
The Meniscus: The Other Injury in the Knee
Dr. Alastair Greenway
MRCVS
Somewhere in the conversation about your dog's cruciate, a second word usually gets mentioned. The vet might say "we'll check the meniscus while we're in there," or "there's a meniscal tear too," or the surgeon reaches for "meniscal release" just as you'd finally got your head around the cruciate itself. There's a second reason owners come looking for this page too: a dog that had a textbook operation, recovered beautifully, then weeks or months later started limping again, with the meniscus named as the likely culprit.
Both routes lead to the same place, the part of the knee that most pages skate over in a sentence. I think that's a mistake, because the meniscus is often the bit that hurts the most, and a late meniscal tear is one of the more important things an owner can learn to recognise. So I'd rather give it the proper explanation it deserves. The underlying disease, the surgery decision and the choice of procedure all have their own guides; here, I'm staying on the meniscus.
The cushion that takes the load
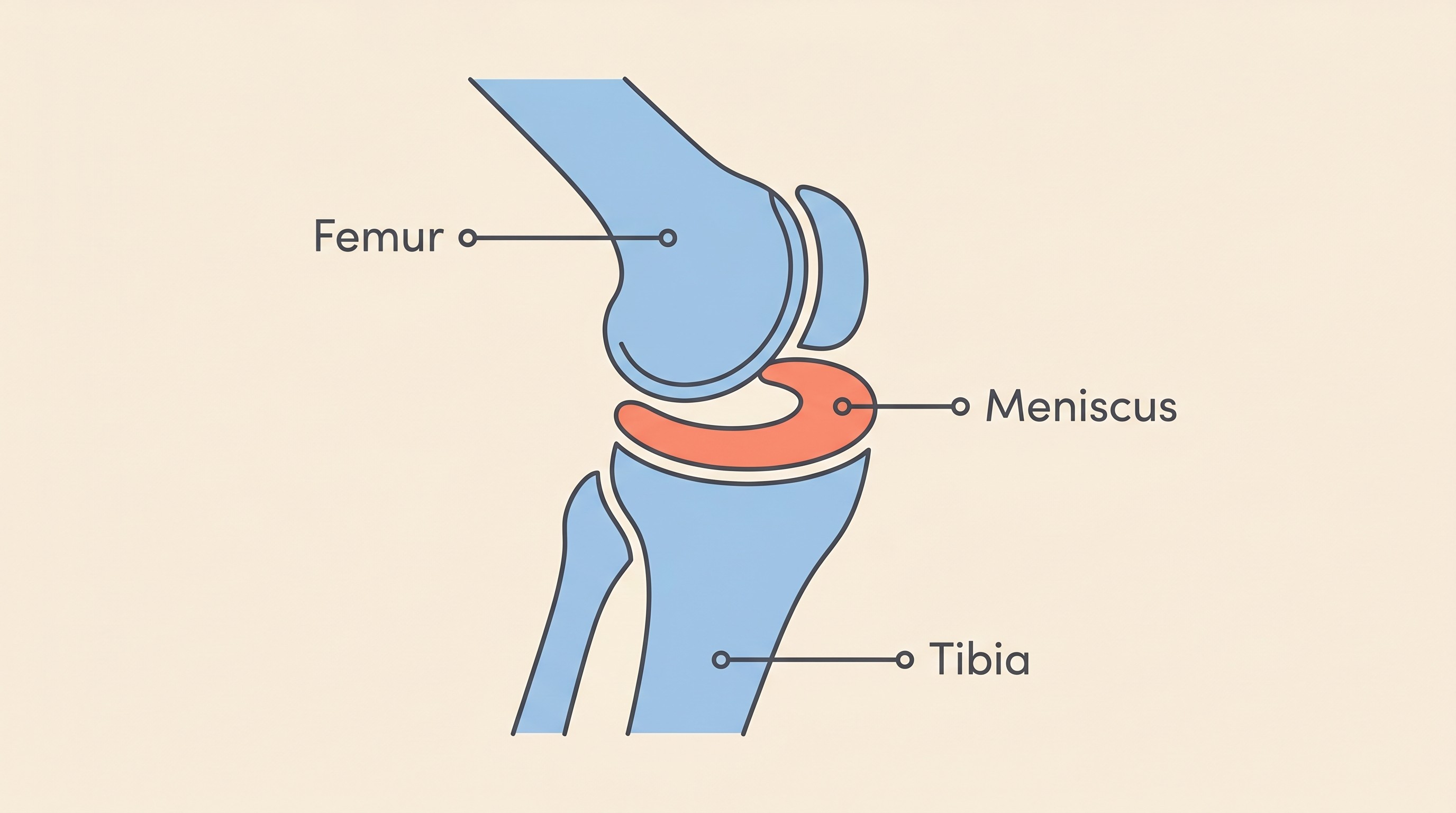
Picture the knee, the stifle, as a joint where a rounded thigh bone sits on a fairly flat shin bone. On its own that's not a stable arrangement, a bit like balancing a ball on a table. The meniscus is what makes it work. There are two of them in each knee, the medial on the inside and the lateral on the outside, each a tough C-shaped wedge of fibrocartilage between the two bones. It deepens the flat shin surface so the thigh bone has somewhere to nestle, spreads load across the joint, absorbs shock, and helps lubricate and stabilise the whole thing. This is no passive spacer. In the dog's knee the menisci carry roughly 65% of the load crossing the joint (Thieman et al., 2010). They are doing real work every step your dog takes.
So why does the meniscus get caught up in cruciate disease? When the cruciate ligament degenerates and fails, and it usually is degeneration rather than a clean one-off injury, which the degeneration guide explains in full, the knee becomes unstable. Every time your dog bears weight, the thigh bone slides backwards across the shin bone in a way it was never meant to. The medial meniscus is the one that pays for it, because it's firmly anchored to the shin bone, the joint capsule and the medial collateral ligament, so it cannot get out of the way. When the thigh bone shears backwards over it, the fixed back portion of the medial meniscus gets crushed and torn (Franklin et al., 2010). The lateral meniscus, by contrast, is only loosely attached, moves with the thigh bone, and so it almost always escapes: it's injured in only around 0 to 2% of cases (Franklin et al., 2010). When people say "meniscal tear" in a cruciate dog, they nearly always mean the medial one.
The meniscus isn't a separate freak accident. It's collateral damage from the instability, the second casualty of the same problem.
How common is it? Here I have to be careful, because the published figures range enormously and it would be easy to pick a scary number and run with it. The rate depends heavily on how thoroughly the surgeon looks. Inspected with an arthroscope, a tiny camera, concurrent tears turn up in around 80 to 85% of cruciate-rupture knees (Ritzo et al., 2014; Clinician's Brief). Inspected by eye through an opened joint, the figure is lower, often around a third: two large series found meniscal injury in 33.2% and 32.2% of stifles (Fitzpatrick & Solano, 2010; Kalff et al., 2011). One study ran both methods in the same population and got 83% by arthroscopy versus 44% by the open approach, so the camera was nearly twice as likely to spot a tear (Ritzo et al., 2014). The fair owner-facing summary, and the one the UK's Canine Cruciate Registry gives, is that somewhere between roughly 20% and 77% of cruciate dogs have a meniscal tear, with the spread mostly about detection rather than different dogs (RCVS Knowledge). The principle matters far more than the exact percentage: meniscal damage is common and worth taking seriously.
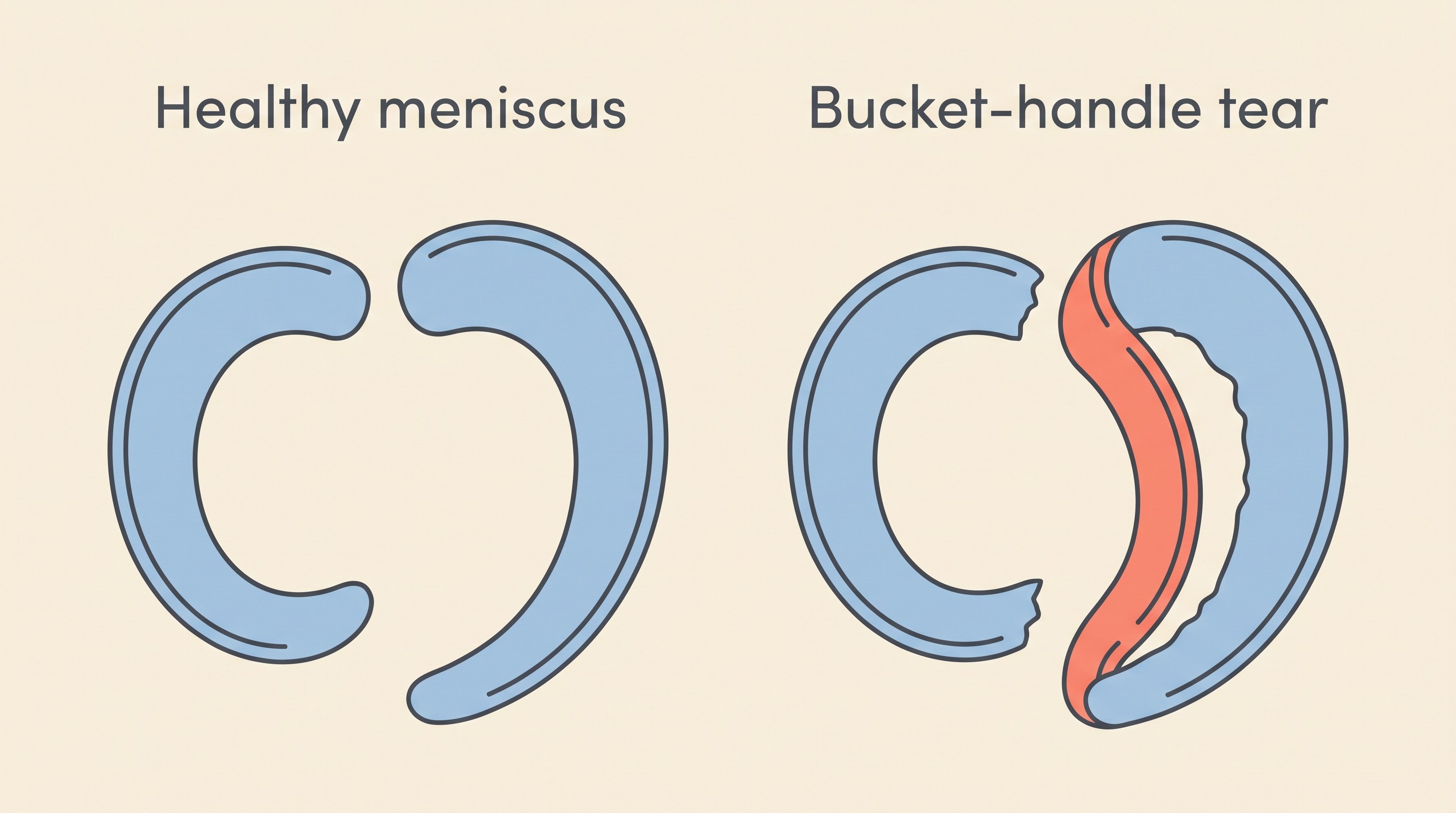
And why does it hurt so much? Because a torn flap, particularly the bucket-handle tear that's the commonest pattern, where a strip peels away from the back of the medial meniscus like the handle lifting off a bucket, gets caught and pinched between the bones every time the joint moves (Clinician's Brief). That's mechanically painful in a way the unstable ligament alone often isn't, and it can sometimes be felt or even heard as a click on examination or as your dog walks, the so-called "meniscal click" (RCVS Knowledge). For a lot of dogs, the torn meniscus is the part of the injury that hurts most acutely.
How it's dealt with at surgery
Whatever procedure your dog is having to stabilise the knee, and the comparison guide covers those choices even-handedly, the surgeon will inspect the meniscus as part of the operation. That might be by eye through the opened joint or with an arthroscope, sometimes with a small probe or a device that gently opens the joint to see the awkward back portion of the medial meniscus, which is genuinely hard to view (Ritzo et al., 2014).
If a torn portion is found, the surgeon removes just that damaged part, a partial meniscectomy, and leaves the healthy rim alone. That's deliberate and it matters: cadaver work shows that taking out only the torn piece preserves the joint's load-spreading far better than removing the whole meniscus, which sharply raises the pressure on the cartilage (Thieman et al., 2010). The aim is always to take the least that solves the problem, and if the meniscus is genuinely intact, the modern instinct of many surgeons is to leave it well alone.
That last point brings us to a real controversy, and I'd rather be candid about it than pretend the profession is united, because it isn't. For years a common practice was "meniscal release," deliberately cutting the back attachment of an intact meniscus so it can slide freely and is less likely to get crushed by any residual instability later. The logic was prevention, and there's a grain of truth to it: stifles where the meniscus was left untreated were around 3.8 times more likely to develop a later tear than those that had a release (Thieman et al., 2006).
The other side of the argument is why the practice has fallen out of favour with many surgeons. Cutting an intact meniscus is not harmless. In a study on knees that still had a working cruciate, a meniscal release on its own caused lameness at 8 and 12 weeks, significantly worse cartilage damage in the inner compartment, and more arthritis on X-ray by 12 weeks, all compared with a sham procedure (Luther et al., 2009). You're trading a reduced chance of a future tear for a guaranteed bit of present harm. So the trend now is towards careful inspection and treating only what is actually torn, rather than pre-emptively cutting healthy tissue. That's the surgeon's individualised judgement, weighing the specific knee, the procedure and their own experience, and it isn't for me to hand down a verdict from here. What you can do is ask whether they tend to release an intact meniscus or leave it, and why. A thoughtful answer tells you a great deal.
The late meniscal tear
A meniscus that was intact at surgery, or that looked intact, can tear weeks to months later, even after a flawless recovery. It's called a late meniscal tear, and there are two ways it happens: either a tiny tear was present but missed at the time, or a previously sound meniscus is damaged afterwards by a little residual instability in the joint (Kalff et al., 2011). Either way, the result is distinctive.
The reassuring news first: it isn't common, especially after a TPLO. In a series of 1,000 dogs, late meniscal tears occurred in 2.8% (Fitzpatrick & Solano, 2010). Another TPLO series put it at 5.6% (Kalff et al., 2011). Across all procedures the registry quotes a wider range, roughly 2% to 22% (RCVS Knowledge), and slightly lower late-tear rates are one reason some surgeons favour the bone-cutting procedures, though that comparison belongs to the procedure guides, not here.
What matters far more than the percentage is knowing what it looks like, because you are the person most likely to spot it. The classic story is a dog that was doing genuinely well, weeks to months after the operation, who suddenly comes up lame again, and sometimes there's an audible click (RCVS Knowledge). As with cruciate lameness generally, it can wax and wane and tends to look worse after activity, which is exactly why an intermittent limp is so easy to talk yourself out of. If you're tracking recovery the sensible way, by how much weight your dog puts through the leg, how lame they are and whether there's new swelling, measured against the post-operative week you're in, a late tear shows up as a clear regression: a leg that was getting steadily better suddenly going backwards. That's exactly the pattern the Recovery Tracker is built to make visible.
The genuinely good news is that a late tear is fixable. The joint is re-inspected, the torn part removed, and dogs generally go back to good function afterwards, with a small added cost in long-term arthritis from the extra cartilage handling (RCVS Knowledge). That small arthritis nudge, and the lifelong joint care that follows any cruciate knee, is picked up properly in the long-term arthritis guide.
I'm deliberately not writing a full red-flags checklist here, because the recovery red-flags guide does that thoroughly and tells you exactly when to pick up the phone. But one headline is worth carrying on its own: a dog that was recovering well and then abruptly goes lame again is not a setback to wait out. It's a reason to ring your vet. That single sign is rarely spelled out in the surgery paperwork, and knowing it is one of the most useful things you can do to protect your dog's recovery.
So before the operation, ask your surgeon two questions: how the meniscus will be assessed, and what a late tear would look like in the months afterwards. The first tells you the knee is in careful hands. The second hands you the early-warning sign, so that if it ever happens, you'll recognise it and act quickly rather than hoping it passes.
References
- Clinician's Brief. Meniscal disease in dogs and cats. Clinician's Brief. Available at:
- Fitzpatrick N, Solano MA, 2010. Predictive variables for complications after TPLO with stifle inspection by arthrotomy in 1000 consecutive dogs. Veterinary Surgery 39(4):460–474. doi:10.1111/j.1532-950X.2010.00663.x.
- Franklin SP, Gilley RS, Palmer RH, 2010. Meniscal injury in dogs with cranial cruciate ligament rupture. Compendium on Continuing Education for the Practising Veterinarian 32(10):E1–E10.
- Kalff S, Meachem SL, Preston CA, 2011. Incidence of medial meniscal tears after arthroscopic assisted tibial plateau leveling osteotomy. Veterinary Surgery 40(8):952–956. doi:10.1111/j.1532-950X.2011.00910.x.
- Luther JK, Cook CR, Cook JL, 2009. Meniscal release in cruciate ligament intact stifles causes lameness and medial compartment cartilage pathology in dogs 12 weeks postoperatively. Veterinary Surgery 38(4):520–529. doi:10.1111/j.1532-950X.2009.00520.x.
- RCVS Knowledge Canine Cruciate Registry. Meniscal tears: information for dog owners. RCVS Knowledge. Available at:
- Ritzo ME, Ritzo BA, Siddens AD, Summerlott S, Cook JL, 2014. Incidence and type of meniscal injury and associated long-term clinical outcomes in dogs treated surgically for cranial cruciate ligament disease. Veterinary Surgery 43(8):952–958. doi:10.1111/j.1532-950X.2014.12220.x.
- Thieman KM, Pozzi A, Ling HY, Lewis D, 2010. Comparison of contact mechanics of three meniscal repair techniques and partial meniscectomy in cadaveric dog stifles. Veterinary Surgery 39(3):355–362. doi:10.1111/j.1532-950X.2010.00661.x.
- Thieman KM, Tomlinson JL, Fox DB, Cook C, Cook JL, 2006. Effect of meniscal release on rate of subsequent meniscal tears and owner-assessed outcome in dogs with cruciate disease treated with tibial plateau leveling osteotomy. Veterinary Surgery 35(8):705–710. doi:10.1111/j.1532-950X.2006.00214.x.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine