
How Cruciate Disease Is Diagnosed
Claire Greenway
BVM&S MRCVS
In the consulting room, a vet who suspects a cruciate problem will bend and push the limping leg in a particular way, and a few minutes later may start talking about sedation, X-rays and surgery. It can all happen quickly. So why does the leg get handled like that? Why raise sedation or an X-ray, when the vet seems to know already? And how sure is anyone, really, that this is the cruciate?
Let me walk you through it properly, because the cruciate is one of the more recognisable orthopaedic problems once you know what a vet is feeling for, and an informed owner is a calmer partner in what comes next. This piece sits underneath the complete guide to cruciate disease, which is the place to start if you want the whole picture. Here I'll stay tightly on one question: how does the vet actually know?
The short version is that this is diagnosed mostly with hands, not machines. A skilled hands-on orthopaedic examination is the heart of it, backed up by imaging where it's needed, and in a clear-cut case a confident diagnosis can usually be reached on the exam alone (Rafla et al., 2025; ACVS, n.d.). Let me show you what the hands are doing.
Reading the joint by hand
There are two manipulations a vet relies on, and both are testing the same thing: is the shin bone sliding forward when it shouldn't?
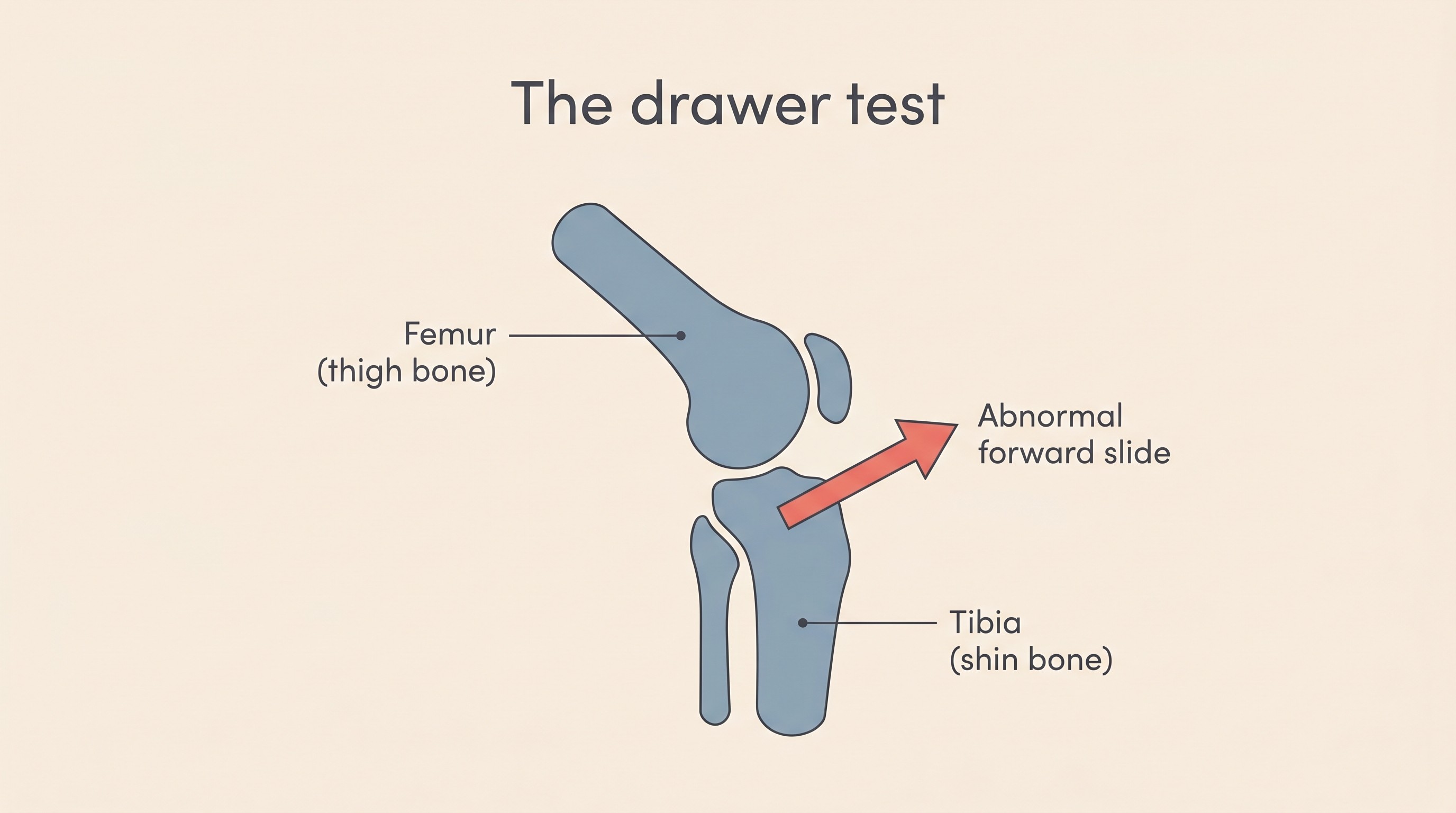
The first is the cranial drawer test. The vet steadies the thigh bone with one hand and, with the other, tries to slide the top of the shin bone forwards. In a healthy knee, the cruciate holds firm and almost nothing moves. If the ligament has failed, the shin slides forward like a drawer pulling open, and that abnormal movement is a positive drawer sign (ACVS, n.d.).
The second is the tibial compression test, sometimes called the cranial thrust test. Here the vet flexes the hock (the ankle) while holding the knee still, which loads the joint in a way that mimics weight-bearing and reproduces that same forward slip of the shin (ACVS, n.d.; Rafla et al., 2025). It's a clever test, because it recreates the real-life forces the knee feels when your dog stands and walks. Either a positive drawer or a positive thrust is enough to confirm cruciate instability (ACVS, n.d.).
Now for the frank bit that a lot of pages skip. These tests can quietly under-read in exactly the dogs you'd most expect to have the problem. A big, anxious or sore dog will brace the leg, and that muscle guarding can hold the joint together well enough to mask the very movement the vet is trying to feel, producing a false-negative (Rafla et al., 2025). The research bears this out: the sensitivity of the manual drawer and compression tests was, in the authors' own word, "surprisingly low" in fully conscious dogs, and significantly better once the dog was under general anaesthesia and the muscles could finally relax (Carobbi & Ness, 2009).
This is why your vet might say they want to sedate your dog, or do a short general anaesthetic, to be sure. It can feel like a step up, or a sign something has gone wrong. It isn't. It simply means they want the muscles to stop fighting them so they can get a clean, truthful answer from the joint (Carobbi & Ness, 2009; Rafla et al., 2025; ACVS, n.d.). A sedated exam is often the kindest and most decisive thing you can do, especially in a nervous large-breed dog.
There's one situation where even a good pair of hands stays unsure, and that's a partial tear. When only some of the ligament fibres have frayed and the rest are still doing their job, the joint is only a little loose, so the drawer sign can be subtle, come and go, or be absent altogether. Partials are genuinely the hard ones to be certain about, and they deserve their own explanation, so if your vet has used the word "partial" or simply said they're not yet sure, the guide to partial tears is the one to read next. For our purposes here, the important thing is that a sedated exam, imaging, and occasionally a keyhole look are exactly how that uncertainty gets resolved.
What the X-ray can and can't show
If your vet suggests X-rays, it helps to know what they will and won't show, because owners are often surprised.
An X-ray does not show the cruciate ligament itself. The ligament is soft tissue, and plain radiographs simply don't render it: you cannot photograph the torn ligament the way you might imagine (Rafla et al., 2025). What X-rays show instead are the secondary signs, the footprints the problem leaves behind in the joint.
The earliest and most consistent of these is joint swelling. Fluid builds up inside an irritated knee, and on the X-ray it blots out a normally crisp little pocket of fat at the front of the joint (the infrapatellar fat pad). When that dark fat shadow is lost or smudged, it's a reliable early flag that the joint is unhappy (Carobbi & Ness, 2009; Rafla et al., 2025). In more long-standing cases the X-ray also shows osteophytes, the small spurs of arthritic new bone that grow around the edges of the kneecap and the joint surfaces once instability has been grinding away for a while (Rafla et al., 2025). And on a special stress view, taken with the hock flexed to load the joint exactly as the compression test does, the X-ray can actually catch the shin in the act of slipping forward (de Rooster et al., 1998).
That stress radiograph is worth dwelling on, because it shows how imaging and hands work together rather than competing. In one study of surgically confirmed ruptures, the stress (tibial-compression) view detected instability in 97% of knees, against 86% for the manual drawer test in the very same dogs, with extremely high specificity for both (de Rooster et al., 1998). I read that not as "X-ray everything," but as fair reassurance: imaging can occasionally catch a slip the hand has missed, which is exactly why a vet reaches for it when the exam leaves a question hanging.
X-rays do one more quiet job: they map the territory for surgery if it comes to that. The slope on the top of the shin bone, the tibial plateau angle (TPA), is measured from a side-on radiograph, and it's the number a surgeon planning a TPLO works their bone cut around (Today's Veterinary Practice, 2018). I'll leave the detail there, because which procedure suits your dog belongs to a later stage, not this one. The practical point is that radiographs are mostly needed when surgery is being planned, or to settle a difficult case, rather than as a routine box to tick on every limping dog (ACVS, n.d.).
When the exam needs backing up
For most dogs, that's the whole toolkit: a careful exam, sedated if necessary, and a couple of X-rays. Most dogs never need anything more advanced. But in complex, ambiguous or borderline-stable cases, there are further options, and it's worth knowing they exist so they don't sound alarming if mentioned.
CT gives exquisite bone detail and is most useful around surgical planning. MRI can image the soft tissues, the ligament and the meniscus, without going inside the joint. And then there's arthroscopy, which is the reference standard, the most definitive look of all (Rafla et al., 2025). Arthroscopy is keyhole surgery: a tiny camera is passed into the joint so the surgeon can see the ligament damage directly and inspect the rest of the knee at the same time, with the option to treat what they find in the one anaesthetic (Rafla et al., 2025).
One of the main things arthroscopy is looking for is the meniscus, the C-shaped cartilage cushion inside the knee. It's the other injury in the joint, frequently torn alongside the cruciate, and how often it's found depends heavily on how hard you look: in one large series, concurrent tears turned up in 44% of knees opened surgically but 83% of the same kind of knee inspected by keyhole camera (Ritzo et al., 2014). Like the ligament, it doesn't show on a plain X-ray, and it's best assessed at arthroscopy or surgery, which find more tears than the naked eye does through an open incision alone (Rafla et al., 2025). I won't go further here, because the meniscus has its own guide; for now it's enough to know it's part of what the more advanced look is checking, and a torn one matters.
Getting a clear answer
There's a reason I've been so candid about the grey areas, and it's this: the next decision after a cruciate diagnosis is usually a big one, often involving surgery and a significant bill, and you are completely entitled to want certainty before you walk through that door.
So if you find yourself wanting a second opinion, or your vet themselves suggests referral to an orthopaedic specialist who can offer the advanced imaging or arthroscopy, please don't read that as a failure of the first vet or a sign things are going badly. A second opinion on a decision of this size is a normal, sensible step, and no good clinician is offended by one. Who does that advanced work, and when a specialist is genuinely worth it, is covered properly in our guide on orthopaedic referral.
I'd add one piece of framing to carry forward, lightly. What the exam has uncovered is degeneration that was already underway, not a fresh injury from one unlucky jump, which is why the degeneration guide is worth a read when you're ready. And because this is so often a whole-dog tendency rather than bad luck in one joint, it's reasonable for your vet to have half an eye on the other knee for the future. Neither of those is something to dwell on today.
Let me leave you with the genuinely reassuring part. Between a careful, sometimes sedated examination and a couple of X-rays, most vets reach a confident diagnosis and a workable plan in a single visit. The cruciate gives itself away once you know what you're feeling and looking for, and the uncertainty I've been open about is the exception, not the rule. The harder question is the one that comes next: not whether it's the cruciate, but what to do about it, and that's where the surgery-or-not decision picks the journey up. You'll walk into that conversation knowing exactly how the answer was reached.
References
- American College of Veterinary Surgeons (n.d.) Cranial Cruciate Ligament Disease. Available at:
- Carobbi, B. and Ness, M.G. (2009) 'Preliminary study evaluating tests used to diagnose canine cranial cruciate ligament failure', Journal of Small Animal Practice, 50(5), pp. 224-226.
- de Rooster, H., Van Ryssen, B. and van Bree, H. (1998) 'Diagnosis of cranial cruciate ligament injury in dogs by tibial compression radiography', Veterinary Record, 142(14), pp. 366-368.
- Rafla, M., Yang, J. and Mostafa, A. (2025) 'Canine Cranial Cruciate Ligament Disease (CCLD): A Concise Review of the Recent Literature', Animals, 15(7), 1030. doi:10.3390/ani15071030.
- Ritzo, M.E., Ritzo, B.A., Siddens, A.D., Summerlott, S. and Cook, J.L. (2014) 'Incidence and type of meniscal injury and associated long-term clinical outcomes in dogs treated surgically for cranial cruciate ligament disease', Veterinary Surgery, 43(8), pp. 952-958.
- Today's Veterinary Practice (2018) Small Animal Cruciate Disease: The Tibial Plateau Angle. Available at:
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine