TTA and the Other Osteotomies
Dr. Alastair Greenway
MRCVS
The letters on your consent form say TTA, or MMP, or CBLO, and somewhere along the way the internet told you everyone does the TPLO. So a familiar worry arrives: a surgeon you trust has recommended a different set of initials, and it's hard not to read that as your dog getting the lesser version. That worry is one of the most common ones owners bring me at this stage.
It rests on a misunderstanding, and I'd rather unpick it now than have you carry it into surgery week. The TPLO isn't the only bone-cutting way to stabilise a cruciate-deficient knee, and the alternatives aren't consolation prizes. They're different routes to exactly the same destination, and a good surgeon picks between them for real reasons to do with your dog's knee, not with what's fashionable.
A quick scoping note before we start. This article assumes the decision to operate has already been made. If you're still weighing surgery against conservative care, that belongs to the decision guide. I'm also not going to re-teach the TPLO, which has its own guide, nor crown a winner, which is the job of the comparison piece. My aim is narrower: to explain the tibial tuberosity advancement and its relatives clearly enough that, when your surgeon tells you why they've chosen one for your dog, you can follow the reasoning and ask a good question back.
TTA: the same goal, a different geometry
Every one of these operations is trying to do the same thing. When the cruciate fails, the shin bone (the tibia) is free to slide forward under the thigh bone every time your dog bears weight, and that abnormal forward shear is what hurts and drives the arthritis. The cruciate isn't coming back, so rather than repair a ligament, all the osteotomies re-shape the bone until the joint stops needing one (RCVS Knowledge Canine Cruciate Registry, 2024). The TPLO does this by levelling the backward slope at the top of the tibia. The TTA, the tibial tuberosity advancement, gets there by completely different geometry, and that's the part worth understanding.
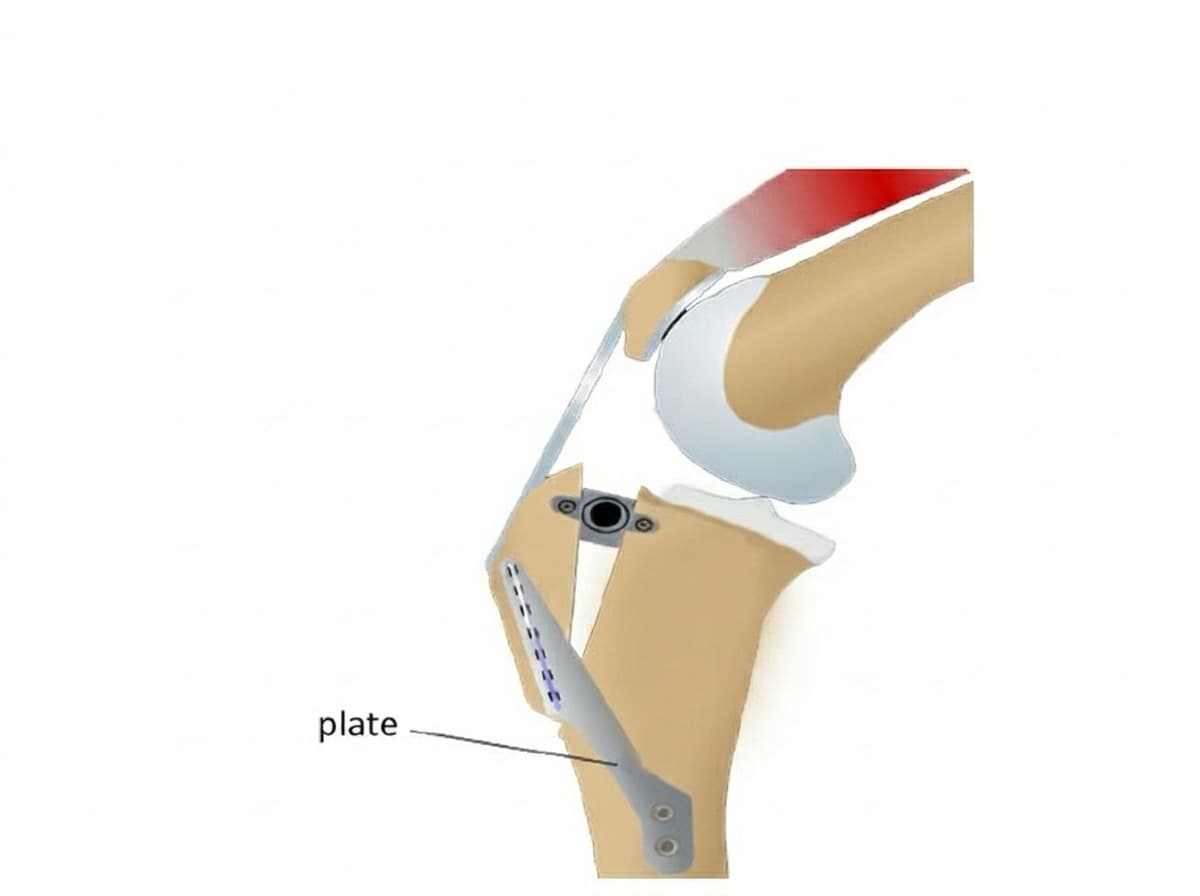
The big thigh muscle, the quadriceps, pulls on the shin through the patellar tendon, the band you can feel just below your dog's kneecap. In a normal knee, the direction of that pull and the slope of the joint mean the shin is always being nudged slightly forward, and the cruciate is what holds it. The insight behind the TTA, first described by Montavon and Tepic around 2002, is that moving the bony bump where that tendon attaches (the tibial tuberosity) forward changes the angle of the pull. Advance it far enough that the tendon sits at roughly 90 degrees to the top of the tibia, and the forward shear the cruciate used to resist effectively cancels out, so the quadriceps pull holds the joint stable and the ligament is genuinely no longer needed (Wemmers et al., 2022; RCVS Knowledge Canine Cruciate Registry, 2024).
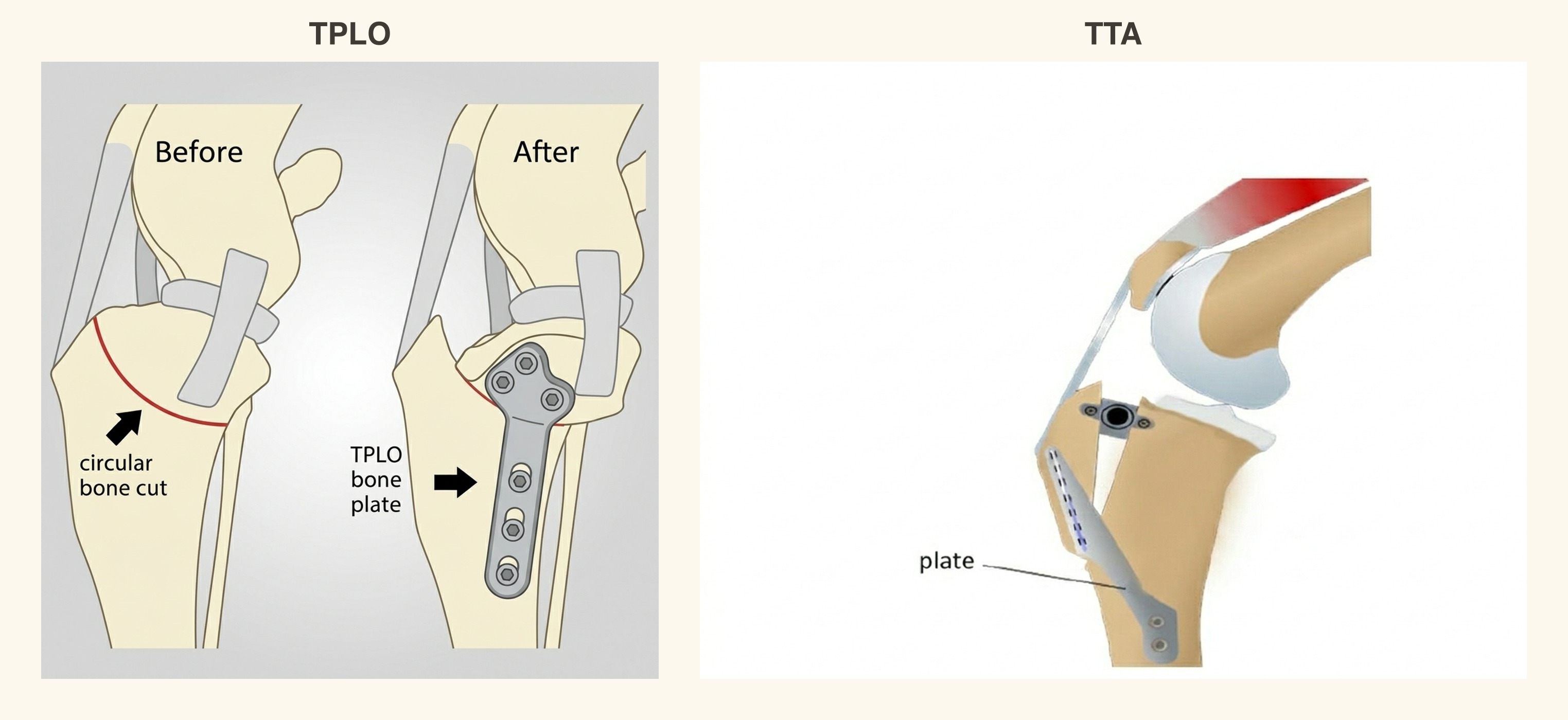
In practice the surgeon cuts to free the front edge of the tibia, advances the tuberosity, and holds it in place with a plate; in the classic TTA, a small titanium cage spacer keeps the advancement open while the bone heals (RCVS Knowledge Canine Cruciate Registry, 2024). As with the TPLO, that metalwork is designed to stay in for life.
Does it work? Yes, and the "lesser operation" worry needs that answer plainly. Across the whole tibial-tuberosity-advancement family, roughly 90 to 95% of dogs return to full or acceptable use of the leg over short, medium and long-term follow-up (Aragosa et al., 2022). The UK cruciate registry, which gathers real-world outcomes from British surgeons, puts good-to-excellent results at around 90% of dogs, with about 97.8% of owners saying they'd choose it again (RCVS Knowledge Canine Cruciate Registry, 2024). Those are not the numbers of a second-rate operation.
No surgery is without cost, and I'd rather you heard the complication picture from me than from a forum at midnight. Across the TTA-family techniques, minor complications run at around a third of cases and major ones, the kind that need a return to theatre, at roughly 10.7%, with a fissure or fracture through the tibial crest the commonest minor problem and a small later risk (around 4.3%) of a meniscal tear, a story of its own told in the meniscus guide (Aragosa et al., 2022). Most are manageable and most dogs never meet any of them, but you're entitled to know the real denominator.
The other osteotomies: MMP and CBLO
If your surgeon used a slightly different name, two relatives are worth knowing about, because in the UK you may well be offered one of them under the broad "TTA" umbrella.
The first is the Modified Maquet Procedure, or MMP, a close cousin of the TTA that's common in British practice. It advances the very same tibial tuberosity on the very same principle, but instead of a cage spacer it holds the advancement open with a wedge of porous titanium foam, placed through a smaller, quicker cut into which the dog's own bone then grows (RCVS Knowledge Canine Cruciate Registry, 2024). If you were told you were having a "TTA" but the paperwork says MMP, that's why.
The second is the CORA-Based Levelling Osteotomy, or CBLO, developed by Don Hulse at Texas A&M. This one is actually a relative of the TPLO rather than the TTA: it levels the tibial plateau too, but places the cut further from the joint, at a point in the bone's natural alignment surgeons call the CORA. That makes it especially useful in two situations a standard TPLO finds awkward: skeletally immature dogs whose growth plates are still open, and dogs with a very steep tibial plateau angle (RCVS Knowledge Canine Cruciate Registry, 2024). Its outcomes sit in the same good company: owner-reported good-to-near-complete function in around 90 to 95% of dogs, and about 93% owner satisfaction at twelve months (RCVS Knowledge Canine Cruciate Registry, 2024). It's offered by fewer surgeons and tends to cost more, and the real-world UK figures live in the cost guide.
TPLO versus TTA, fairly
So if the TTA works this well, why does the TPLO get all the airtime, and which is actually better? Here's the honest answer, and it isn't a dodge: on the current evidence, neither is proven superior overall.
The most careful synthesis we have is a systematic review with meta-analysis that pooled the TPLO and TTA studies and looked for a winner. It didn't find a clear one. Both came out as successful options and their overall complication rates were close together, around 20 to 22% either way, so the authors made no overall recommendation either way, noting that almost half the underlying studies were of low quality (Wemmers et al., 2022). The one caveat is that the same review found the TPLO came out slightly ahead on a few specific complications, such as surgical site infection (Wemmers et al., 2022). That echoes the wider review across every cruciate procedure, which likewise found it unclear whether any single technique is superior (Bergh et al., 2014). When two careful, independent reviews both decline to crown an overall winner, that isn't fence-sitting. That's the finding.
There's one real nuance, because good medicine includes the bits that don't fit neatly. In the one prospective study that put force plates under dogs and compared the procedures directly, the TPLO limbs returned to control-level function at both the walk and the faster trot by six to twelve months. The TTA limbs reached normal at the walk, but at the trot they stayed statistically indistinguishable from lateral-suture repair, so they hadn't quite normalised at the faster gait by the study's end (Krotscheck et al., 2016). Two things keep that in proportion: the numbers were small (14 dogs with a TTA, 15 with a TPLO), and a difference on a force plate at a trot isn't the same as one your dog's life will notice. It's a reason to weigh the choice carefully, not to call the TTA a failure.
So what does the choice rest on? On your dog, and on your surgeon. The relevant factors are your dog's tibial anatomy, such as the plateau angle and the shape of the bone, its size and activity level, the surgeon's own experience and audited results with each technique, and cost (Wemmers et al., 2022; Bergh et al., 2014). A steep plateau or an immature skeleton might tilt things toward a CBLO, and the UK registry notes that in very large dogs, over about 50 kg, the TTA may carry a higher revision rate than some alternatives, exactly the sort of individual factor a surgeon weighs (RCVS Knowledge Canine Cruciate Registry, 2024). The full side-by-side of how surgeons balance all this lives in the comparison guide, the right next read if you're still turning the choice over.
One note to hold lightly: whichever cut your dog has, it stabilises the knee, it doesn't repair the ligament, and it doesn't abolish arthritis. Cruciate disease is a degeneration, and some stifle arthritis is inevitable once the joint has been unstable. A good osteotomy slows that, but it doesn't undo it (Wemmers et al., 2022). And because the tendency often sits in the dog rather than in bad luck, there's a real chance the other knee will follow in time, which the other-leg guide treats fully (Muir et al., 2011).
What to ask, and where this goes next
If your surgeon has recommended a TTA, an MMP or a CBLO, the useful question isn't "is this the best operation in the world." It's "why is this the right cut for my dog's knee," and a good surgeon will answer it gladly, in terms of your dog's tibial anatomy, size and activity, and their own results. If the answer is just "it's what we do," it's entirely fair to ask for more, and a specialist opinion is exactly where that detail lives.
With that answer and a date in the diary, the question shifts from which operation to what happens next. Whichever osteotomy your dog has, recovery runs to around twelve weeks, with strict rest of roughly eight weeks and an X-ray check at that point before you ease off (RCVS Knowledge Canine Cruciate Registry, 2024). You'll track it not by any grade but by the simple things you can see, week by week against the post-op clock: how much weight the leg is taking, how the lameness is settling, whether the swelling is going down. The 12-week recovery roadmap walks you through each of those weeks, and our recovery tracker gives you somewhere to log it so you and your vet see the line of progress rather than guess at it. That part is genuinely in your hands, and it matters more to the result than which cut your surgeon picked.
References
- Aragosa, F., Caterino, C., Della Valle, G., & Fatone, G. (2022). Tibial Tuberosity Advancement Techniques (TTAT): A Systematic Review. Animals, 12(16), 2114.
- Bergh, M. S., Sullivan, C., Ferrell, C. L., Troy, J., & Budsberg, S. C. (2014). Systematic Review of Surgical Treatments for Cranial Cruciate Ligament Disease in Dogs. Journal of the American Animal Hospital Association, 50(5), 315-321.
- Krotscheck, U., Nelson, S. A., Todhunter, R. J., Stone, M., & Zhang, Z. (2016). Long Term Functional Outcome of Tibial Tuberosity Advancement vs. Tibial Plateau Leveling Osteotomy and Extracapsular Repair in a Heterogeneous Population of Dogs. Veterinary Surgery, 45(2), 261-268.
- Muir, P., Schwartz, Z., Malek, S., Kreines, A., Cabrera, S. Y., Buote, N. J., et al. (2011). Contralateral Cruciate Survival in Dogs with Unilateral Non-Contact Cranial Cruciate Ligament Rupture. PLOS ONE, 6(10), e25331.
- RCVS Knowledge Canine Cruciate Registry. (2024). Common surgical procedures: Tibial Tuberosity Advancement (TTA) and Modified Maquet Procedure (MMP). RCVS Knowledge.
- RCVS Knowledge Canine Cruciate Registry. (2024). Common surgical procedures: CORA-Based Levelling Osteotomy (CBLO). RCVS Knowledge.
- Wemmers, A. C., Charalambous, M., Harms, O., & Volk, H. A. (2022). Surgical treatment of cranial cruciate ligament disease in dogs using Tibial Plateau Leveling Osteotomy or Tibial Tuberosity Advancement: a systematic review with a meta-analytic approach. Frontiers in Veterinary Science, 9, 1004637.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine