
Cruciate Ligament Disease: Understanding the Most Common Reason Dogs Need Knee Surgery
Dr. Alastair Greenway
MRCVS, 25 years clinical experience
A dog diagnosed with cranial cruciate ligament disease is in very common company. It's the single most common orthopaedic problem in dogs and the most frequent reason a dog ends up needing knee surgery. It's also one of the biggest causes of hind-limb arthritis, which is why it earns a detailed article in this space.
This is the first of our condition-specific surgical guides, sitting beneath the general article on the surgery decision, which I'd encourage you to read alongside this one. That article covers how to think about whether surgery is right, what recovery demands of you, and the questions worth asking. This one goes deep on cruciate disease specifically: what it is, how it's diagnosed, what the options actually are, and what to expect.
A word on what this article is and isn't. It's here to help you understand your dog's condition and walk into the conversation with your vet or surgeon informed and able to ask good questions. It is not here to tell you which procedure your dog should have. That decision belongs to you and your surgeon together, based on your individual dog, and a good surgeon's individualised judgement is worth far more than anything you'll read online, including here. My aim is to make you a well-informed partner in that conversation, not to second-guess it.
What the cranial cruciate ligament is, and what goes wrong
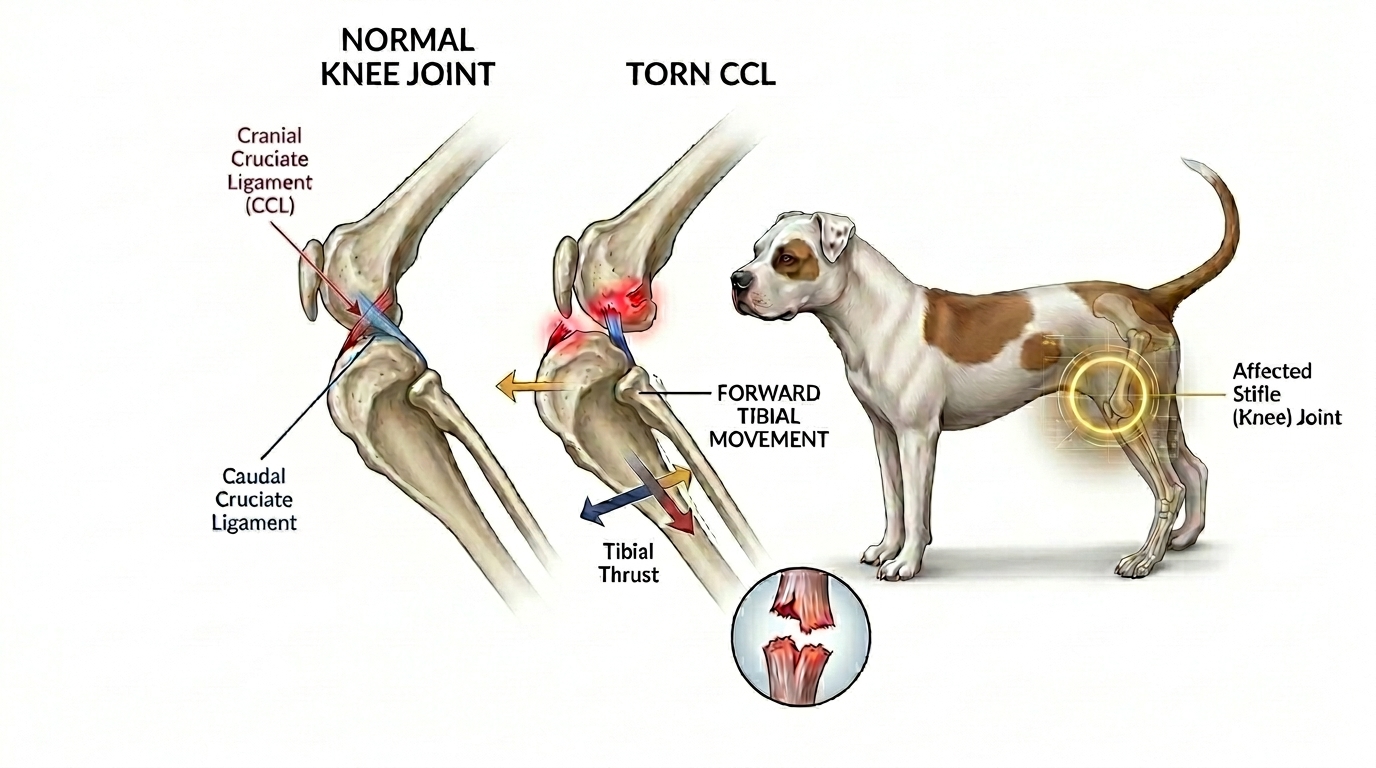
The cranial cruciate ligament, or CCL, is a band of tissue inside the knee, the stifle joint, that stops the shin bone sliding forward relative to the thigh bone when the dog bears weight. It's the dog's equivalent of the ACL in a human knee, and it does a similar job of keeping the joint stable through movement.
Now the part that surprises most owners, and it matters. In dogs, cruciate disease is usually not a sudden sporting injury the way an ACL tear often is in people. In most dogs it's a degenerative process: the ligament gradually weakens and frays over months or years, until it partially or completely fails, sometimes with a final dramatic moment but often as the culmination of a slow decline. That's why a dog can "do" their cruciate simply jumping off the sofa, when the real story is a ligament that had been deteriorating for a long time.
Several things raise the risk: larger breeds, being overweight, neutering, and conformation of the knee such as a steep tibial plateau angle, the slope of the top of the shin bone. Patellar luxation, which we cover in its own article, can also contribute, particularly in small breeds.
The degenerative nature also explains something owners find distressing: the high chance that the other knee will go too. Because the underlying problem is often a tendency in the dog rather than bad luck in one joint, a significant proportion of dogs who rupture one cruciate will rupture the other within a year or two. It's worth knowing this from the start, both so you're not blindsided, and because it matters for planning and budgeting.
Why it leads to arthritis
This is the link back to the heart of this space. A knee with a failed cruciate is an unstable knee, and an unstable joint is one that develops arthritis. Every time the dog bears weight, the abnormal movement damages the joint surfaces and the structures around them, driving inflammation and the progressive changes of osteoarthritis.
That has an important implication. Some degree of arthritis will develop in a cruciate-affected knee whether or not surgery is done; the instability has already started the process. But stabilising the joint, by whatever means, slows that process considerably compared with leaving it unstable. So the conversation is rarely "surgery prevents arthritis" versus "no surgery means arthritis." It's more accurate to say that addressing the instability gives the best chance of limiting the arthritis and keeping the dog comfortable and functional.
There's often a second structure involved, too: the meniscus, a cushion of cartilage in the knee, is frequently damaged alongside the cruciate, and meniscal damage is itself a significant source of pain. Whether and how the meniscus is dealt with is part of the surgical conversation.
Reaching a diagnosis
Your vet diagnoses cruciate disease through a combination of history, examination, and imaging.
On examination, the classic findings are an abnormal forward movement of the shin bone when the vet manipulates the joint, tests known as the cranial drawer sign and the tibial compression or thrust test. In a tense or painful dog these can be hard to elicit while the dog is awake, so sedation is sometimes needed for a clear assessment.
Imaging usually follows. X-rays don't show the ligament itself but reveal the secondary signs, joint swelling, arthritis, and the joint angles relevant to surgical planning. More advanced imaging, CT or MRI, gives more detail in complex cases, and arthroscopy, keyhole inspection of the inside of the joint, is considered the most definitive way to confirm the state of the ligament and the meniscus. Most dogs don't need the advanced imaging; examination plus X-rays is often enough to reach a diagnosis and a plan.
The treatment options
This is where owners most need clear, even-handed information, because there are genuinely several options and the "right" one depends heavily on the individual dog. I'll describe them plainly, including their trade-offs, but I'll say again: which is right for your dog is a decision for you and your surgeon, not a verdict I can deliver from here.
Surgical stabilisation
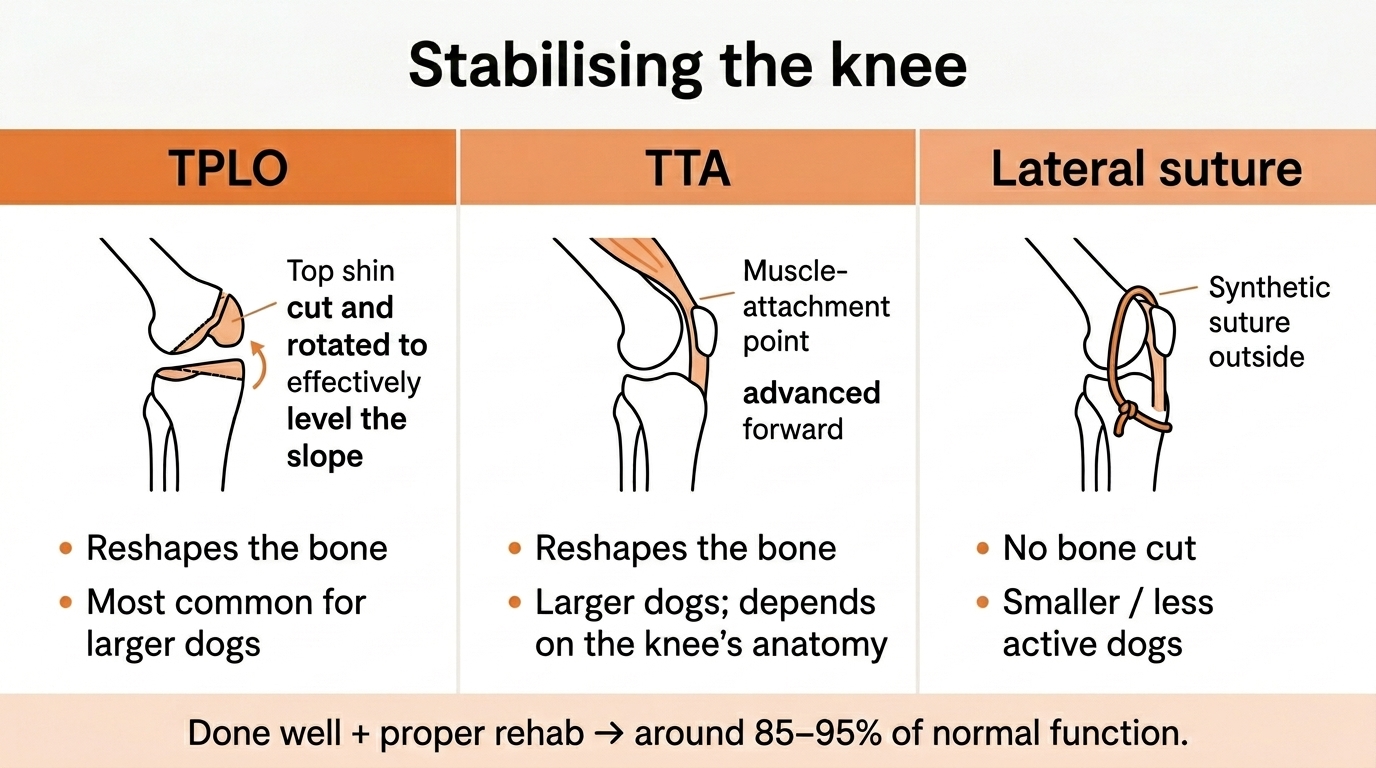
For most dogs, particularly larger and more active ones, surgery to stabilise the knee gives the best chance of a good return to function. There are three main approaches.
TPLO (tibial plateau levelling osteotomy) changes the geometry of the knee by cutting and rotating the top of the shin bone, so that the joint no longer needs the cruciate to stay stable during weight-bearing. It's currently the most commonly recommended procedure for larger dogs and is performed by making a precise cut in the bone and fixing it with a plate. It tends to give a strong, reliable return to function and carries a slightly lower major-complication rate than some alternatives, though no surgery is without risk.
TTA (tibial tuberosity advancement) is another bone-cutting procedure that achieves stability by a different geometric change, moving the point where the main thigh muscle attaches. It's also used mainly in larger dogs and has good outcomes; the choice between it and TPLO often comes down to the individual knee's anatomy and the surgeon's experience and preference.
Lateral suture (extracapsular stabilisation) is a less invasive technique that places a strong synthetic suture outside the joint to mimic the cruciate's function while the dog's own scar tissue builds up to provide longer-term stability. It involves no bone cut, is generally less expensive, and is most often used for smaller or less active dogs, or where the bone-cutting procedures aren't suitable or affordable.
Across the stabilisation techniques, owners can reasonably expect substantial improvement, in the region of 85 to 95 percent of normal function, when surgery is done well and followed by proper rehabilitation. Complication rates vary by procedure and patient; for TPLO, one large study reported a complication rate of around 15 percent, the majority of them minor.
Conservative (non-surgical) management
Surgery is not the only path, and it's not always the right one. For some dogs, particularly smaller, lighter, older, or less active ones, or where surgery isn't possible for health or financial reasons, conservative management can give a good quality of life. This means weight control, controlled exercise and physiotherapy, pain relief, and the home and lifestyle measures this whole guide describes, allowing the body to stabilise the knee with scar tissue over time.
It's a legitimate option, not a consolation prize, for the right dog. But it generally gives less reliable stability and return to function than surgery in larger active dogs, and the evidence overall tends to favour surgical stabilisation for those dogs. The right answer genuinely depends on the individual, which is exactly why this is a conversation rather than a formula.
What recovery actually involves

Recovery is the part owners most underestimate, and it's where the general surgery-decision article and its recovery-planning content really matter. Cruciate surgery is not a procedure after which the dog bounces back in a few days. It demands a serious, sustained commitment from you.
Recovery typically involves weeks of strict exercise restriction, often eight to twelve weeks, during which the dog must be kept calm, confined, and prevented from doing the very things, jumping, running, stairs, that they'll most want to do as they start feeling better. This is harder than it sounds; managing a recovering dog who feels well enough to misbehave but mustn't is genuinely demanding. There's controlled, gradually increasing exercise on a schedule, often guided by a physiotherapist, and rehabilitation such as hydrotherapy frequently plays a valuable role.
Before committing, it's worth being realistic with yourself about whether you can provide this: the confinement, the lead-only toilet trips, the weeks of restricted activity, the rehabilitation appointments, the supervision. The surgery's success depends heavily on the recovery being done properly, and the recovery depends on you. Our surgery-decision article includes recovery-planning content specifically to help you think this through before you commit.
Questions worth asking your surgeon
Walking into the conversation, these are the questions that tend to be most useful:
Which procedure do you recommend for my dog specifically, and why this one over the others? What's your experience and typical outcomes with it? What does recovery realistically involve, week by week? How will the meniscus be assessed and dealt with? What are the main risks and complications, and how often do they happen in your hands? What rehabilitation will my dog need, and can you help arrange it? What's the likelihood the other knee will need the same down the line? And, given the costs, what are the options at different price points?
A good surgeon will welcome these questions. The aim isn't to test them; it's to understand your dog's situation well enough to make the decision together with confidence.
The bottom line
Cruciate disease is common, it causes arthritis, and for most affected dogs something does need to be done to address the instability. Encouragingly, the outcomes, with appropriate treatment and committed rehabilitation, are generally very good: the large majority of dogs return to comfortable, active life.
There is rarely a single "correct" choice that applies to every dog. The best procedure for a 40-kilogram working dog may not be the best for a 6-kilogram elderly companion, and conservative management has its place for the right patient. What matters most is an accurate diagnosis, a frank conversation with a surgeon you trust, a clear-eyed understanding of what recovery will ask of you, and a commitment to doing the rehabilitation properly. Get those right, and your dog has every chance of a good outcome.
Read this alongside the surgery-decision article for the framework on deciding and planning recovery, and the specialist pain clinic article if your dog's pain needs more than the surgery alone provides. And use the questions above to make the conversation with your surgeon as useful as it can be.
References
- Bergh MS, Sullivan C, Ferrell CL, Troy J, Budsberg SC. Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. Journal of the American Animal Hospital Association, 2014;50(5):315-321.
- Fitzpatrick N, Solano MA. Predictive variables for complications after tibial plateau levelling osteotomy with stifle inspection by arthrotomy in 1000 consecutive dogs. Veterinary Surgery, 2010;39(4):460-474.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine