TPLO Explained: What It Is and Who It's For
Dr. Alastair Greenway
MRCVS
A TPLO is the operation most surgeons reach for when a dog tears its cruciate, and the acronym sounds a great deal more alarming than the procedure deserves. Once you have a date in the diary and a consent form to sign, the four letters tend to sit there looking ominous. So let me explain plainly what the operation actually does. TPLO sounds dramatic. Understanding it makes it a great deal less so.
This article assumes the decision to operate has been made, and that TPLO is the procedure on the table. If you are still weighing surgery against conservative care, that question belongs to the decision guide, and if you want the even-handed comparison of why TPLO was chosen for your dog over the alternatives, that is the comparison piece, not this one. My job here is narrower and, I hope, more useful the night before: to tell you plainly what a TPLO is, who it suits, what the outcomes really look like and what can go wrong.
What the surgeon actually does
Start with what a TPLO does not do. It does not stitch the torn ligament back together, and it does not replace it with anything. This surprises people, because the natural assumption is that knee surgery fixes the broken part. TPLO takes a different approach: instead of repairing the ligament, it changes the shape of the joint so the ligament is no longer needed.
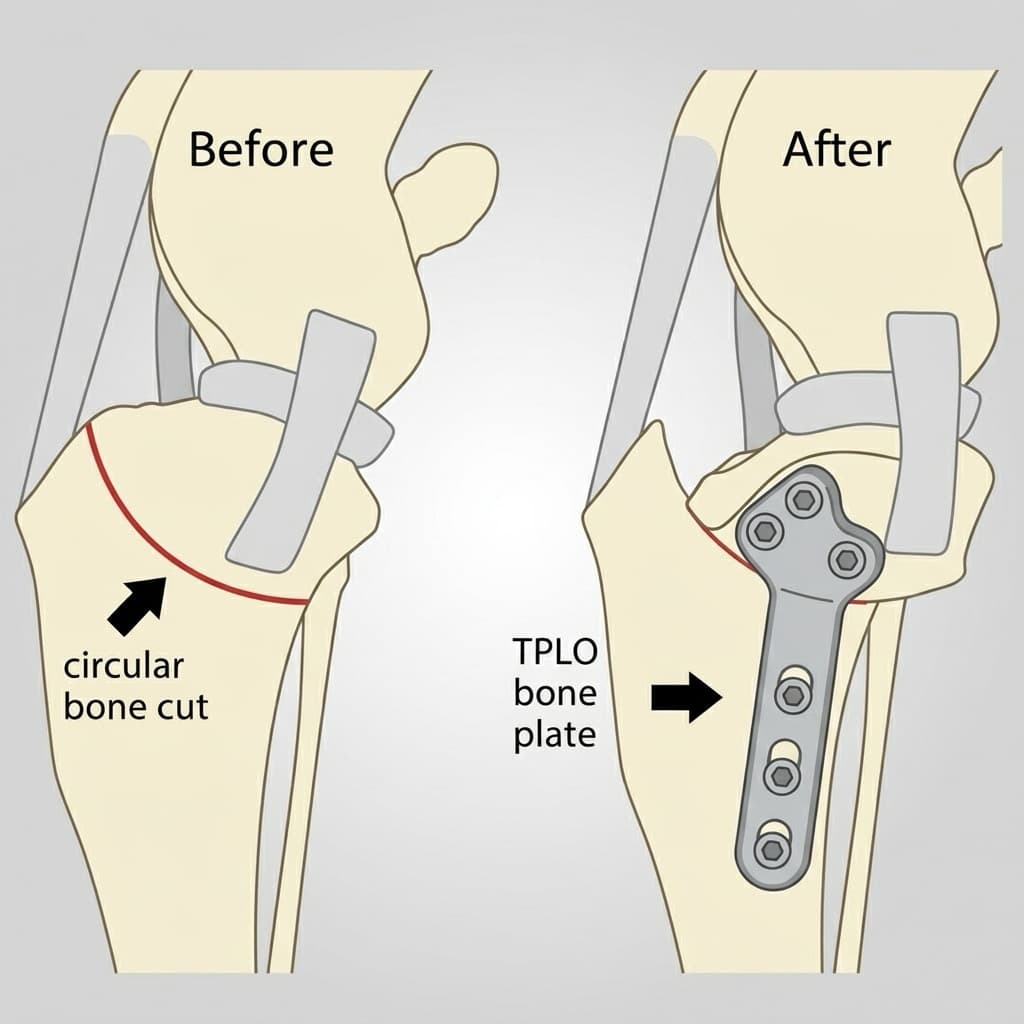
TPLO stands for tibial plateau levelling osteotomy, and the name, once unpacked, is simply a description of the operation. The top of the shin bone, the tibia, has a natural backward slope to it, called the tibial plateau. The surgeon makes a curved cut in the top of the tibia, rotates that piece of bone to flatten the slope, and holds it in place with a metal plate and screws. Once the slope is levelled, the knee no longer relies on the cruciate ligament to stop the shin sliding forward when the dog bears weight (Slocum & Slocum, 1993; Boudrieau, 2009). The joint becomes, in effect, self-stabilising.
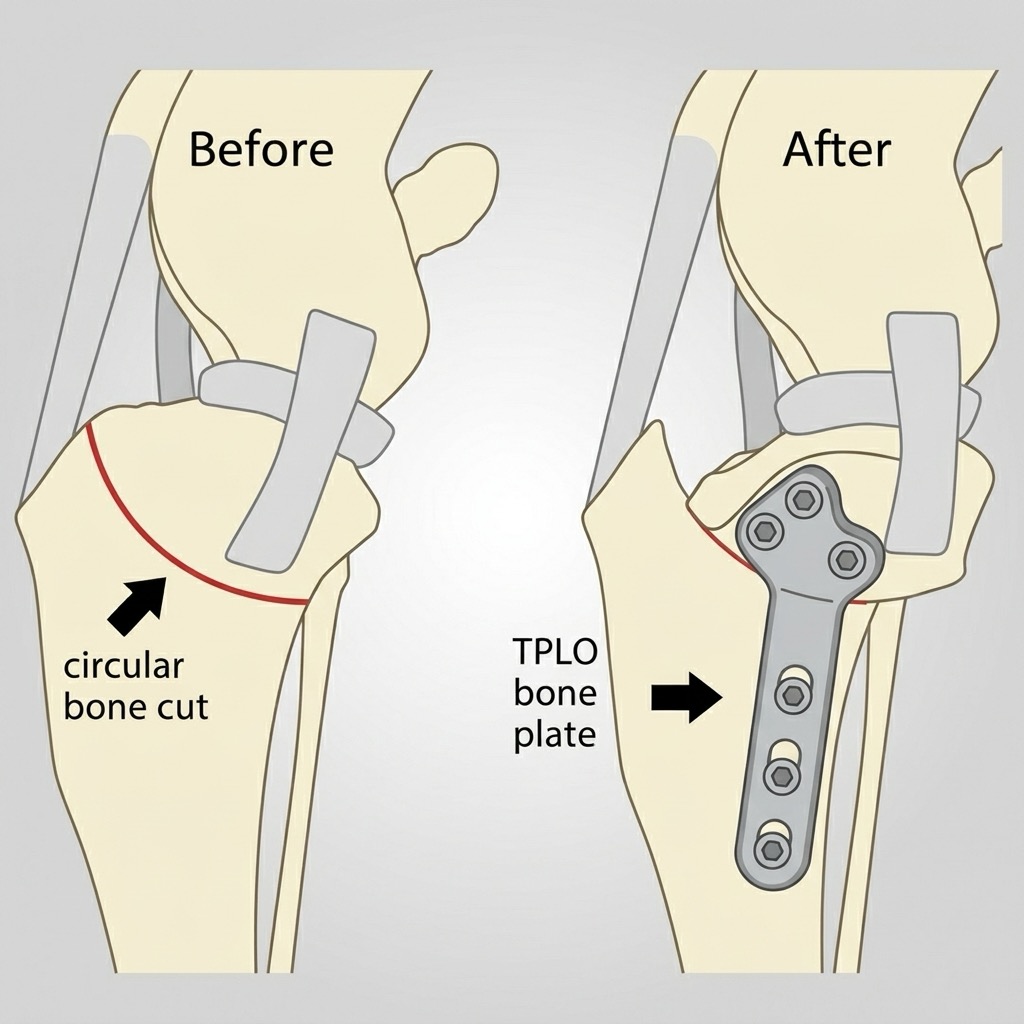
When a dog bears weight on a normal knee, that backward-sloping plateau makes the shin want to thrust forwards, and in a healthy joint the cruciate ligament is what holds it back. This forward push is called cranial tibial thrust. In a cruciate-deficient knee there is nothing to resist it, so every step lets the shin slide forwards, and that abnormal shearing movement is what makes the joint unstable and painful. Levelling the slope changes the direction of those forces. The thrust that used to shear the joint forwards becomes a squeezing, compressive force the joint tolerates comfortably, so the leg stays stable through the whole step with no working cruciate at all (Slocum & Slocum, 1993; Boudrieau, 2009; Kim et al., 2008). That is the whole idea: not a repaired ligament, but a knee that no longer needs one.
The plate and screws are designed to stay in for life. Implant removal is the exception rather than the rule, done only if the metalwork causes a problem later, such as a persistent infection or local irritation. For most dogs it simply stays put and is never thought about again.
The dogs it suits
TPLO is the most commonly recommended surgery for cruciate disease in dogs, and that is exactly why owners get sent home to research it (Bergh et al., 2014; Nanda & Hans, 2019). It is the benchmark major procedure, the one most studied and most often performed, particularly in larger and more active patients.
The reason comes down to load. The bone-reshaping osteotomies, of which TPLO is the most common, tend to be favoured over the less invasive lateral suture in bigger, heavier, more active dogs, because they restore limb function more reliably under the higher forces those dogs put through the joint (Bergh et al., 2014). Working dogs, athletic dogs and agility dogs are the group most often expected to return close to their pre-injury function, which is why a surgeon will frequently steer a fit, powerful, active dog towards a TPLO (Nanda & Hans, 2019). Historically it was described mostly in medium and large breeds, but its outcomes have proved reliable enough that it is now offered across a much wider range of sizes, and giant-breed dogs in particular are often considered good candidates (Nanda & Hans, 2019).
It cuts the other way too, and this matters just as much. For a small, light, older or otherwise complicated dog, a major osteotomy is not automatically the answer, and well-run conservative management is real medicine rather than a consolation prize, a genuine option I would never dismiss for the right patient. If that sounds more like your dog, the conservative-management guide is the candid counterweight to this page.
I want to be careful here, though, because this is where useful information shades into overreach. I can describe the typical TPLO candidate, but I cannot tell you that TPLO is the right operation for your particular dog. That is a genuinely individualised judgement, made by a surgeon with hands on the joint and the X-rays in front of them, weighing your dog's size, age, conformation and the state of the knee. It is never mine to make from a page. If you want to understand how that choice gets made, and how TPLO stacks up against TTA and the lateral suture, the comparison guide is the place for it.
How well it works
In a controlled study using force-plate gait analysis, dogs treated with TPLO had limb function that was indistinguishable from a normal, sound dog population one year after surgery, and more symmetric loading than dogs treated with extracapsular (lateral suture) repair (Nelson et al., 2013). In a separate randomised, blinded, controlled trial, owners leaned the same way: 80% of TPLO owners gave a top satisfaction score against 68% in the lateral-suture group, though in truth the difference between the two did not reach statistical significance (Gordon-Evans et al., 2013). So the headline is not that TPLO beats every alternative for every dog. It is that a well-done TPLO followed by proper rehabilitation reliably returns most dogs to a leg they use normally. The objective gait data is exactly why that holds up rather than being wishful thinking.
A TPLO limits arthritis. It does not prevent it. Some degree of arthritis is already on its way the moment the knee becomes unstable, and radiographic osteoarthritis keeps progressing after stabilisation, with measurable progression on follow-up X-rays after TPLO that is significant by around twenty-four months (Hurley et al., 2007; Shimada et al., 2020). Stabilising the joint is still worth it, because the alternative, leaving the knee unstable, drives arthritis faster and keeps the dog in pain, but no operation rewinds the clock to an arthritis-free knee. If you want the full lifelong picture, the long-term arthritis guide covers it properly, and it is genuinely worth reading once the surgery is behind you. The short version is that a well-stabilised knee is a comfortable, functional knee for years, but it asks for the kind of lifelong weight and muscle care that keeps any arthritic joint happy.
What can go wrong
No major operation is risk-free, and you deserve real numbers rather than vague reassurance. The most useful come from a large single-surgeon series of 1,000 consecutive dogs (1,146 stifles), in which the overall complication rate was 14.8%, of which 6.6% were major, with postoperative infection occurring in 6.6% of cases (Fitzpatrick & Solano, 2010).
The fair way to read those figures is this: most dogs sail through. A minority have a complication, and of those, most are minor and treatable. The single most common major problem is a surgical-site infection, which sometimes settles around the implant and is usually managed with antibiotics, occasionally with implant removal once the bone has healed. Serious problems with the bone cut or the plate itself are uncommon. It is, in short, a well-understood operation with a largely manageable risk profile, which is part of why surgeons reach for it so readily.
One complication is worth singling out, because it explains a pattern that frightens owners when they do not expect it. At the time of surgery, a meniscal tear, damage to the cartilage cushion in the knee, is found and dealt with in a substantial share of cases: in that same series, a concurrent meniscal injury was present in 33.2% of stifles (Fitzpatrick & Solano, 2010). Separately, a late meniscal tear, one that happens weeks to months after an otherwise successful operation, occurred in 2.8% of cases (Fitzpatrick & Solano, 2010). That late tear is the classic reason a dog that was recovering beautifully suddenly comes up lame again. The meniscus itself, and the debate about how it is best managed, belongs to its own guide, so I will not expand it here. But the practical point matters: if your dog is doing well and then abruptly deteriorates, that is not something to wait out. Knowing the red flags protects your dog's recovery, and the recovery red-flags guide tells you what warrants a call.
A brief word on cost, since it is often the next question. UK TPLO pricing is a practical, real-world estimate rather than anything from a peer-reviewed source, and the detail, along with how insurance tends to handle it, lives in the cost guide.
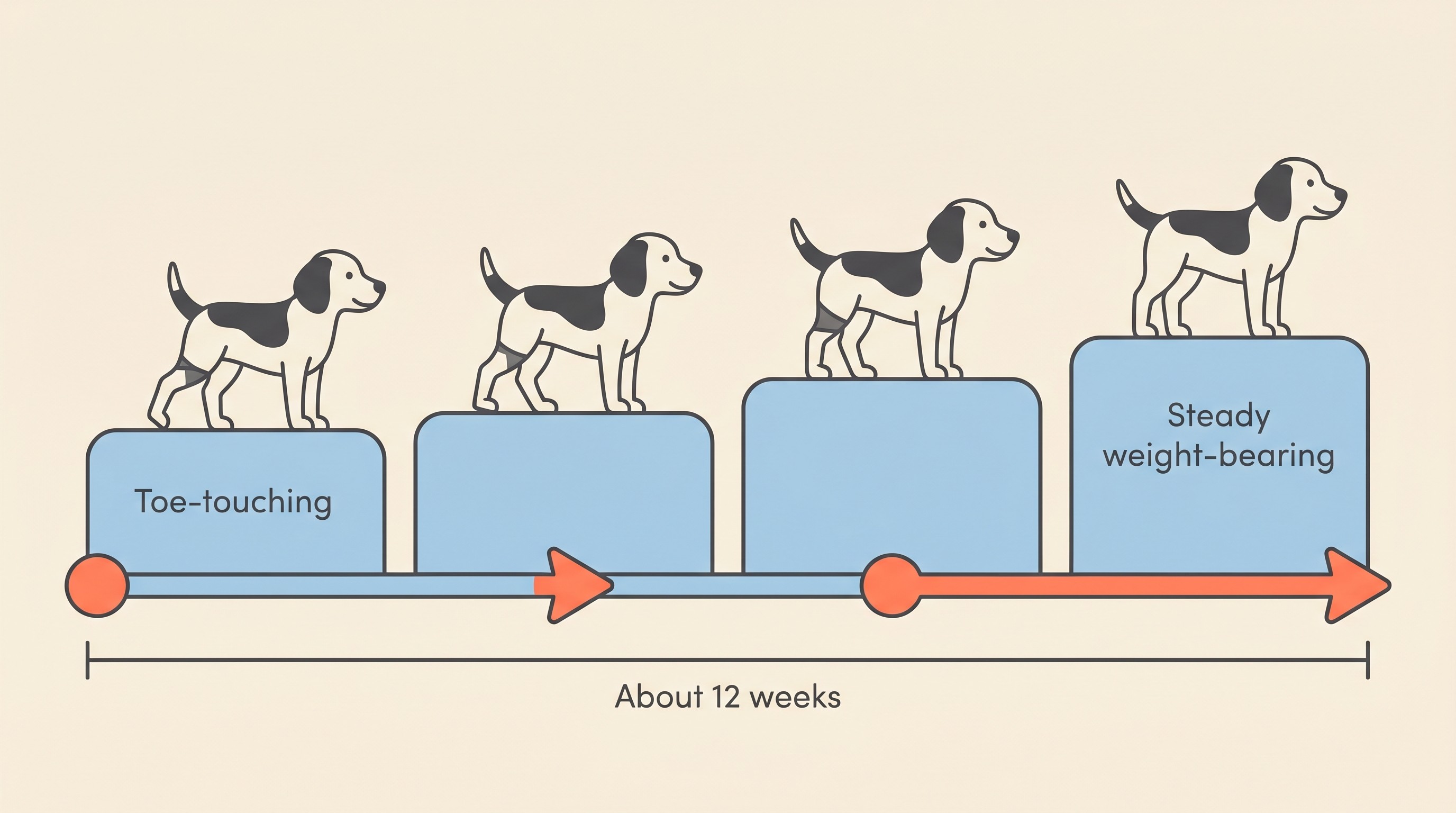
A last reassurance, and a handover. Recovery from a TPLO is measured the sensible way, by how your dog uses the leg: weight-bearing, lameness and swelling, tracked against the expected post-operative week. Bone healing is the rate-limiting step, which is precisely why strict rest matters so much in the early weeks, and the canonical arc is around twelve weeks from theatre to a dog back to normal function. I am deliberately not writing the recovery plan here, because the recovery guides own it and do it far better than a paragraph could. From the day your dog comes home, the twelve-week recovery roadmap and the Recovery Tracker pick the journey up, week by week, so you always know whether what you are seeing is on track.
A TPLO is, in the end, one of the best-understood operations in small-animal orthopaedics, with outcomes that are genuinely and reliably good for the right dog. If you are signing the consent form tonight with a knot in your stomach, that is entirely normal, and I hope this has untangled at least some of it.
References
- Bergh MS, Sullivan C, Ferrell CL, Troy J, Budsberg SC, 2014. Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. Journal of the American Animal Hospital Association 50(5):315-321. doi:10.5326/JAAHA-MS-6356.
- Boudrieau RJ, 2009. Tibial plateau leveling osteotomy or tibial tuberosity advancement? Veterinary Surgery 38(1):1-22. doi:10.1111/j.1532-950X.2008.00439.x.
- Fitzpatrick N, Solano MA, 2010. Predictive variables for complications after TPLO with stifle inspection by arthrotomy in 1000 consecutive dogs. Veterinary Surgery 39(4):460-474. doi:10.1111/j.1532-950X.2010.00663.x.
- Gordon-Evans WJ, Griffon DJ, Bubb C, Knap KM, Sullivan M, Evans RB, 2013. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs with cranial cruciate ligament disease. Journal of the American Veterinary Medical Association 243(5):675-680. doi:10.2460/javma.243.5.675.
- Hurley CR, Hammer DL, Shott S, 2007. Progression of radiographic evidence of osteoarthritis following tibial plateau leveling osteotomy in dogs with cranial cruciate ligament rupture: 295 cases (2001-2005). Journal of the American Veterinary Medical Association 230(11):1674-1679. doi:10.2460/javma.230.11.1674.
- Kim SE, Pozzi A, Kowaleski MP, Lewis DD, 2008. Tibial osteotomies for cranial cruciate ligament insufficiency in dogs. Veterinary Surgery 37(2):111-125. doi:10.1111/j.1532-950X.2007.00361.x.
- Nanda A, Hans EC, 2019. Tibial plateau leveling osteotomy for cranial cruciate ligament rupture in canines: patient selection and reported outcomes. Veterinary Medicine: Research and Reports 10:249-255. doi:10.2147/VMRR.S204321.
- Nelson SA, Krotscheck U, Rawlinson J, Todhunter RJ, Zhang Z, Mohammed H, 2013. Long-term functional outcome of tibial plateau leveling osteotomy versus extracapsular repair in a heterogeneous population of dogs. Veterinary Surgery 42(1):38-50. doi:10.1111/j.1532-950X.2012.01052.x.
- Shimada M, Mizokami N, Ichinohe T, Kanno N, Suzuki S, Yogo T, Harada Y, Hara Y, 2020. Long-term outcome and progression of osteoarthritis in uncomplicated cases of cranial cruciate ligament rupture treated by tibial plateau leveling osteotomy in dogs. Journal of Veterinary Medical Science 82(7):908-916. doi:10.1292/jvms.19-0613.
- Slocum B, Slocum TD, 1993. Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Veterinary Clinics of North America: Small Animal Practice 23(4):777-795. doi:10.1016/s0195-5616(93)50082-7.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine