Getting the diagnosis: why chronic enteropathy is what is left when everything else is ruled out
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
If you have already read about what chronic enteropathy is, you will know it is not one tidy disease but a group of long-running gut problems that we sort out mostly by how they respond to treatment. What that explainer does not answer is the question almost every worried owner asks next: if you think it might be this, why not just scope him and tell me for sure?
It is a fair question. There is no single blood test that says "chronic enteropathy", because the gut produces the same handful of signs for a long list of causes. CE is, and remains, a diagnosis of exclusion: what is left once we have ruled out the other things that produce the same picture (Heilmann et al., 2026). Your vet reaches it not with one clever test but by working through the alternatives in order. That is not a fobbing-off; it is the careful thing, and it usually pays off long before anyone reaches for a scope. (The formal term in the 2026 guidelines is "chronic inflammatory enteropathy", but I will use "chronic enteropathy", CE, throughout.)
Before any of this begins, the problem has to qualify as chronic in the first place. The working threshold most vets use is signs that persist or keep returning for roughly three weeks or more: vomiting, diarrhoea, weight loss, a changeable appetite, a coat that has lost its shine (Dandrieux, 2016; Heilmann et al., 2026). Whether a given upset is a passing bug to watch at home or a chronic problem to investigate belongs to vomiting and diarrhoea explained. The idea to carry across is that diarrhoea is a symptom, not a diagnosis, which is precisely why we rule the causes out one by one.
How the work-up is ordered, and the reason for it
Picture the work-up as a staircase. We start at the bottom, where the tests are cheap and pick up the commonest culprits, and only climb higher if the lower steps come back clear.
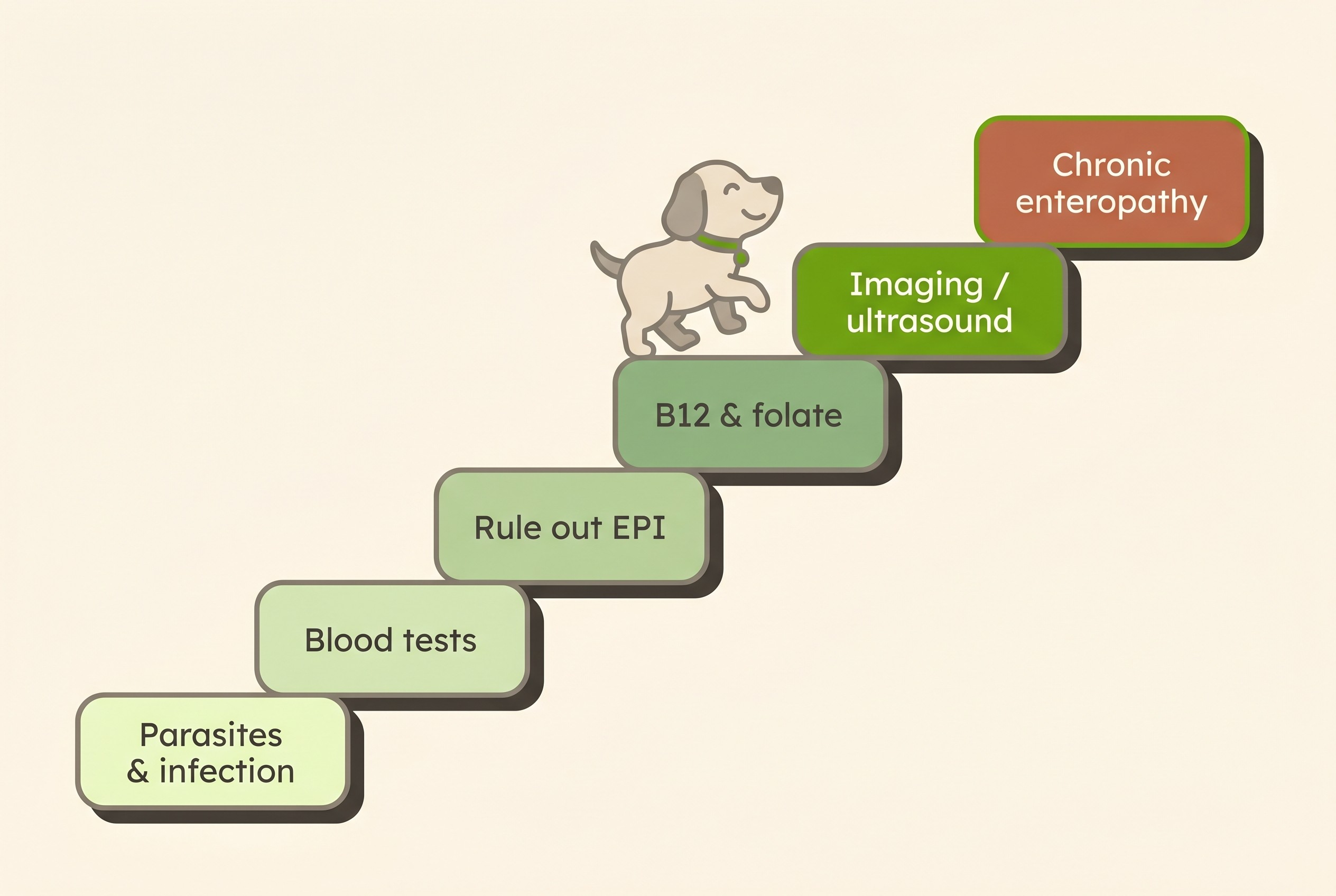
First, the cheap and common things: parasites and infection. Faecal testing, including a Giardia antigen test, comes early, because intestinal parasites are common, treatable, and can produce exactly the chronic-diarrhoea picture you are worried about (Heilmann et al., 2026). It would be poor medicine to investigate a complicated immune condition before checking for a worm or protozoan that a simple course of treatment would clear. Which parasites do this is covered in worms, giardia and chronic diarrhoea.
Then blood tests, to look for disease outside the gut and find the fixable things. A complete blood count and a biochemistry panel with electrolytes are not looking for CE itself. They look for whole-body or organ diseases that show up as gut signs, such as kidney disease, and for clues to hypoadrenocorticism (Addison's disease), a hormonal condition that is a notorious mimic of chronic gut disease and that the consensus specifically recommends excluding, using a resting cortisol and, if low, an ACTH stimulation test (Heilmann et al., 2026). Other systemic causes with marked thirst or weight loss, such as diabetes or an overactive thyroid, are screened for too, though those belong to the endocrine and hormones space.
EPI is ruled out with a specific test, not assumed away. Exocrine pancreatic insufficiency, where the pancreas stops making enough digestive enzymes, causes loose, greasy, voluminous faeces and weight loss in a hungry dog, which overlaps heavily with CE. It is excluded with a single fasted serum trypsin-like immunoreactivity (TLI) test, essentially a blood test for the enzyme-making part of the pancreas, which is highly sensitive and specific for EPI (Williams & Batt, 1983; Williams & Batt, 1988). The fasted part matters: a recent meal can nudge the result up into the normal range and hide the problem. A pancreatic-specific lipase usually runs alongside it to assess for pancreatitis, and the EPI story itself is told in EPI explained.
Cobalamin and folate, for two good reasons. Cobalamin is simply vitamin B12, and low levels are strikingly common in CE: the consensus reports hypocobalaminaemia in roughly 19 to 61% of affected dogs and notes it is a negative prognostic factor, meaning low B12 tends to go with a tougher course (Heilmann et al., 2026). That echoes older landmark work, in which a cobalamin below 200 ng/L predicted a worse outcome (Allenspach et al., 2007). Folate adds information about a different part of the small intestine, though it is a weaker marker (Heilmann et al., 2026). We measure both because they help localise the problem and because a low B12 is fixable: correcting it can itself improve how a pet responds to treatment. Topping up B12 (oral versus injection, and dose) lives in living with chronic enteropathy. A normal cobalamin, incidentally, does not rule CE out (Heilmann et al., 2026).
Imaging where it is needed, usually an ultrasound. Abdominal ultrasonography is recommended before any thought of a scope, not to confirm CE but to find the things that masquerade as it: a mass, a blockage, a strikingly thickened patch of bowel, enlarged lymph nodes, or the wall and fluid changes that point to gut protein loss (Heilmann et al., 2026). It maps the problem and rules out the mimics. (Where a blockage is the worry, that is urgent territory: see digestive emergencies.)
Where the diet trial fits: a test as much as a treatment
This is the step that surprises people most, and it is the heart of why a biopsy is rarely step one. A properly run diet trial is not a delaying tactic before the "real" tests; it is one of the most important diagnostic steps there is. The 2026 consensus is emphatic that, in clinically stable dogs, dietary treatment trials are the preferred first-choice diagnostic recommendation, used before invasive tests (Heilmann et al., 2026). The logic is simple: the largest group of dogs with CE turn out to be food-responsive, so when a pet responds to the right diet, the response itself has made the diagnosis. You have identified the type of CE and treated it in one move, without an anaesthetic.
The mechanics, which diet, how strict and how long, have their own guide in the diet trial, done properly. What matters here is that the diet trial comes before biopsy precisely because it is a test, and if your vet recommends one, the Diet-Trial Companion helps you run it strictly and read the result rather than guessing.
A biopsy: what it can settle, and what it can't
This is where a lot of online advice quietly misleads. A biopsy, taken through an endoscope or at surgery, is genuinely useful for certain questions. It can confirm whether there is inflammation and how severe it is, classify the type (for example lymphoplasmacytic versus eosinophilic), and pick up structural problems such as lymphangiectasia, where the gut's lymph channels are abnormal. Samples are graded against standardised WSAVA criteria, so different pathologists at least describe the same features (Day et al., 2008). In cats especially, a biopsy with clonality testing is often what separates chronic inflammation from a low-grade lymphoma, which matters because the two look so alike (Marsilio et al., 2023).
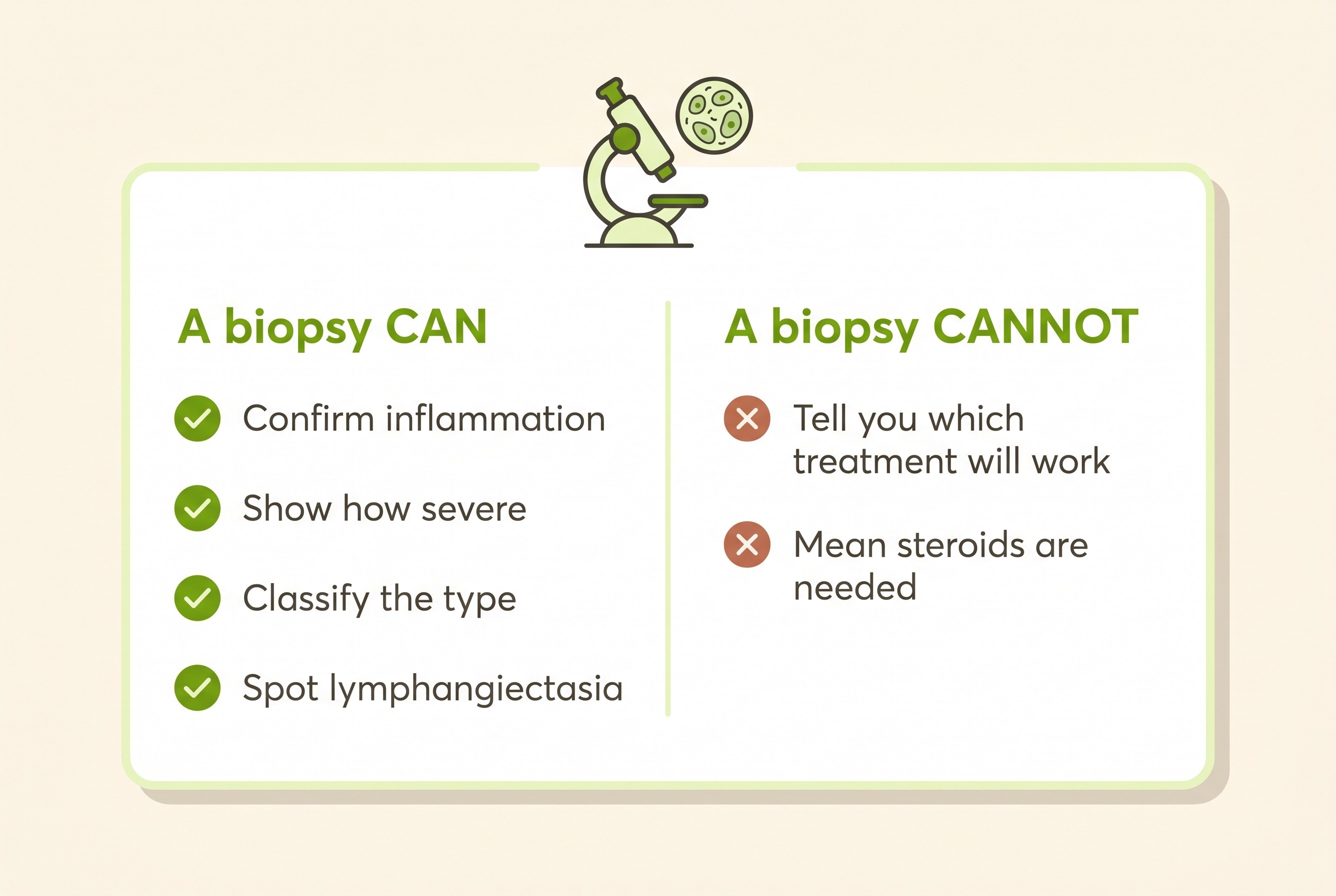
But a biopsy does not tell you which treatment will work, and it does not, by itself, mean steroids are needed. The consensus puts it plainly: histological findings do not differentiate the dogs that will respond to a diet change from those that need other treatment (Heilmann et al., 2026). A scope can show inflammation in a dog who then does perfectly well on food alone. So a biopsy confirms and characterises; it does not dictate the treatment ladder. The old reflex that inflammation on a biopsy equals IBD equals immunosuppress-for-life is simply not how modern CE is managed. Where steroids and gut-targeted alternatives genuinely fit, for the minority who need them, is when diet is not enough.
There is a second reason not to over-read a borderline report: biopsies are more subjective than people imagine. In a landmark study, five veterinary pathologists could not agree on their interpretation of roughly half the intestinal samples they examined (Willard et al., 2002), which is exactly why the WSAVA criteria, and later a simplified scoring model, were developed to improve consistency (Day et al., 2008; Jergens et al., 2014). This does not make a biopsy useless; it means a mild, equivocal "some inflammation" result should not, on its own, push an otherwise well dog onto strong medication it may never need.
So when is a biopsy the right call? It is reserved for dogs that have not responded to appropriate trials, or for dogs unwell enough that waiting is not safe (a markedly low blood albumin, severe or worsening signs), where the result would genuinely change what we do (Heilmann et al., 2026). For the stable dog who would have responded to a diet change, going straight to anaesthetic and scope is usually the wrong order, and an avoidable cost and risk.
When low albumin changes the plan
One situation legitimately speeds the sequence up. When CE leaks enough protein out of the bloodstream and into the bowel to drop the blood albumin, we call it protein-losing enteropathy, and it is a more serious form (Allenspach et al., 2007; Heilmann et al., 2026). A low albumin is a recognised warning sign and a reason to bring imaging and biopsy forward rather than working slowly up the staircase. The management and outlook of these cases belong to the treatment article.
A word about cats, because the same staged logic applies but the feline picture has its own wrinkle. Cats are not simply small dogs here: the inflammation-versus-lymphoma question is the reason a biopsy carries more weight in a cat, so the whole feline story is told in feline chronic enteropathy.
Patience with the staircase usually pays off
Step back and the design becomes reassuring. We start with the cheap, common, treatable things, move through a diet trial that doubles as a diagnosis, and only climb to biopsy and immunosuppression for the few who need them. That order means most dogs are diagnosed and treated without ever needing a scope or a steroid (Allenspach et al., 2007; Heilmann et al., 2026).
The single most useful thing you can do while the work-up unfolds is to give your vet what a snapshot consultation cannot capture: the pattern over time. Recording the daily faecal score and your pet's weight with the Faecal Score Tracker is exactly the data that shows whether a diet trial is working, and it lets you and your vet read the same picture rather than relying on memory (the scoring method itself is taught in describing symptoms to your vet). With that record in hand, the most productive next step is rarely dramatic: trust the order, give the diet trial a proper run, and let the response, written down day by day, do the talking.
References
- Heilmann RM, Jergens AE, Kathrani A, Allenspach K, Salavati Schmitz S, Priestnall SL, Dandrieux JRS, O'Connor AM. ACVIM-endorsed statement: consensus statement and systematic review on guidelines for the diagnosis and treatment of chronic inflammatory enteropathy in dogs. J Vet Intern Med. 2026;40(1):aalaf017.
- Allenspach K, Wieland B, Gröne A, Gaschen F. Chronic enteropathies in dogs: evaluation of risk factors for negative outcome. J Vet Intern Med. 2007;21(4):700-708. )21[700:CEIDEO]2.0.CO;2.
- Dandrieux JRS. Inflammatory bowel disease versus chronic enteropathy in dogs: are they one and the same? J Small Anim Pract. 2016;57(11):589-599.
- Williams DA, Batt RM. Diagnosis of canine exocrine pancreatic insufficiency by the assay of serum trypsin-like immunoreactivity. J Small Anim Pract. 1983;24(10):583-588. AND Williams DA, Batt RM. Sensitivity and specificity of radioimmunoassay of serum trypsin-like immunoreactivity for the diagnosis of canine exocrine pancreatic insufficiency. J Am Vet Med Assoc. 1988;192(2):195-201.
- Day MJ, Bilzer T, Mansell J, Wilcock B, Hall EJ, Jergens A, Minami T, Willard M, Washabau R; World Small Animal Veterinary Association Gastrointestinal Standardization Group. Histopathological standards for the diagnosis of gastrointestinal inflammation in endoscopic biopsy samples from the dog and cat. J Comp Pathol. 2008;138(Suppl 1):S1-S43.
- Willard MD, Jergens AE, Duncan RB, et al. Interobserver variation among histopathologic evaluations of intestinal tissues from dogs and cats. J Am Vet Med Assoc. 2002;220(8):1177-1182.
- Jergens AE, Evans RB, Ackermann M, Hostetter J, Willard M, Mansell J, Bilzer T, Wilcock B, Washabau R, Hall EJ, Minami T, Wang C, Day MJ. Design of a simplified histopathologic model for gastrointestinal inflammation in dogs. Vet Pathol. 2014;51(5):946-950.
- Marsilio S, Freiche V, Johnson E, Leo C, Langerak AW, Peters I, Ackermann MR. ACVIM consensus statement guidelines on diagnosing and distinguishing low-grade neoplastic from inflammatory lymphocytic chronic enteropathies in cats. J Vet Intern Med. 2023;37(3):794-816.
- Toresson L, Steiner JM, Suchodolski JS, Spillmann T. Oral cobalamin supplementation in dogs with chronic enteropathies and hypocobalaminemia. J Vet Intern Med. 2016;30(1):101-107.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine