Why It's Degeneration, Not an Injury
Dr. Alastair Greenway
MRCVS
A sentence I hear over and over, usually said quietly, usually while the owner looks at the floor: "I shouldn't have thrown the ball." "He only jumped off the sofa." There's nearly always a thread of guilt running through it, the sense that one ordinary moment broke a healthy dog.
I want to take that weight off you, because the science is genuinely on your side here. In people, a torn cruciate is usually an accident: a healthy ligament wrenched in one violent moment on a football pitch or a ski slope. In dogs, it's almost never that story. By the time your dog's cruciate gives way, it has usually been failing for a long time. The jump didn't cause it. The jump revealed it.
The slow fraying
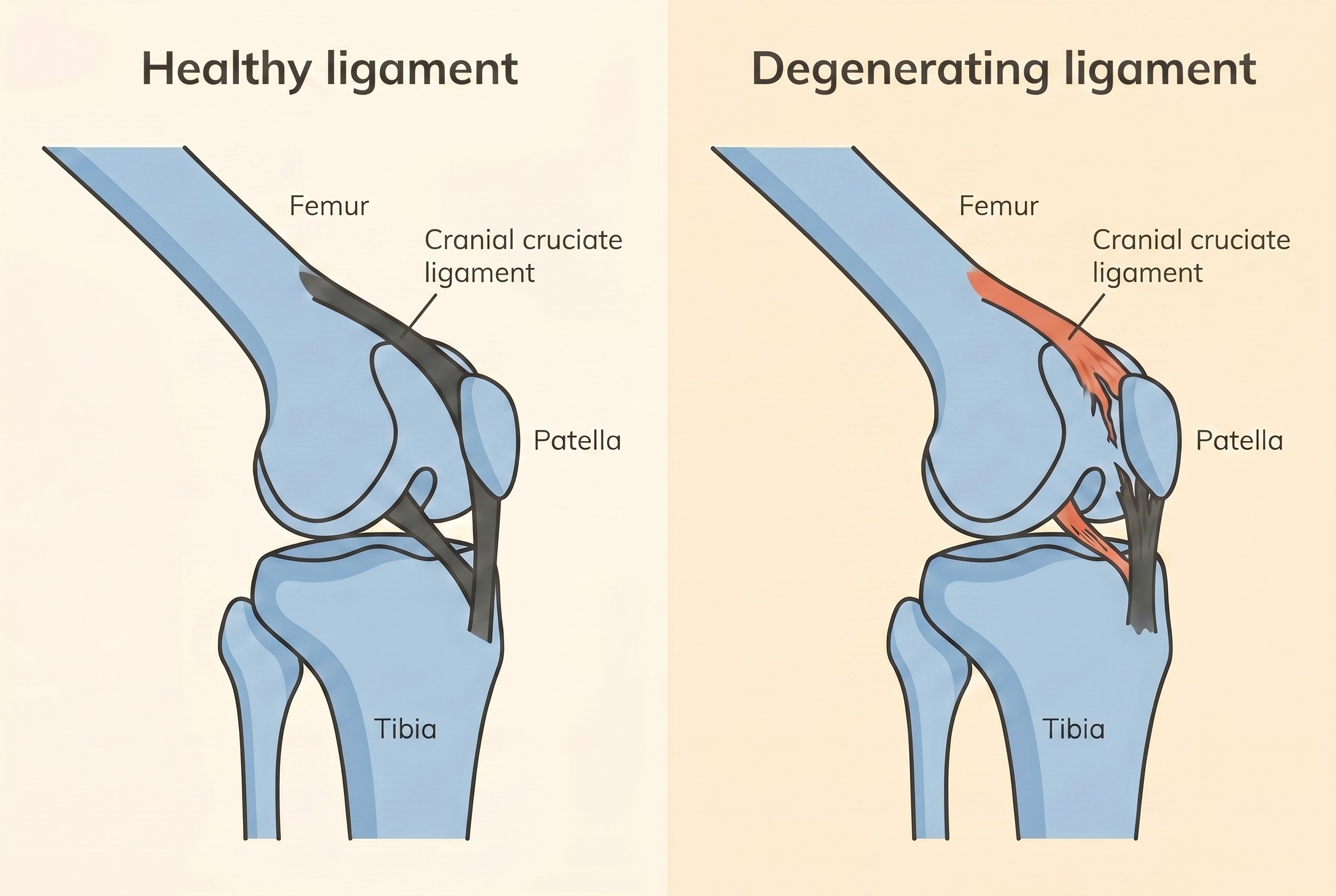
For a long time the textbooks described canine cruciate rupture the way they described a human one: wear and tear, then a traumatic snap. We now know that model was wrong, and it's been formally replaced. The modern understanding is that the cranial cruciate ligament is a progressive degenerative disease of the joint, in which the ligament's collagen matrix slowly breaks down and weakens, often silently, for months or even years before it finally fails (Comerford et al., 2011; Niebauer & Restucci, 2023). That's why the profession now talks about cruciate ligament disease rather than cruciate injury. The wording isn't pedantry. It reflects a completely different thing happening inside the knee.
The numbers make the point starkly. Only around 20% of canine cruciate cases can genuinely be put down to a traumatic event. The other 80% or so follow this slow degeneration of the ligament (Fauron & Perry, 2017). So for four dogs out of five, there was no accident at all in any meaningful sense. The ligament was quietly coming apart from the inside, and one ordinary movement was the last thing it could take.
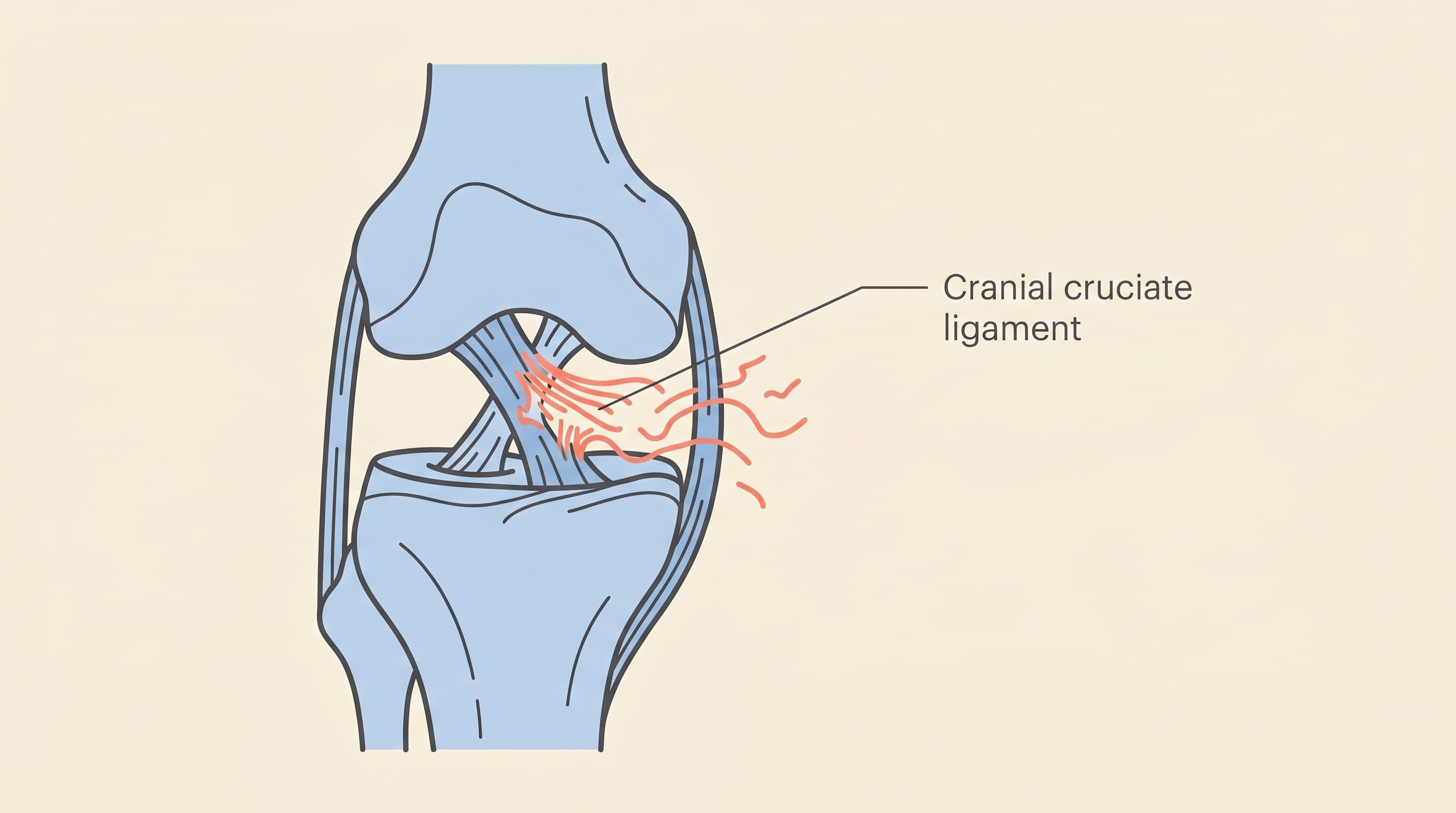
Put a degenerating cruciate under a microscope and you can actually see the fraying. The cells that maintain the ligament, the fibroblasts, are lost from its core, and the survivors change character, taking on a cartilage-like form in a process called chondroid metaplasia. The orderly architecture of the collagen falls apart too, losing the normal wavy "crimp" pattern that lets a healthy ligament stretch and recoil (Fauron & Perry, 2017). In plain English: the rope inside the knee slowly frays and stiffens from the inside out until it can't hold.
And it isn't only mechanical. There's a real immune and inflammatory component underneath. Inflammation of the joint lining, synovitis, is often present early, sometimes before the ligament has fully torn: in one study of 110 dogs, 56 (51%) had inflammatory lymphoplasmacytic synovitis at the time of cruciate surgery (Erne et al., 2009). Researchers have also found anti-collagen antibodies and immune complexes deposited within ruptured ligaments and joint capsules, and these appear to drive further collagen breakdown, the body's own immune system joining in on the unravelling (Niebauer & Restucci, 2023). Conformation loads the dice too: a steep slope to the top of the shin bone increases the forward shear force on the ligament with every step, so the rope is under chronic strain on top of the biological decay (Niebauer & Restucci, 2023). Exactly which dogs carry that risk is a story in itself, covered in which dogs get it.
So the "moment" you keep replaying was real, but it was the last straw rather than the cause. Picture a frayed climbing rope: it might hold for weeks looking almost fine, then part on an ordinary day under ordinary load. Nobody would say the climber broke the rope by using it. The rope was already gone.
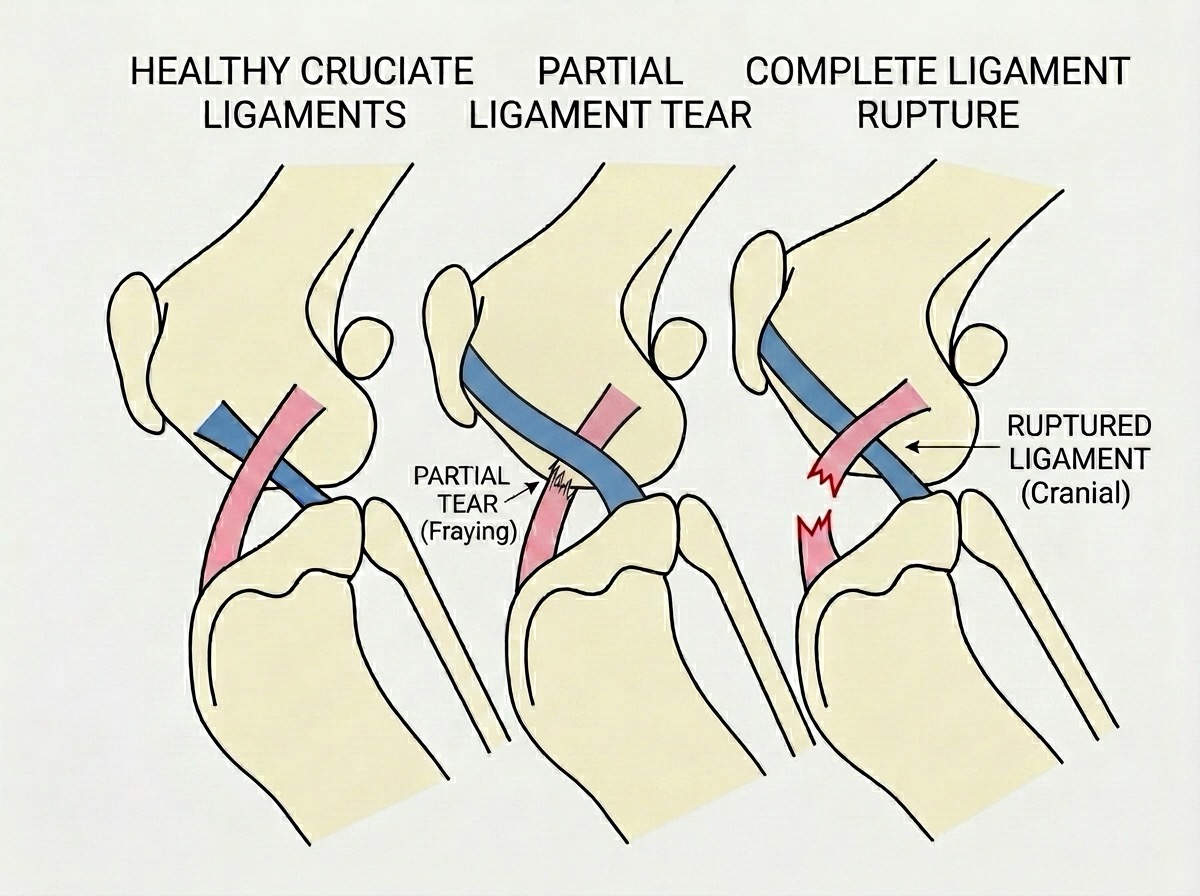
That timeline matters, because it means there's usually a long middle to this story before the full rupture. Healthy gives way to fraying, fraying to a partial tear, and only then to complete rupture. The partial tear is a tricky, important stage in its own right. If your dog has that diagnosis, or an intermittent limp no one can quite pin down yet, that's its own conversation, and I'd send you to the guide on partial cruciate tears rather than cover it here.
(One aside for completeness: cats can rupture their cruciate too, but it's far rarer in them, and when it happens it's more often a genuine one-off injury. This degenerative picture is very much a dog story, which is why this whole space is written for dogs.)
None of this was your doing
You did not do this to your dog.
I mean that as a clinical statement, not just a kind one. The ligament was already structurally compromised long before the day it failed. If it hadn't given way on the sofa, it would have gone on the stairs, or on a turn in the garden. The degeneration had been underway for months, and no realistic change in how you walked or played with your dog would have stopped a ligament already coming apart at the cellular level (Comerford et al., 2011; Fauron & Perry, 2017). The ball didn't cause the disease. It just happened to be there at the end of it.
I labour this because the guilt gets in the way. Owners who blame themselves sometimes hesitate over the very decisions that will help their dog most, as though a "natural" failure means they should somehow fix it naturally. None of that serves the dog in front of you. This is a recognised disease with a recognised course, you didn't engineer it, and the useful question now is simply what to do next.
What it means for the other knee
There's a hard truth that follows from all this, and I'd rather you heard it from me, gently and early, than stumbled on it in a forum at midnight. Because cruciate disease is a body-wide degenerative process and not bad luck in one joint, the same thing is usually quietly going on in the other knee. This isn't speculation. In a large study following 380 affected dogs, 54% went on to rupture the cruciate in their second knee too, with a median time to that second rupture of around 947 days, roughly two and a half years (Muir et al., 2011). As a working figure, the larger studies put the contralateral risk at around a third to a half, typically within one to two years. The most telling finding, though, was molecular: the pattern of T-lymphocyte gene activity in the first affected joint actually predicted which dogs would later rupture the second (Muir et al., 2011). That's about as clear as evidence gets that this is one shared disease expressing itself in both stifles, not two separate accidents befalling the same unlucky dog.
I'm flagging it here only so the concept lands: same disease, both knees. It shapes how you plan, budget and watch your dog over the next couple of years, and that deserves more than a paragraph. When you're ready, the bilateral risk is where that conversation lives. For now, keeping the other leg in mind is sensible foresight, not pessimism.
How it shapes the treatment choices
Once you see this as degeneration rather than injury, the treatment logic stops feeling arbitrary and starts to make sense.
Start with surgery. If a healthy ligament had snapped, you might expect a surgeon to stitch the two ends back together, the way they might repair a torn tendon. But the cruciate hasn't cleanly snapped. It has degenerated. There are no two good ends to rejoin, just frayed, diseased tissue that was already failing. That's why modern cruciate surgery doesn't try to repair the old ligament at all. The goal instead is to stabilise the joint by another route, so the knee can work without relying on a ligament that's gone. It's worth being clear that this fixes the mechanical problem, the instability, rather than curing the underlying disease, which is one reason the cartilage cushion called the meniscus can be torn at the outset or later on (a separate issue, covered in the meniscus guide). How stabilisation is achieved, and which method suits which dog, is the surgeon's territory, covered in the surgery decision guide and the procedure guides beyond it. Which procedure is "best" is never a verdict I'd hand down from an article: it's an individualised judgement your surgeon makes with your dog in front of them.
The same logic explains why doing nothing surgical can still work for some dogs. Once the joint is unstable, the body lays down scar tissue, peri-articular fibrosis, around it, and over time that can provide a degree of stability of its own. That's the principle conservative management leans on, supported by weight control, controlled exercise, physiotherapy and pain relief. For the right dog, it's real medicine, not a consolation prize.
But I have to be straight about which dog. The evidence does favour surgical stabilisation in large, active dogs. In a study of overweight dogs, TPLO plus conservative care gave a successful outcome in 75% at one year, against 63.6% for conservative care alone, and the gap was far wider earlier on, 92.6% versus 33.3% at 24 weeks (Wucherer et al., 2013). So conservative care is a real option that helps a meaningful number of dogs, and the right call for many small, light, older or comorbid patients, but it shouldn't be oversold to a big athletic dog, nor dismissed for a small, sensible one. Where your own dog sits on that spectrum is exactly the kind of individual judgement the conservative management guide is written to help you weigh, alongside your vet. If you'd like a structured way to talk it through, our decision helper walks you through the same factors a vet would weigh.
One last thing belongs here, because it's the most common misunderstanding I meet. Surgery limits arthritis. It does not prevent it. Once a knee has been unstable, some degree of osteoarthritis in that joint is essentially inevitable, and stabilising it slows that progression rather than stopping it. We can see this on X-rays: OA continues to advance after a TPLO, visible from as early as three months post-operatively, even as the dog's weight-bearing function recovers well and stays good out to three years (Shimada et al., 2020). So please don't let anyone, including a well-meaning website, tell you an operation makes arthritis a non-issue. That lifelong picture is its own subject, and cruciate disease and arthritis takes it on properly.
Understanding cruciate disease as exactly that, a disease with a slow course rather than an accident in a single moment, is the key that makes sense of everything else in this space. It's why the surgeon talks about stabilising rather than fixing, why we keep an eye on the other leg, why conservative care suits some dogs and not others, and why arthritis is part of the long game whatever you decide. If you'd like the wider overview first, the complete guide to cruciate disease is the piece to read. And whatever path lies ahead, let go of the idea that you caused this with a ball or a sofa. You didn't. You're just the one who's now going to help them through it.
References
- Comerford, E. J., Smith, K., & Hayashi, K. (2011). Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Veterinary and Comparative Orthopaedics and Traumatology, 24(2), 91-98.
- Erne, J. B., Goring, R. L., Kennedy, F. A., & Schoenborn, W. C. (2009). Prevalence of lymphoplasmacytic synovitis in dogs with naturally occurring cranial cruciate ligament rupture. Journal of the American Veterinary Medical Association, 235(4), 386-390.
- Fauron, A., & Perry, K. (2017). Canine cranial cruciate ligament disease, part 1: pathophysiology. Veterinary Times, 19 June 2017.
- Muir, P., Schwartz, Z., Malek, S., Kreines, A., Cabrera, S. Y., Buote, N. J., Bleedorn, J. A., Schaefer, S. L., Holzman, G., & Hao, Z. (2011). Contralateral cruciate survival in dogs with unilateral non-contact cranial cruciate ligament rupture. PLoS ONE, 6(10), e25331.
- Niebauer, G. W., & Restucci, B. (2023). Etiopathogenesis of canine cruciate ligament disease: a scoping review. Animals, 13(2), 187.
- Shimada, M., Mizokami, N., Ichinohe, T., Kanno, N., Suzuki, S., Yogo, T., Harada, Y., & Hara, Y. (2020). Long-term outcome and progression of osteoarthritis in uncomplicated cases of cranial cruciate ligament rupture treated by tibial plateau levelling osteotomy in dogs. Journal of Veterinary Medical Science, 82(7), 908-916.
- Wucherer, K. L., Conzemius, M. G., Evans, R., & Wilke, V. L. (2013). Short-term and long-term outcomes for overweight dogs with cranial cruciate ligament rupture treated surgically or nonsurgically. Journal of the American Veterinary Medical Association, 242(10), 1364-1372.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine