glucose runs high, the lens is flooded with more sugar than its normal machinery can handle, and an enzyme called aldose reductase starts converting the excess into a sugar-alcohol called sorbitol (Lee & Chung, 1999). Sorbitol is the troublemaker: it can't easily get back out of the lens fibres, so it builds up, and because it's osmotically active it drags water in after it. The fibres swell and eventually rupture, and with the oxidative stress that comes as the same pathway depletes the lens's antioxidant defences, the orderly transparent structure breaks down into opacity (Lee & Chung, 1999; Richter et al., 2002). That's a cataract.
The word to take from that is osmotic. This is glucose-driven, not age-driven, which is why it comes on so quickly and why a young diabetic dog gets cataracts just as readily as an old one. The trigger is the sugar, not the years.
How common, and how fast
I'd rather give you the real numbers than soften them, because the scale of it is part of the reassurance. In the cohort study everyone still cites, around half of diabetic dogs had developed cataracts by roughly five to six months after diagnosis, about three-quarters by twelve months, and around 80% within about sixteen months (Beam et al., 1999). A separate ten-year referral series found cataract in 97.3% of the diabetic eyes presented, comfortably the most common eye change in these dogs (Cantero et al., 2023). So around 80% within the first year or so is the working figure (Beam et al., 1999).
And they can arrive fast. Diabetic cataracts often progress over days to a few weeks rather than the slow years an ageing non-diabetic dog might take, and they're frequently bilateral, which is why so many owners describe a dog that seemed fine and then, almost overnight, couldn't see. In one series of rapidly swelling cataracts, they had been present for a mean of only about 39 days (Wilkie et al., 2006); Cornell's veterinary centre puts it simply, that in diabetic dogs these cataracts tend to form quickly (Cornell Riney Canine Health Center). I tell owners this at diagnosis now, precisely so a cloudy eye three months later feels like something we predicted together rather than a fresh disaster.
Signs to look for at home
Most owners spot it without knowing the word for it: a bluish-grey or white cloudiness sitting in the pupil, the dark centre of the eye, where you'd normally see straight through to black. Behavioural clues often come alongside or first: bumping into furniture, hesitating at the top of the stairs, cautious in dim light or unsure in unfamiliar rooms, suddenly sticking close on walks. Because it's often both eyes at once, there may be no "good side" to compensate with, which is why the change in confidence can seem so abrupt.
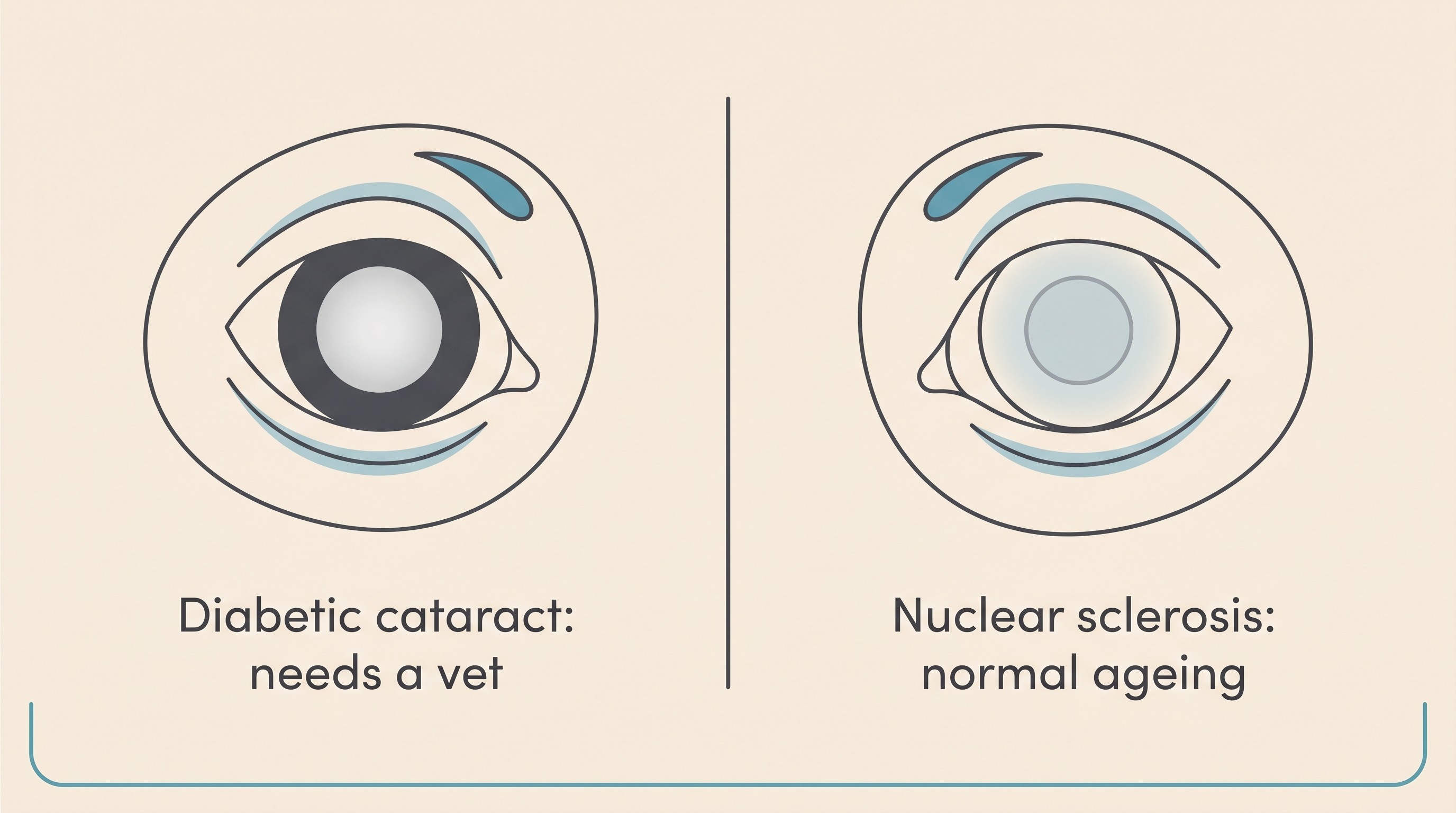
One distinction is worth holding, because owners conflate the two and it worries everyone for nothing. As dogs age, the lens often develops a hazy blue-grey sheen called nuclear sclerosis: it looks a little like a cataract from across the room, but it is a normal part of getting older, the dog still sees through it, and it does not cause blindness. A vet tells the two apart in seconds with a light, which is the point: nuclear sclerosis needs nothing, a diabetic cataract needs attention, and you cannot reliably tell which from the sofa.
The other sign to take seriously is an eye that looks sore: red, squinting, weeping, held half-shut, or one the dog wants to rub. That's not the cataract itself. That's the complication I want to tell you about next, and it's the reason "just keep an eye on it" is the wrong plan.
The complication that makes this more than cloudiness: lens-induced uveitis
This is the part competitor pages tend to skip, and it's the strongest reason to get a diabetic cataract looked at rather than simply watched.
When a diabetic cataract swells quickly, the lens can become intumescent, swollen and waterlogged, and leaky lens proteins start to escape into the eye. The immune system doesn't recognise these proteins and reacts to them, setting up inflammation inside the eye called lens-induced uveitis, or LIU (Wilkie et al., 2006; Cornell Riney Canine Health Center). At its worst, a fast-swelling lens can rupture its own capsule, the thin bag that holds it, spilling lens material and triggering severe inflammation. In the rapid-cataract series, the majority of eyes had already had a spontaneous capsule rupture before any surgery, and intumescent cataracts were the commonest type, over half the cataractous eyes in the ten-year study (Wilkie et al., 2006; Cantero et al., 2023).
Why does that matter at home? Because uncontrolled LIU is what turns a manageable cataract into a sight-threatening, and sometimes painful, problem. Persistent inflammation can lead on to secondary glaucoma, a painful rise in eye pressure that is notoriously hard to control once it takes hold, and it raises the risk of retinal detachment (Cornell Riney Canine Health Center). This is why a diabetic dog with cataracts is usually started on anti-inflammatory eye drops and monitored, even when surgery isn't yet on the table. It's also why I push back, gently but firmly, when an owner tells me they've decided to "just leave it and see". A diabetic cataract is not cosmetic cloudiness. The eye needs examining, and often treating, not just watching.
Surgery can give the sight back
Now the genuinely hopeful part, and it's hopeful with evidence behind it. Cataract surgery in dogs, the same operation people have, is called phacoemulsification, or phaco: the cloudy lens is broken up with ultrasound and removed through a tiny incision, and in most dogs an artificial lens is placed. It works. In a study comparing diabetic dogs that had surgery against those managed with eye drops alone, 94.8% of operated eyes were visual at last follow-up, the large majority of them complication-free, against just 7.6% of the medication-only eyes; the medically managed group also carried close to four times the overall risk of complications (Lee et al., 2023). For good candidates, reported success generally sits around 80 to 90% (Cornell Riney Canine Health Center). So when I say surgery restores sight in most dogs, that's not optimism, it's the data.
The catch, and there's always a catch, is that not every diabetic dog is a candidate, and timing matters. Surgery is the territory of a veterinary ophthalmologist, and before they operate they need to know two things the opaque lens hides: is the retina still working, and is it still attached. They check the first with an electroretinogram (ERG), measuring the retina's response to light, and the second with an ocular ultrasound behind the cloudy lens (Lee et al., 2023; Wilkie et al., 2006). The dog also has to be a reasonable anaesthetic candidate: a stable, reasonably controlled diabetic without a recent crisis like diabetic ketoacidosis or a flare of pancreatitis. Poor glucose control, advanced inflammation, scarring or existing retinal disease all count against suitability (Lee et al., 2023).
The next consideration is speed. Because the secondary complications, the LIU, the capsule rupture, the glaucoma, are what spoil the odds, ophthalmologists generally want to assess and operate promptly, often within a couple of weeks of the cataract appearing, rather than wait (Wilkie et al., 2006; Lee et al., 2023; Cornell Riney Canine Health Center). So if your vet confirms a diabetic cataract, the useful next question isn't "should we watch it" but "can we get a referral to see whether surgery is an option". On cost, I'll be straight: this is specialist surgery, it isn't cheap, and it's usually a per-eye conversation, but I won't put a figure on it because it varies too much by centre to be useful. The wider lifetime cost picture is in the cost and insurance guide.
If surgery isn't the path
Surgery isn't right or possible for every dog or every household, and choosing not to operate is not abandoning your dog. Dogs live extraordinarily well without sight, navigating by smell, hearing and memory, and a blind dog in a familiar home, with furniture kept in its usual places, very often adapts to the point where visitors don't realise anything's wrong. What I'd ask, if you go this route, is that the eyes are still looked after rather than ignored: the LIU still needs controlling with drops and the pressures still want checking, because a blind eye can still become a painful one, and that's the bit we can prevent. A comfortable blind dog is a perfectly good outcome. A painful blind eye is not, and it's avoidable.
What good glucose control can and can't do for the eyes
This is the line I'd most want you to leave with, because it protects you from a particular kind of heartbreak.
Tighter, steadier glucose control is worth doing, and there's reason to think it slows things down. In a recent preliminary study, the dogs whose control improved over time, with falling fructosamine and less glucose variability, tended not to need cataract surgery, while higher variability went with faster progression; even so, four of nine newly diagnosed dogs needed surgery within twelve to twenty-four weeks (Arad et al., 2025). So less of the swinging, spiky glucose that drives the sorbitol pathway may buy the lens time. That's a real reason to keep things as steady as you reasonably can, and if you log readings and CGM traces in the Glucose Companion you can actually see the variability you're trying to flatten. What steady control looks and feels like day to day is covered in the well-controlled diabetic pet.
But here's the non-negotiable: good control delays cataracts, it does not reliably prevent them. They develop in the great majority of diabetic dogs regardless of how tightly the diabetes is managed (Cornell Riney Canine Health Center; Beam et al., 1999). I labour this for one reason: I never want an owner who's been doing everything right to see a cloudy eye and read it as their failure. It isn't. It's the disease doing what it overwhelmingly does, on a dog whose owner did nothing wrong. (Prevention is being researched: aldose-reductase-inhibitor eye drops delayed cataract formation in a small trial, but they aren't a licensed, available product, so they're context rather than something you can buy today (Kador et al., 2010).)
A quick word on cats, because owners always ask
If you've also got a cat, or you've read that diabetic cats don't tend to go blind, you've read correctly, and the reason is neat. The whole cascade depends on aldose reductase being active in the lens, and in older cats its activity is much lower than in a dog's; because feline diabetes usually starts later in life, the enzyme that drives the damage is largely missing, so cats are mostly protected despite the same high blood sugar (Richter et al., 2002). It's one of the clearest illustrations that canine and feline diabetes really are two different diseases, which is the subject of the dog versus cat difference. For your dog, the cataract risk is real and part of the long game, because canine diabetes is the lifelong, insulin-dependent kind that doesn't go into remission (Heeley et al., 2020).
So here's where I'd point you next. If your dog's eyes are clear today, you now know what to watch for and why a sudden cloudiness shouldn't send you into a spiral of self-blame. If you're already looking at a cloudy pupil, the most useful thing you can do this week is ask your vet to examine the eyes and, if it's a diabetic cataract, talk about referral sooner rather than later, while the odds are best. Cloudy eyes are not the end of a good life for your dog, and very often they're not the end of their sight either.
References
- Beam, S., Correa, M. T., & Davidson, M. G. (1999). A retrospective-cohort study on the development of cataracts in dogs with diabetes mellitus: 200 cases. Veterinary Ophthalmology, 2(3), 169-172.
- Arad, D., Ofri, R., Sebbag, L., Rimer, D., & Mazaki-Tovi, M. (2025). The effect of glycemic control on diabetic cataract progression rate in dogs: A preliminary study. The Veterinary Journal, 314, 106491.
- Cantero, F., Ortillés, Á., Peña, M. T., & Leiva, M. (2023). Prevalence of ocular findings and their association with glycemia in dogs with diabetes mellitus: A 10-year clinical study (2009-2019). Open Veterinary Journal, 13(5), 620-628.
- Cornell Riney Canine Health Center. Canine Cataracts. Cornell University College of Veterinary Medicine.
- Heeley, A. M., O'Neill, D. G., Davison, L. J., Church, D. B., Corless, E. K., & Brodbelt, D. C. (2020). Diabetes mellitus in dogs attending UK primary-care practices: frequency, risk factors and survival. Canine Medicine and Genetics, 7, 6.
- Kador, P. F., Webb, T. R., Bras, I. D., Ketring, K., & Wyman, M. (2010). Topical Kinostat ameliorates the clinical development and progression of cataracts in dogs with diabetes mellitus. Veterinary Ophthalmology, 13(6), 363-368.
- Lee, A. Y. W., & Chung, S. S. M. (1999). Contributions of polyol pathway to oxidative stress in diabetic cataract. FASEB Journal, 13(1), 23-30.
- Lee, E., Kang, S., Jeong, D., & Seo, K. (2023). Comparison of the outcomes of phacoemulsification versus topical medication alone in canine diabetic cataracts: a retrospective study. Journal of Veterinary Science, 24(6), e86.
- Richter, M., Guscetti, F., & Spiess, B. (2002). Aldose reductase activity and glucose-related opacities in incubated lenses from dogs and cats. American Journal of Veterinary Research, 63(11), 1591-1597.
- Wilkie, D. A., Gemensky-Metzler, A. J., Colitz, C. M. H., et al. (2006). Canine cataracts, diabetes mellitus and spontaneous lens capsule rupture: a retrospective study of 18 dogs. Veterinary Ophthalmology, 9(5), 328-334.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine