Lateral Suture: The Less Invasive Option
Claire Greenway
BVM&S MRCVS
A lateral suture is the cruciate operation that doesn't cut your dog's shin bone, and that fact tends to pull owners two ways at once. There's relief that a saw isn't part of the plan, and there's a nagging suspicion that the gentler-sounding option must be the second-rate one. Neither reading holds up. The lateral suture isn't a poor relation of the bone-cutting operations, and it isn't a magic cheap fix either. It's a real, well-established procedure that suits one kind of dog very well and another kind rather poorly.
This piece assumes you've decided surgery is the right road. If you haven't settled that, start with the surgery-or-not decision guide, and if you want this option set head-to-head against the osteotomies, that even-handed comparison lives in TPLO vs TTA vs Lateral Suture. Below, I'll go deep on the lateral suture itself: how it works, who it's genuinely for, and what the outcomes really look like once you read past the marketing.
How it works
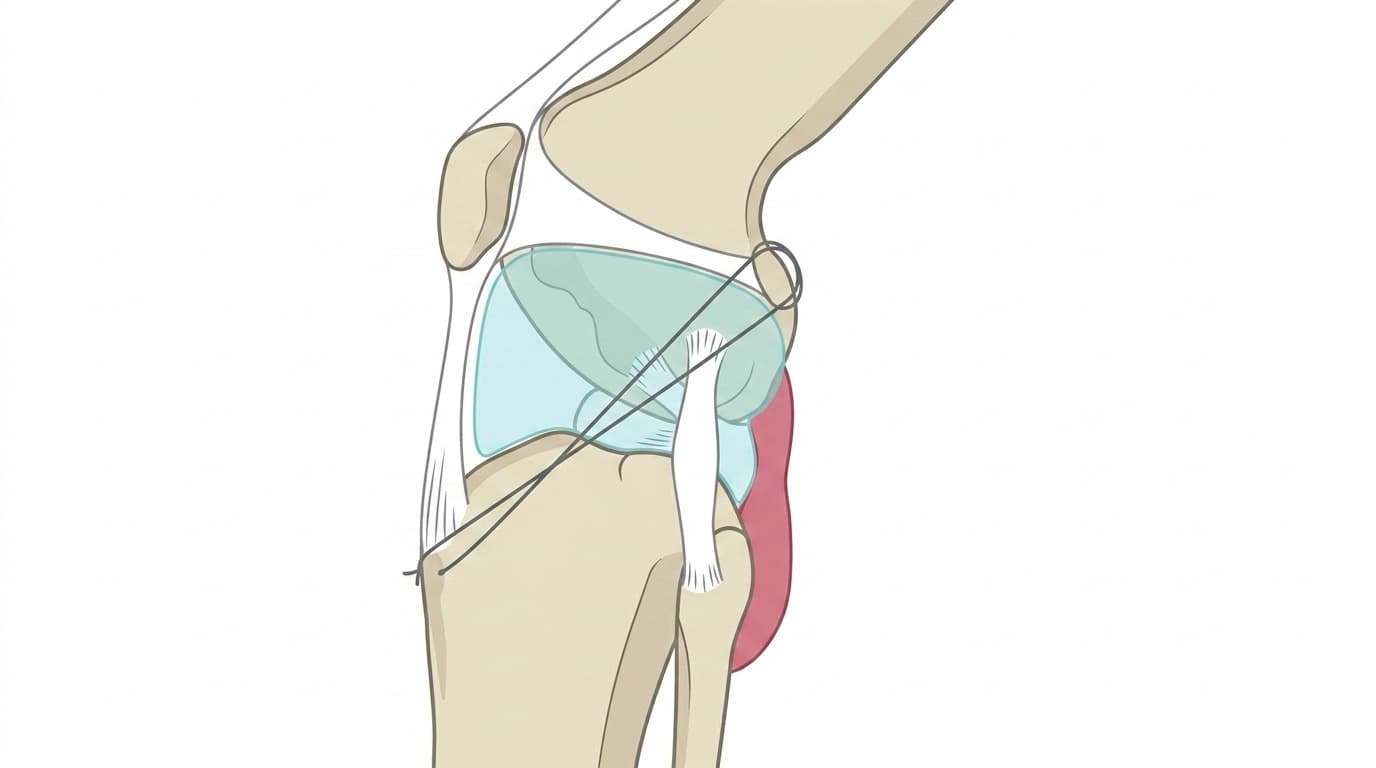
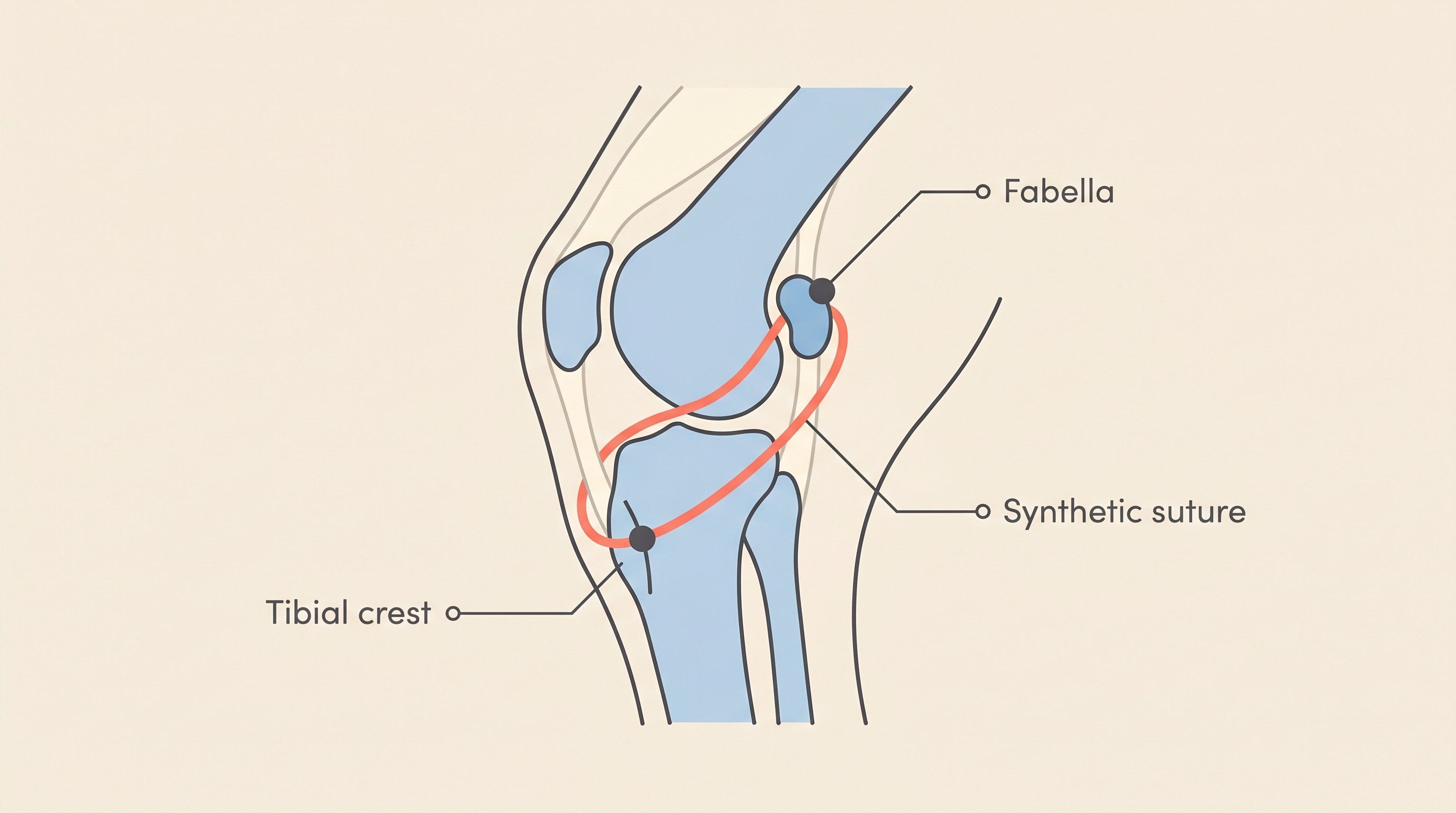
The first thing to understand is that the lateral suture sits outside the joint. You'll see it written as the lateral fabellar suture, or extracapsular lateral suture stabilisation (often shortened to ELSS), and sometimes as a branded system such as TightRope. The word tying all those names together is extracapsular, meaning outside the joint capsule, and it's the term likely to appear on your quote (RCVS Knowledge Canine Cruciate Registry, n.d.).
The mechanism is straightforward once you picture it. A strong synthetic suture is anchored around a small bone behind the knee called the lateral fabella, then passed through or near the front of the shin bone, so it runs roughly along the line the cruciate used to take. When your dog bears weight, that suture stops the shin bone sliding forward against the thigh bone, the abnormal movement that makes a cruciate-deficient knee unstable and sore (RCVS Knowledge Canine Cruciate Registry, n.d.). It doesn't repair or replace the torn ligament. It works from the outside to do the ligament's old job of holding the joint steady.
There's one point a lot of pages skip, and it matters more than any other: the suture is not meant to hold the knee together forever. It's an internal splint that buys time. Over the weeks and months after surgery, the body lays down its own scar tissue, periarticular fibrosis, around the joint, and that thickened tissue takes over the long-term job of stabilising the knee. As the fibrosis builds and assumes the load, the suture itself gradually stretches, loosens or breaks, and by then it has usually done its work (RCVS Knowledge Canine Cruciate Registry, n.d.). The suture buys the time; the scar tissue is what lasts.
That difference is the whole reason this procedure is described as less invasive. A TPLO or a TTA re-engineers the geometry of the shin bone so the knee is stable without any ligament at all. The lateral suture leaves your dog's own anatomy untouched: no bone cut, no plate, and, above all, no bone that has to heal. It leans on an implant plus scar tissue rather than on reshaping the skeleton, and exactly how the osteotomies do that reshaping I'll hand to TPLO Explained and TTA and the Other Osteotomies.
One truth I'll carry in from the rest of this space: stabilising the knee, by any method, treats the instability but not the underlying disease. Canine cruciate disease is a slow degeneration of the ligament, not a rope that snapped in one unlucky leap, and no suture reverses that or undoes the arthritis an unstable joint has already begun. Stabilising slows that arthritis; it doesn't prevent it. (If the degenerative picture is new to you, Why It's Degeneration, Not an Injury is the piece for it.)
Who it suits
This is where the lateral suture earns its place. The procedure is more commonly advised in smaller and less active dogs (RCVS Knowledge Canine Cruciate Registry, n.d.). A small, light dog asks far less of its knee with every step, so the forces are lower, the suture and scar tissue have a more manageable job, and the result tends to hold up well.
In day-to-day UK practice you'll often hear an informal weight guide, something like extracapsular repair being favoured around and below roughly fifteen kilograms, with the osteotomies preferred above that in larger, younger, more athletic dogs. I want to be careful with that number: it's a practical clinical pattern, not a peer-reviewed cut-off, and a good surgeon weighs the whole dog rather than the reading on the scales. Treat the weight band as a guide to the conversation, not a verdict.
There's a second group the lateral suture genuinely serves: dogs for whom an osteotomy isn't suitable or isn't affordable. Some carry other health problems that make a longer anaesthetic and a bone-healing recovery a poorer bet, some have anatomy that complicates the osteotomy options, and for some families the cost of a specialist procedure simply isn't reachable. An operation that gives a real, good result at lower cost is, for those dogs, the sensible and kind choice, not a compromise to apologise for.
One boundary worth drawing, though: if your dog isn't a surgical candidate at all, the lateral suture isn't a halfway house between surgery and no surgery. It's still surgery. The genuinely non-surgical route, with its own real merits for the right dog, is Conservative Management.
Whatever you choose, plan for one more thing: the other knee. Because this is a bilateral-tendency degeneration rather than bad luck in a single joint, the contralateral cruciate is at real risk. One study following dogs after a first rupture found 54% went on to rupture the other-leg cruciate over the follow-up period (Muir et al., 2011). That's a budgeting and planning fact rather than a reason to panic, and the full picture sits in Will the Other Leg Go Too?.
Outcomes and limits
Here is the full picture, because this is exactly where competitor pages tend to go soft in one direction or the other. In the right patient, a smaller or less active dog, the lateral suture gives genuinely good function. UK registry figures describe around 85% of dogs regaining complete or near-complete function, and roughly 82% of owners rating their dog's function good or excellent (RCVS Knowledge Canine Cruciate Registry, n.d.). Those are aggregate registry numbers rather than a single trial, but they reflect a great many real dogs walking comfortably again.
The qualification is that the comparative evidence consistently favours the osteotomies, the TPLO in particular, for returning a dog to fuller, faster, more athletic function. A broad systematic review concluded the evidence most strongly supports TPLO for return to normal function, and gave strong support to intermediate-period recovery being superior after TPLO compared with the lateral extracapsular suture, with too few data to judge TTA fully (Bergh et al., 2014). A force-plate study sharpened where that gap lives: by six to twelve months, TPLO dogs had returned to control-level function at both walk and trot, whereas the extracapsular repair did not normalise at the trot, and TTA normalised at the walk but at the trot was indistinguishable from the extracapsular repair (Krotscheck et al., 2016). The gap shows up most at higher demand, which is exactly why a surgeon steers a big, young athlete towards a bone-cutting procedure.
The ceiling is worth holding plainly in both directions, though. In a force-plate study of Labradors, the lateral suture and TPLO produced similar results and both bettered the older intracapsular techniques, yet all the groups only infrequently achieved truly normal function on objective measurement, especially where the meniscus had been involved (Conzemius et al., 2005). And further out, a long-term study found no significant force-plate difference between the osteotomy and extracapsular techniques, with roughly a third of dogs still carrying measurable lameness whatever the surgery they'd had (Molsa et al., 2014). In the long run the techniques converge more than the marketing suggests.
Now the limits specific to this procedure. It's less favoured for large, active dogs because the suture can loosen or fail before the scar tissue is strong enough to take over, letting instability creep back, and lameness can recur years later as arthritis advances. The complication rate is real but modest: a series of 363 cases found an overall rate of 17.4%, with 7.2% of dogs needing a second surgery, and, tellingly, greater body weight and younger age were both significantly associated with more complications (Casale & McCarthy, 2009). Those are exactly the big, young dogs a surgeon would tend to send towards an osteotomy anyway. The recognised problems are wound infection, suture-related issues such as the anchor loosening, and a late meniscal injury: a previously intact cartilage cushion tearing some time after the knee was stabilised. The meniscus is its own subject, so I'll hand that detail to The Meniscus.
Two practical points to close. On cost, the lateral suture is typically the least expensive of the three, needing no specialist saw, jig or bone plate and often no board-certified surgeon. As a UK practical estimate, not a peer-reviewed figure, many practices price it from a few hundred to around fifteen hundred pounds, comfortably below a typical specialist TPLO. The full breakdown, and how insurance handles it, lives in What Cruciate Surgery Costs in the UK.
On recovery, don't let the absence of a bone cut fool anyone into thinking your dog can run around sooner. The canonical arc is still around twelve weeks, the first six to eight weeks strict confinement and lead-only, because the scar tissue you're quietly growing needs that protected time to mature just as much as a healing bone would (RCVS Knowledge Canine Cruciate Registry, n.d.). We judge progress by weight-bearing, lameness and swelling against the expected post-operative week, not by any neurological grade. The week-by-week belongs to The 12-Week Recovery Roadmap, and the Recovery Tracker logs exactly those signs.
For a smaller, lighter or less active dog, the lateral suture can give an excellent, comfortable result at a price more families can manage, and there's nothing second-rate about choosing it. For a big, young athlete, your surgeon will very likely steer you towards an osteotomy instead, and the comparison guide explains exactly why. Either way, the right operation is the one a surgeon with hands on your dog's knee recommends, and walking in already understanding this option is how you make that a genuine, two-way conversation.
References
- Bergh MS, Sullivan C, Ferrell CL, Troy J, Budsberg SC, 2014. Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. Journal of the American Animal Hospital Association 50(5):315-321. doi:10.5326/JAAHA-MS-6356.
- Casale SA, McCarthy RJ, 2009. Complications associated with lateral fabellotibial suture surgery for cranial cruciate ligament injury in dogs: 363 cases (1997-2005). Journal of the American Veterinary Medical Association 234(2):229-235.
- Conzemius MG, Evans RB, Besancon MF, Gordon WJ, Horstman CL, Hoefle WD, Nieves MA, Wagner SD, 2005. Effect of surgical technique on limb function after surgery for rupture of the cranial cruciate ligament in dogs. Journal of the American Veterinary Medical Association 226(2):232-236.
- Krotscheck U, Nelson SA, Todhunter RJ, Stone M, Zhang Z, 2016. Long term functional outcome of tibial tuberosity advancement vs. tibial plateau leveling osteotomy and extracapsular repair in a heterogeneous population of dogs. Veterinary Surgery 45(2):261-268. doi:10.1111/vsu.12445.
- Molsa SH, Hyytiainen HK, Hielm-Bjorkman AK, Laitinen-Vapaavuori OM, 2014. Long-term functional outcome after surgical repair of cranial cruciate ligament disease in dogs. BMC Veterinary Research 10:266. doi:10.1186/s12917-014-0266-8.
- Muir P, Schwartz Z, Malek S, Kreines A, Cabrera SY, Buote NJ, Bleedorn JA, Schaefer SL, Holzman G, Hao Z, 2011. Contralateral cruciate survival in dogs with unilateral non-contact cranial cruciate ligament rupture. PLoS ONE 6(10):e25331. doi:10.1371/journal.pone.0025331.
- RCVS Knowledge Canine Cruciate Registry, n.d. Extracapsular lateral suture stabilisation (ELSS) [dog-owner information]. Available at:
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine