TPLO vs TTA vs Lateral Suture: An Even-Handed Comparison
Dr. Alastair Greenway
MRCVS
Start reading about cruciate surgery and you'll hit a wall of acronyms within five minutes. TPLO. TTA. Lateral suture, extracapsular, TightRope. One forum swears blind that TPLO is the only thing worth doing; the next says their dog did beautifully on a lateral suture and the bone-cutting operations are overkill. Your own vet has recommended one of them, and you're left wondering whether you're being steered toward the right thing or just the thing this practice happens to do.
I want to do something a lot of pages won't, which is refuse to crown a winner. There isn't a single best cruciate operation. There's a best operation for this particular dog, with this particular knee, owned by this particular family, and working that out should be a real conversation with your surgeon, not a verdict you reach from a website. What I can do is lay the three main options side by side, with their real trade-offs, so you understand what's being weighed.
This article assumes the surgery-or-not question is already settled. If you're still weighing whether to operate at all, that's a different decision, covered in Surgery or Not? How to Think About the Cruciate Decision. Here, we're choosing between operations.
Two families of operation
It helps enormously to know that these operations split into two completely different camps that solve the problem from opposite directions.
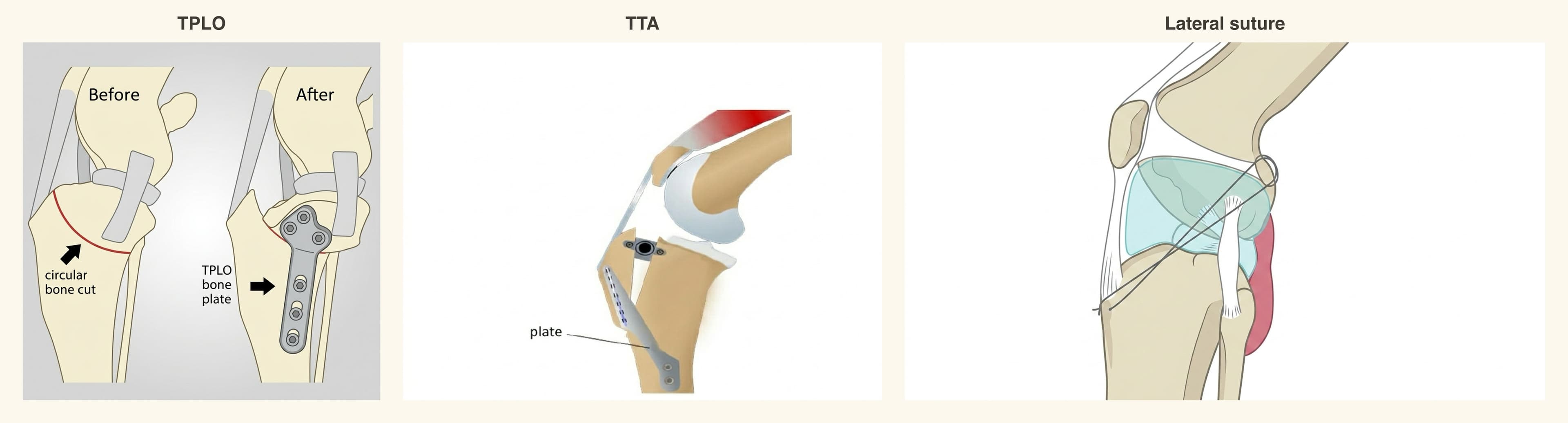
The first is the bone-cutting operations, the osteotomies: the TPLO and the TTA. Rather than replace the failed ligament, they change the geometry of the knee so it no longer needs the cruciate to stay stable under weight. It's structural engineering: instead of fixing the broken part, you reshape the building so the broken part doesn't matter.
The second is the lateral suture, also called the extracapsular or fabellotibial suture, working from outside the joint. A strong implant is anchored across the knee, roughly where the ligament used to pull, holding things steady while the body does the real long-term work: laying down scar tissue that gradually takes over as the suture weakens (RCVS Knowledge Canine Cruciate Registry). The implant is the scaffolding; the dog's own healing is the permanent structure.
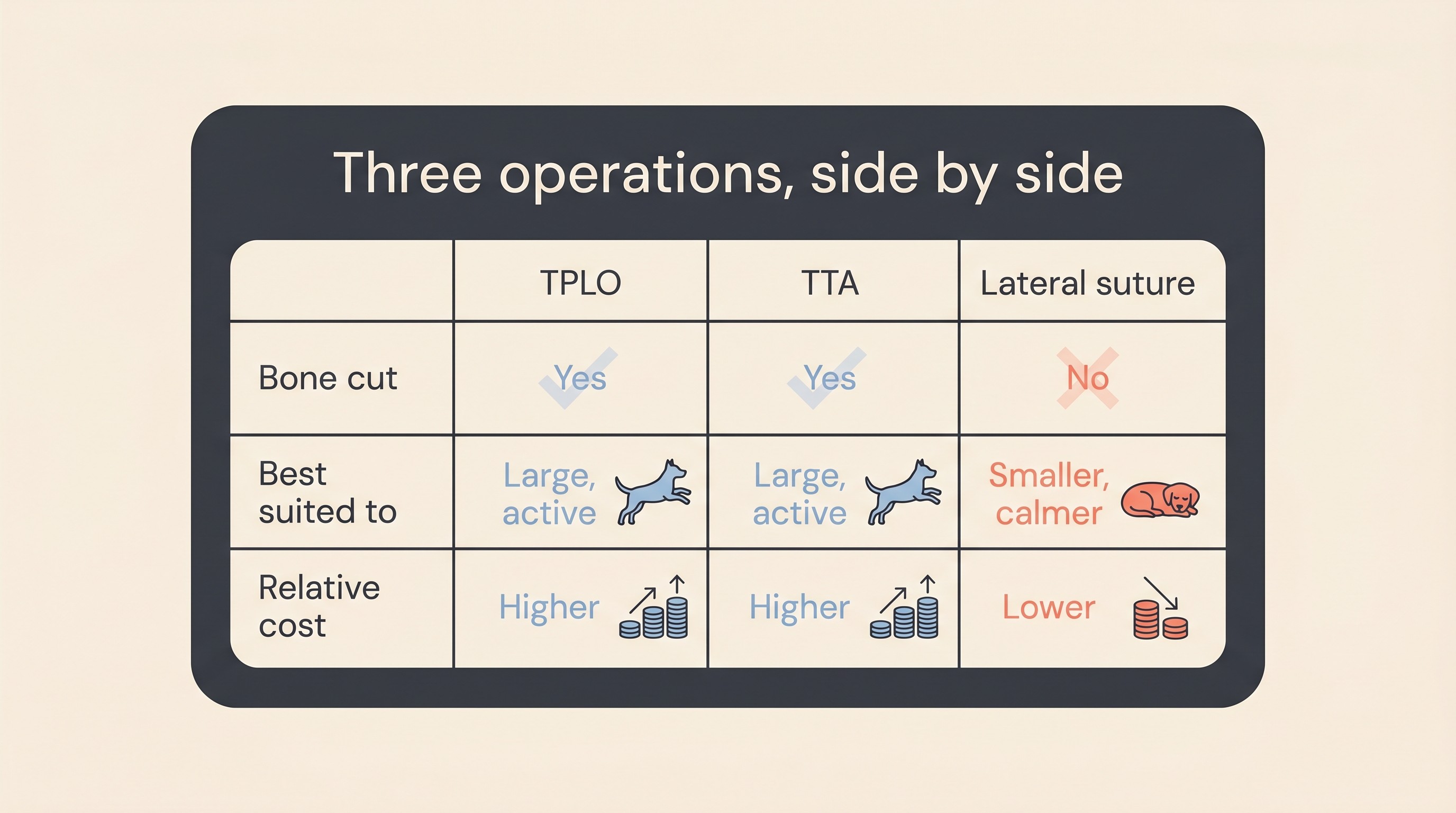
That single distinction explains almost every trade-off that follows. The osteotomies are more involved, dearer and carry the risks of cutting and healing bone, but they restructure the joint definitively. The lateral suture is gentler and cheaper but leans on the body, which is why your dog's size and activity matter.
TPLO
The TPLO, or tibial plateau levelling osteotomy, is the operation most people have heard of, and the one most often recommended for larger, more active dogs. The top of the shin bone slopes backward a little, and with the cruciate gone every step drives the shin down that slope: that's the abnormal movement causing the pain. The TPLO cuts and rotates the top of the shin to flatten that slope, holding it with a plate while it heals, so the knee stays stable without a working ligament.
Its real strength is the evidence behind it. The best systematic review of cruciate surgery concluded that the available evidence "most strongly supports" the TPLO for returning dogs to normal function (Bergh et al., 2014), and force-plate gait studies, which measure how a dog actually loads the leg rather than relying on an owner's impression, found it restoring limb function similar to normal dogs at both walk and trot by six to twelve months (Krotscheck et al., 2016). That's why, for a big athletic dog, it's so often the first suggestion.
No operation is free of risk, and I'd rather you heard the real numbers from me than from a scaremongering thread. Systematic-review data put the overall TPLO complication rate at around 16 per cent, with major complications near 5 per cent and catastrophic ones under 1 per cent (Beer et al., 2018), and a large series of 1,000 consecutive TPLOs found much the same: 14.8 per cent overall, 6.6 per cent of them major (Fitzpatrick and Solano, 2010). The great majority are managed successfully and most dogs do very well, but the figures aren't zero. How a TPLO is done, who it suits and what can go wrong lives in TPLO Explained: What It Is and Who It's For.
TTA and its relatives
The TTA, or tibial tuberosity advancement, is the other geometry-changing operation, reaching the same goal by a different route. Rather than levelling the slope, it advances the bony point at the front of the shin where the big thigh muscle attaches, so the muscle's pull counteracts the forward slide. There are relatives here too, including the CBLO and the CCWO, which a surgeon might prefer for particular knee shapes; the detail on all of them sits in TTA and the Other Osteotomies.
This is where I have to be even-handed, because the data pull in slightly different directions. The TTA tends to carry somewhat higher complication rates than the TPLO: that same systematic review put TTA total complications around 21 per cent and major complications around 13 per cent, against the TPLO's lower figures (Beer et al., 2018). And in a long-term comparison, dogs treated with TTA scored lower on owner and clinician assessment than those treated with either TPLO or TightRope, with significantly higher rates of major complications and subsequent meniscal tears (Christopher et al., 2013). I mention the meniscal point only as a comparison; the meniscus itself, and why a late tear matters, is explained in The Meniscus: The Other Injury in the Knee.
None of that makes the TTA a bad operation, and please don't read it that way. A surgeon who does a great many TTAs and gets excellent results may well be the right person for your dog's knee. But it does explain why, on the published evidence, the TPLO tends to edge ahead.
Lateral suture
The lateral suture is the gentler option, and for the right dog a genuinely good one, not a budget compromise. There's no bone cut at all: the implant mimics the line of the old ligament and holds the knee steady while the body builds its own scar-tissue stability. That sidesteps the whole category of bone-healing complications the osteotomies carry, it's usually noticeably cheaper, and it's far more widely offered, including by many first-opinion practices rather than only specialist centres. The full account is in Lateral Suture: The Less Invasive Option.
Its limitation is just as straightforward. The suture and scar tissue have to cope with whatever load the dog puts through the leg, and in a large, heavy, bouncy dog that load is considerable, so the implant is more likely to stretch or fail and the intermediate return of function is poorer than after a TPLO (Bergh et al., 2014). The registry notes that younger and larger dogs are more prone to complications with it, which is why it's more commonly advised in smaller or less active dogs (RCVS Knowledge Canine Cruciate Registry). For a 7kg terrier it's often exactly the right tool; for a 40kg Labrador who lives to chase a ball, your surgeon will usually steer you toward an osteotomy.
How surgeons actually choose
If there's no league-table winner, how does a good surgeon land on one operation for your dog? It comes down to a handful of factors. Your dog's size and activity level is usually the single biggest lever: heavy and athletic points toward an osteotomy, small and sedate opens up the lateral suture. Then comes the anatomy of the knee, including how steep that plateau slope is on the films, because the geometry of the individual joint can make one operation a cleaner fit; whether the meniscus is damaged, which the surgeon assesses and deals with at the same time; and cost, a legitimate part of the decision and nothing to feel awkward about (the lateral suture is usually cheapest, with the real UK estimates set out in What Cruciate Surgery Costs in the UK, and Insurance).
The factor owners tend to overlook is the last one: the surgeon's own training and case volume with each technique. This matters more than the theory. A high-volume surgeon doing the operation they do best, and do often, will reliably beat a textbook-superior operation done by someone who does it rarely. The osteotomies in particular usually mean a referral to an orthopaedic specialist, which is completely normal and no reflection on your own vet; when it's worth it is covered in Does My Dog Need an Orthopaedic Specialist?.
One thing to hold onto before we close. "The TPLO has the strongest evidence" is fair, but the same review didn't have enough good-quality data to fully rank every procedure against every other (Bergh et al., 2014), and over the long term all the main techniques do well: owner and clinician rated function beyond a year sat around 89 to 93 per cent of normal across all three (Christopher et al., 2013). So "the TPLO is the right operation for your dog" is a different statement, and only the surgeon with hands on the knee can make it. The outcomes themselves are encouraging: in a trial of overweight dogs, three-quarters of the surgical group met a stringent threshold by one year, combining an affected-limb force above 85 per cent of a healthy leg with a clear improvement in owner-reported scores (Wucherer et al., 2013). Recovery runs to around twelve weeks whichever operation you have, so the road home looks broadly similar in all three; what it involves is mapped out in The 12-Week Recovery Roadmap.
Two caveats, each with its own article. First, no operation prevents arthritis: once a knee has been unstable, some stifle osteoarthritis is essentially inevitable, and stabilising the joint slows its progression rather than stopping it, the long view taken in Cruciate Disease and Arthritis: The Lifelong Picture. Second, rupture of the cruciate in the other knee is common: one prospective study found 54 per cent of dogs went on to do so, at a median of around two and a half years (Muir et al., 2011). That's a planning fact, not part of choosing the operation, and it's covered in Will the Other Leg Go Too? The Bilateral Risk.
So here's the useful next step. Find out which operation your surgeon is leaning toward, read the deep-dive on that one, then ask them plainly why it's right for your dog specifically: its size and activity, the knee they actually saw on the films, and their own experience with that technique. A good surgeon will welcome the question. The Decision Helper lays those out if you'd like a hand beforehand, and once the operation is behind you the Recovery Tracker lets you log weight-bearing, lameness and swelling against the post-op week, so you can watch the progress that, across all three operations, the great majority of dogs do make.
References
- Beer P, Bockstahler B, Schnabl-Feichter E. Tibial plateau leveling osteotomy and tibial tuberosity advancement - a systematic review. Tierarztliche Praxis Ausgabe K: Kleintiere/Heimtiere. 2018;46(4):223-235. DOI 10.15654/TPK-170486.
- Bergh MS, Sullivan C, Ferrell CL, Troy J, Budsberg SC. Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. Journal of the American Animal Hospital Association. 2014;50(5):315-321. DOI 10.5326/JAAHA-MS-6356.
- Christopher SA, Beetem J, Cook JL. Comparison of long-term outcomes associated with three surgical techniques for treatment of cranial cruciate ligament disease in dogs. Veterinary Surgery. 2013;42(3):329-334. DOI 10.1111/j.1532-950X.2013.12001.x.
- Fitzpatrick N, Solano MA. Predictive variables for complications after TPLO with stifle inspection by arthrotomy in 1000 consecutive dogs. Veterinary Surgery. 2010;39(4):460-474. DOI 10.1111/j.1532-950X.2010.00663.x.
- Krotscheck U, Nelson SA, Todhunter RJ, Stone M, Zhang Z. Long term functional outcome of tibial tuberosity advancement vs. tibial plateau leveling osteotomy and extracapsular repair in a heterogeneous population of dogs. Veterinary Surgery. 2016;45(2):261-268. DOI 10.1111/vsu.12445.
- Muir P, Schwartz Z, Malek S, et al. Contralateral cruciate survival in dogs with unilateral non-contact cranial cruciate ligament rupture. PLoS One. 2011;6(10):e25331. DOI 10.1371/journal.pone.0025331.
- RCVS Knowledge Canine Cruciate Registry. Extracapsular Lateral Suture Stabilisation (ELSS): dog-owner information.
- Wucherer KL, Conzemius MG, Evans R, Wilke VL. Short-term and long-term outcomes for overweight dogs with cranial cruciate ligament rupture treated surgically or nonsurgically. Journal of the American Veterinary Medical Association. 2013;242(10):1364-1372. DOI 10.2460/javma.242.10.1364.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine