Partial Cruciate Tears: The Tricky Early Stage
Dr. Alastair Greenway
MRCVS
Lame, then fine, then lame again. That on-and-off pattern is what brings a lot of dogs into my consulting room with a partial cruciate tear, and it tends to come with a frustrating conversation. Your vet has felt the knee, frowned a little, used the words "partial tear", and then said something that sounded a lot like "let's see how it goes". You came home wanting a clear answer (operate now, wait, or manage) and instead you've got a maybe. That's an unsettling place to sit, and the uncertainty isn't your vet being vague. It's the nature of the thing.
A partial cruciate tear is a real, distinct stage of cruciate disease, not a near miss and not a sprain that will quietly heal. It's the middle ground most pages online skip straight past, jumping from a healthy knee to a fully ruptured one as if there were nothing in between. There is, and your dog is in it. So let me walk you through what a partial tear is, why it's so hard to pin down, what tends to happen next, and what your options are while you've still got time to think rather than react. For the whole arc of the disease, the complete guide is the place to start; this one zooms in on the awkward early chapter.
What a partial tear actually is
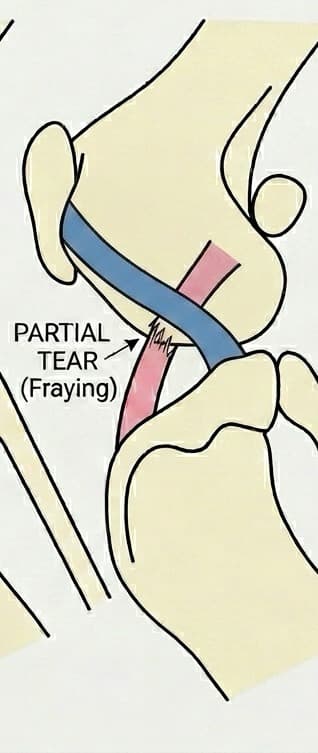
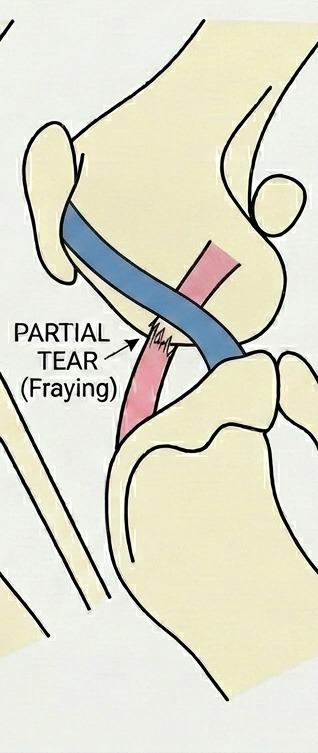
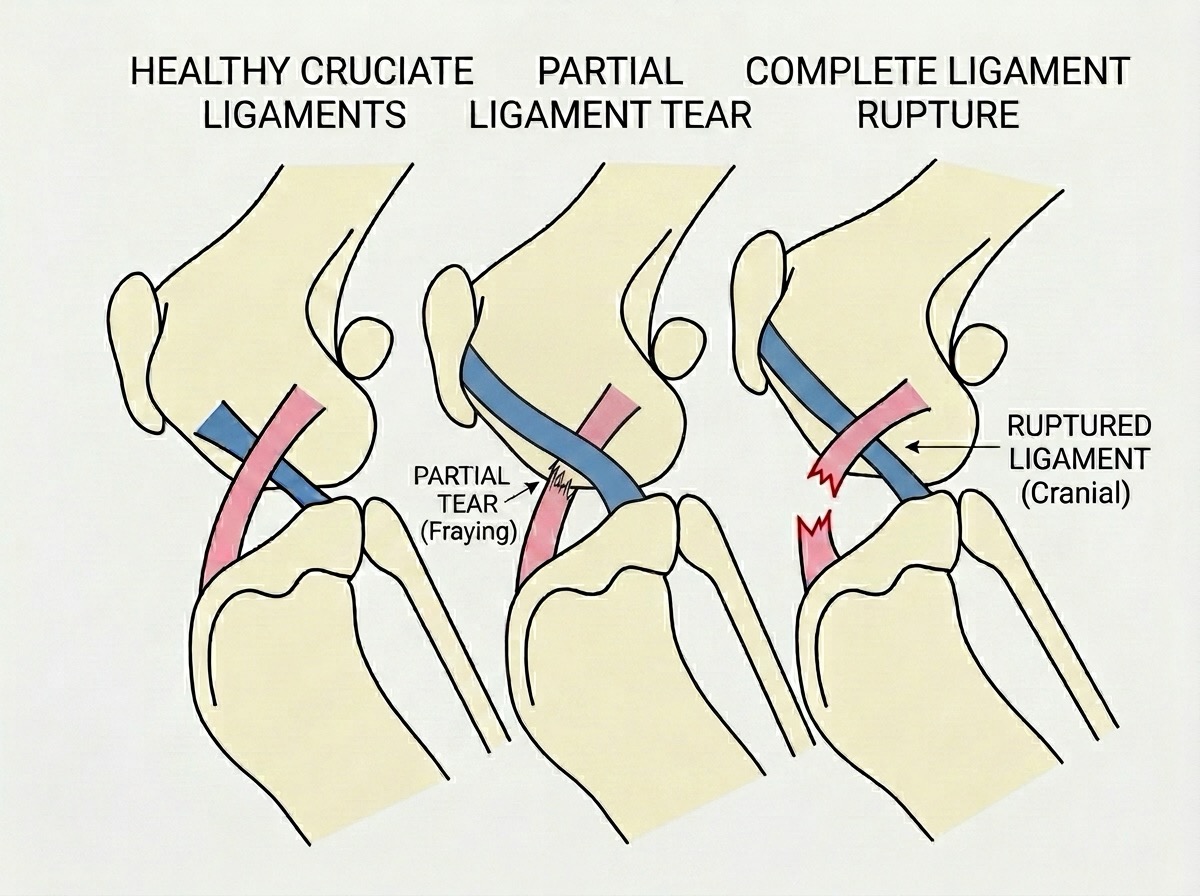
The cranial cruciate ligament, the CCL, isn't a single solid cord. It's made of two functional bands, the craniomedial and the caudolateral, which take up the strain at different angles as the knee bends and straightens. In a partial tear, the fibres of one band give way while the other stays intact, so the joint is only partly unstable. In the landmark case series, it was the craniomedial band that had ruptured in 20 of 25 dogs (Scavelli et al., 1990). That's the structural heart of it: some fibres have gone, some are still holding on, and the knee is wobbly in some positions but not others.
This is why the lameness can be so maddeningly inconsistent. A dog with a fully ruptured cruciate is usually clearly, persistently lame. A dog with a partial tear can limp after a long walk, trot around the garden next morning as if nothing's wrong, then pull up sore again after chasing a ball. The leg isn't fine, but it isn't obviously broken either, and that on-and-off pattern is what sends owners back and forth to the vet chasing an answer that keeps slipping away.
There's one point here I most want you to take on board. A partial tear is not a fresh sports injury that arrived the day your dog skidded on the kitchen floor. In dogs, cruciate rupture results from "subtle, slow degeneration that has been taking place over a period of time rather than the result of a sudden trauma to an otherwise healthy ligament" (American College of Veterinary Surgeons, 2024). The ligament has been quietly fraying from the inside for months, sometimes years, as part of a progressive degenerative process within the joint (Comerford et al., 2011). The partial tear is simply that fraying caught in the act, halfway through, and the jump off the sofa was the moment it became obvious, not the cause. That's the lens that makes everything else here make sense, and we give it the full treatment in why it's degeneration, not an injury.
Why it's so hard to diagnose
If your vet seemed less than certain, they were being straight with you. The classic test for cruciate failure is the cranial drawer sign, where the vet holds the thigh bone steady and tries to slide the shin bone forward. In a complete rupture the shin slides forward easily. But in a partial tear, the intact band can keep the joint feeling deceptively solid. Because the caudolateral band is taut when the knee is extended but slack when it's flexed, a craniomedial-band partial tear classically gives drawer movement only when the knee is bent, and none with the leg straight. In that 25-dog series, only 13 of the 25 dogs had any detectable drawer sign at all, 9 of those only in flexion, and 12 had none whatsoever (Scavelli et al., 1990). In nearly half of confirmed partial tears, the standard test came up empty.
So a quiet examination doesn't mean a quiet ligament. Stifles with partial rupture can be "stable with ligament fiber rupture evident with arthroscopic examination" (Sample et al., 2017): the joint can feel solid to skilled hands while the ligament inside is already visibly damaged. That's the real tension at the centre of this stage, and it's why a tidy yes or no isn't always on offer at the first visit.
It also explains the suggestions that can feel like over-caution. Cruciate disease is "easy to diagnose in acute, complete ruptures, but may be more subtle in chronic or partial tears", and a clear answer may need mild sedation so a tense dog stops guarding the joint, plus radiographs (American College of Veterinary Surgeons, 2024). The definitive confirmation is a direct look inside by arthroscopy, where the torn fibres and inflamed lining can be seen (Sample et al., 2018). Most dogs don't need to go that far, and we lay out the full exam-and-imaging pathway in how cruciate disease is diagnosed. The takeaway: if the diagnosis felt uncertain, that's normal, not a failing on anyone's part.
Where it's likely to go
This is the question every owner asks, and it deserves a straight answer. Most partial tears do go on to become complete ruptures. The ACVS puts it plainly: partial tearing "is common in dogs and almost always progresses to a full tear over time" (American College of Veterinary Surgeons, 2024). In one prospective study, 8 of 27 partial-rupture stifles, just under a third, had progressed to complete rupture by twelve months, at a median of 214 days (Sample et al., 2018). That study is also quietly important for what it failed to find: it tested an intra-articular platelet-rich-plasma and collagen "repair" aimed at saving the partial ligament, and it did no better than untreated historical controls at preventing progression (Sample et al., 2018). There's no proven way to reliably halt a partial tear mid-stream.
Let me hold two things in balance. Progression is the rule, so I'd be doing you a disservice to imply this might just resolve on its own. But "almost always, over time" is not a deadline. I can't tell you it will give way in six weeks or six months, because nobody can. Some dogs go on for a long while in this partial state; others tip over quickly. What I can tell you is the direction of travel, and that is the most useful thing to plan around.
There's one more reason a partial tear matters more than its modest symptoms suggest. As the joint shifts abnormally, the cartilage cushion inside the knee, the meniscus, gets caught and worn by the movement, and a meniscal tear can in turn cause or worsen the lameness (RCVS Knowledge, 2024). So a knee that looks like a minor on-and-off limp can be quietly accumulating a second problem. The meniscus has its own full story in the other injury in the knee.
Weighing up your two roads
So if it's probably going to progress and nothing reliably stops it, what do you do? You've essentially got two roads, and the partial stage is the rare luxury of choosing between them calmly rather than in a crisis.
The first is early surgical stabilisation: treating the knee now, on the basis that it's likely heading for full rupture anyway, and getting ahead of the wear that instability causes. The second is watchful conservative management: weight control, controlled exercise, physiotherapy and pain relief, with a close eye on the leg, accepting that you may move to surgery later if it progresses. Neither is a fudge, and neither is giving up.
What steers the choice is mostly your dog's size, activity and the degree of instability. For large, active dogs the evidence leans surgical. In a trial of overweight dogs with cruciate rupture, every dog got the conservative basics of weight loss, rehabilitation and pain relief, and half also had a TPLO, a bone-reshaping stabilisation. At 52 weeks, 75.0% of the surgical dogs had a successful outcome against 63.6% of those managed without surgery (Wucherer et al., 2013). A broader systematic review reached a similar steer: osteotomy techniques such as TPLO tend to give the most consistent return to function, though the authors were clear the overall quality of evidence is limited (Bergh et al., 2014).
Now read that Wucherer number the other way, because it matters just as much: close to two thirds of the dogs managed without surgery still reached a successful outcome (Wucherer et al., 2013). For a smaller, lighter, older or comorbid dog, conservative management is real medicine with a genuinely good chance of a comfortable result, not a consolation prize. The mistake I see in both directions is treating one route as the "proper" answer. Surgery isn't over-treatment for a big athletic dog, and conservative care isn't second best for a small steady one. I won't write the decision out for your dog here: weigh it through in surgery or not, read the candid case for the non-surgical route in conservative management, and if it helps to organise your thinking, the Decision Helper surfaces the right questions rather than handing you a verdict.
Two caveats while you weigh it. First, the other knee. Around half of dogs go on to rupture the contralateral cruciate; in one Labrador study 48% did so at a median of 5.5 months (Buote et al., 2009), and the ACVS cites up to 50%, usually within 12 to 18 months (American College of Veterinary Surgeons, 2024). I mention it not to alarm you but because it belongs in any sensible plan; the detail lives in will the other leg go too?. Second, and I won't soften this: stabilising the joint slows arthritis but doesn't abolish it. In partial-rupture stifles the degree of radiographic osteoarthritis already tracked with how much the ligament fibres were damaged (Sample et al., 2017), so the arthritis is underway before the ligament has fully gone. Surgery limits that long game rather than resetting it, as we cover in cruciate disease and arthritis.
So where does that leave you, sitting with a maybe? In a better position than it feels. A partial tear is the one stage of this disease that hands you time, and time spent planning beats time spent reacting. While the leg is only partly affected, you can get the weight off, have the frank conversation with your vet about which road suits your dog, and set a baseline rather than waiting for a sudden lame morning to force your hand. The uncertainty is real, but so is the head start.
References
- American College of Veterinary Surgeons. (2024). Cranial Cruciate Ligament Disease. ACVS Small Animal patient resource.
- Bergh, M. S., Sullivan, C., Ferrell, C. L., Troy, J., & Budsberg, S. C. (2014). Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. Journal of the American Animal Hospital Association, 50(5), 315-321.
- Buote, N., Fusco, J., & Radasch, R. (2009). Age, tibial plateau angle, sex, and weight as risk factors for contralateral rupture of the cranial cruciate ligament in Labradors. Veterinary Surgery, 38(4), 481-489.
- Comerford, E. J., Smith, K., & Hayashi, K. (2011). Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Veterinary and Comparative Orthopaedics and Traumatology, 24(2), 91-98.
- RCVS Knowledge. (2024). Meniscal Tears. Canine Cruciate Registry, owner information.
- Sample, S. J., Racette, M. A., Hans, E. C., Volstad, N. J., Holzman, G., Bleedorn, J. A., Schaefer, S. L., Waller, K. R., Hao, Z., Block, W. F., & Muir, P. (2017). Radiographic and magnetic resonance imaging predicts severity of cruciate ligament fiber damage and synovitis in dogs with cranial cruciate ligament rupture. PLoS ONE, 12(6), e0178086.
- Sample, S. J., Racette, M. A., Hans, E. C., Volstad, N. J., Schaefer, S. L., Bleedorn, J. A., Little, J. P., Waller, K. R., Hao, Z., Block, W. F., & Muir, P. (2018). Use of a platelet-rich plasma-collagen scaffold as a bioenhanced repair treatment for management of partial cruciate ligament rupture in dogs. PLoS ONE, 13(6), e0197204.
- Scavelli, T. D., Schrader, S. C., Matthiesen, D. T., & Skorup, D. E. (1990). Partial rupture of the cranial cruciate ligament of the stifle in dogs: 25 cases (1982-1988). Journal of the American Veterinary Medical Association, 196(7), 1135-1138.
- Wucherer, K. L., Conzemius, M. G., Evans, R., & Wilke, V. L. (2013). Short-term and long-term outcomes for overweight dogs with cranial cruciate ligament rupture treated surgically or nonsurgically. Journal of the American Veterinary Medical Association, 242(10), 1364-1372.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine