
When Diet Is Not Enough: The Step-Up, and Where Steroids Actually Fit
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
A diet trial that does not work is a deflating place to land. You did everything asked: the single prescription food, nothing else past the lips, weeks of faecal scores that stubbornly refused to firm up. And the word that often comes next, steroids, can feel like a step into something heavier than you bargained for.
So let me set the tone up front. Steroids are not the start of chronic enteropathy treatment, and for most dogs not even the middle of it. They sit later on the ladder, and for a minority. The most useful thing I can do is put them, and the other immune-suppressing drugs, back in their correct place. If you are still getting your head around what chronic enteropathy is and the response-defined groups it splits into, that framework lives in chronic enteropathy explained; here we pick up where diet alone has failed.
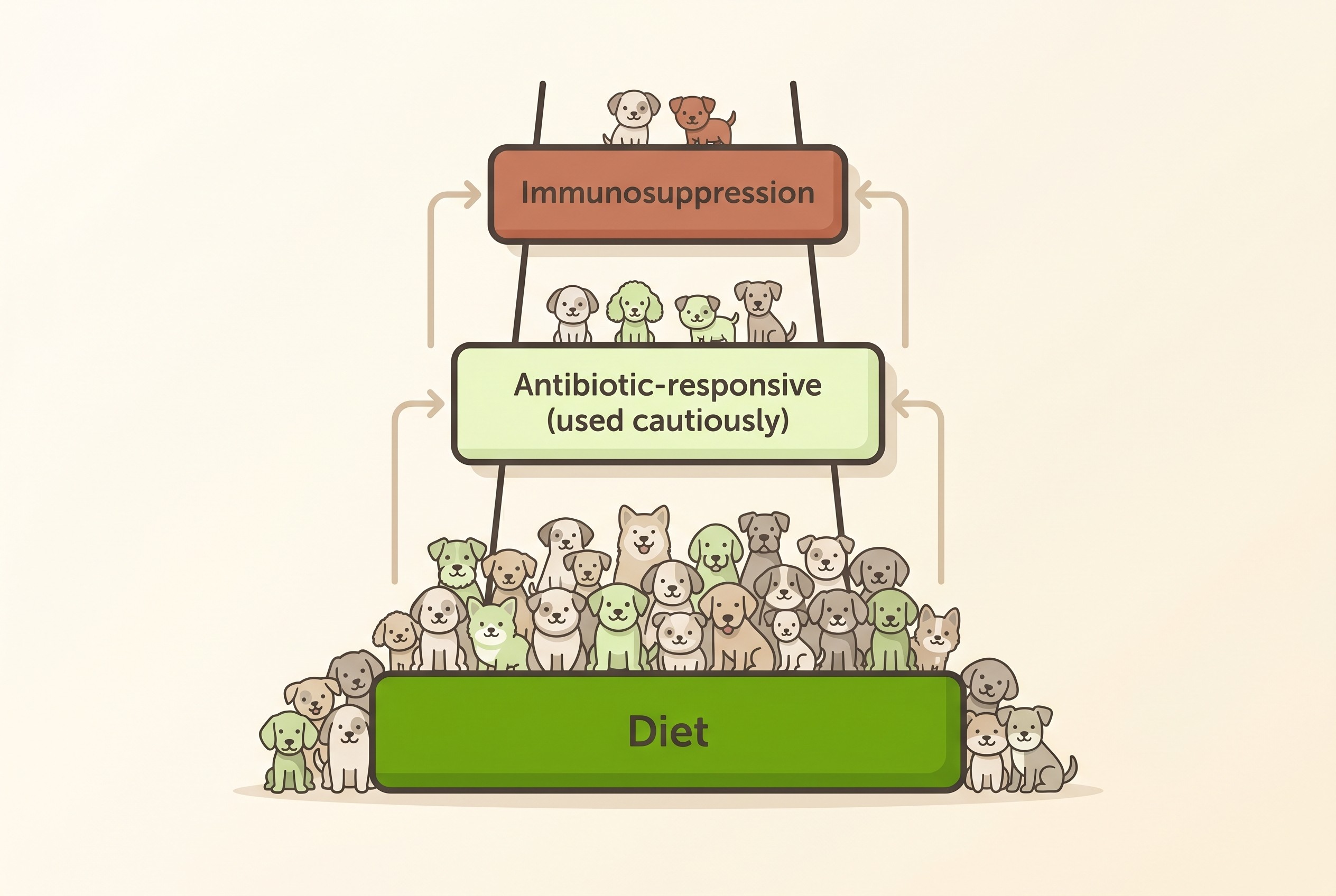
Why we climb one rung at a time
Modern chronic enteropathy treatment is sequential and response-defined, not label-defined. We do not read a biopsy report, decide a dog "has IBD", and reach for the strongest drug; we try the gentlest effective option first, and climb to the next rung only when the one below has had a fair go and failed (Dandrieux, 2016; Heilmann et al., 2026).
Diet is the bottom rung, and for most dogs the only rung they ever need. The 2026 ACVIM consensus, the governing modern statement on this disease, is unambiguous that diet "should be used first, whenever possible", and recommends a minimum of three diet trials of at least two weeks each before concluding diet has failed, with response rates running anywhere from 38 to 89% (Heilmann et al., 2026). The food-responsive group is consistently the largest, with a good long-term outlook (Allenspach et al., 2007; Dandrieux & Mansfield, 2019). The mechanics of that trial are owned by the diet trial guide, and our Diet-Trial Companion keeps that first rung disciplined, so I will only add that "we tried diet and it did not work" should mean more than one food and more than a fortnight.
The plain endpoint is that a small minority of dogs do not respond to anything we try, somewhere around 5 to 27% of cases across studies (Dandrieux & Mansfield, 2019). But notice which way round that is: the great majority do well, and two phrases shape every decision below. This is control, not cure, and the aim throughout is the lowest effective treatment (Allenspach et al., 2007; Heilmann et al., 2026).
A rung we now mostly step over
There is a middle rung on the old ladder, the antibiotic-responsive group, and the advice here has genuinely changed. For years a course of metronidazole was almost a reflex for chronic diarrhoea. No longer: the ACVIM consensus now explicitly advises against empirical antibiotics in suspected chronic enteropathy, on stewardship and microbiome grounds (Heilmann et al., 2026).
The reasoning is worth a sentence. A 14-day course of metronidazole in healthy dogs measurably reduced the richness of the gut microbiome and depleted important bacteria, changes that had not fully recovered four weeks after stopping (Pilla et al., 2020). Some dogs do respond to an antibiotic such as tylosin, but the signs commonly return within weeks of stopping, and while a low maintenance dose can hold things steady, that is managing a dependency rather than a cure, and the long-term outlook for this antibiotic-dependent group is one of the poorer ones (Kilpinen et al., 2011; Kilpinen et al., 2014; Dandrieux & Mansfield, 2019). The full case for de-emphasising antibiotics, and the narrow situations where they are still warranted, belongs to antibiotics for diarrhoea. The point here is simple: we no longer reach for them on the way up as routine.
Where steroids actually fit
So we arrive at the rung that brought you here. Glucocorticoids, the steroids, come after a fair diet trial, not before, and that ordering is not caution for its own sake. They work fast, with a median response of around five days, but precisely because they damp inflammation so effectively they can mask a treatable infection or an underlying malignancy if used too early (Heilmann et al., 2026). The diet trial, and the diagnostic work behind it in the diagnosis guide, earns us the right to use them safely.
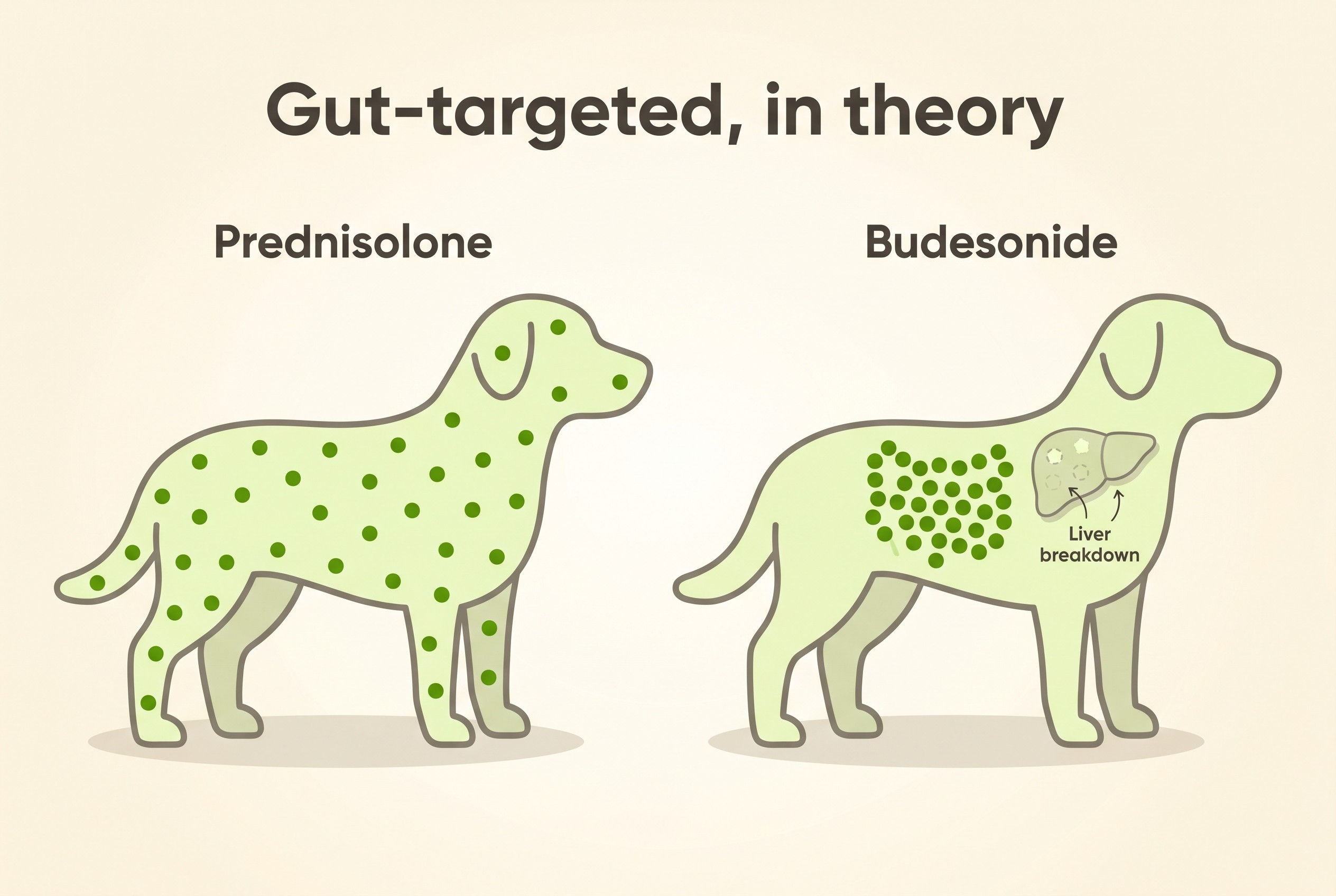
In UK practice the workhorse steroid is oral prednisolone. (You will see "prednisone" in American sources; it converts to prednisolone in the body, and prednisolone is the term to hold on to here.) The familiar alternative is budesonide, a glucocorticoid designed to act largely on the gut wall and then be broken down by the liver before much reaches the rest of the body, which in theory spares a dog the systemic steroid effects. It is a reasonable option where those side effects are a real problem, but not a free lunch: the one randomised controlled trial comparing it with prednisone found no significant difference in remission rate (78% versus 69%) and a broadly similar side-effect profile, and the gut-sparing is relative rather than absolute, since some systemic absorption still occurs (Dye et al., 2013; Coates, 2023). It is used off-licence on a vet's judgement, not a dose to administer of your own accord.
When steroids alone are not enough, or cannot be tolerated, the next options are the steroid-sparing immunosuppressants. The one with the best evidence in dogs is ciclosporin (the UK spelling of cyclosporine): in a small study of steroid-refractory dogs, oral ciclosporin given for ten weeks improved the clinical signs in 12 of 14 (Allenspach et al., 2006). It sits alongside agents such as chlorambucil, azathioprine and mycophenolate as the usual second-line choices when diet and steroids have not held the disease, all used off-licence here (Heilmann et al., 2026). Chlorambucil in particular is more a cat-and-low-grade-lymphoma agent, territory the feline chronic enteropathy guide is far better placed to cover.
The trade-offs are the real reason we climb slowly. Steroids bring increased thirst and urination, a ravenous appetite, panting, muscle loss over time, a higher infection risk and, at high doses for long, a Cushingoid, over-treated look; ciclosporin can cause vomiting and overgrowth of the gums, carries its own infection risk, and is not cheap. None of this is a reason to refuse treatment a dog genuinely needs; it is why the whole game is the lowest dose that holds the disease (Heilmann et al., 2026). Which brings us to how you tell whether a rung is working.
Knowing whether a rung is working
This is where day-to-day tracking earns its keep, and where you are not a passenger. Titrating these treatments to the lowest effective dose is not done on a hunch; it is read off the trend in three plain things: the faecal score, the body weight and the appetite. A dose that has the stool firm, the weight stable and the dog hungry-but-not-frantic is one we can start carefully reducing; a dose under which the faecal score is creeping back up is telling you something before the dog looks unwell. Logging this in the Faecal Score Tracker turns a vague "I think she is a bit better" into a line on a chart you and your vet can act on, and it is the same trend that catches the more serious slide below while there is still time to respond.
One supportive measure runs alongside the ladder rather than on it: cobalamin, vitamin B12. It is depleted in a large share of chronic-enteropathy dogs (reported at roughly 19 to 61%) and is a genuine negative prognostic factor, so it is corrected as a matter of course, and oral supplementation now works well for many dogs rather than requiring injections (Allenspach et al., 2007; Heilmann et al., 2026; Toresson et al., 2016). Its detail, with fibre, the microbiome and the flare plan, is the subject of living with chronic enteropathy, so I will hand you there.
Protein-losing enteropathy: the serious end
One finding on the bloodwork changes the picture. If a dog's blood albumin is low, that points to protein-losing enteropathy, the more serious end of this disease. Low albumin is a recognised poor prognostic factor, and these cases need closer care, often with specialist input, and sustained low-fat dietary management to stay stable (Allenspach et al., 2007; Heilmann et al., 2026).
But more serious does not mean hopeless, and it does not mean throwing every drug at once. A subset of protein-losing dogs, classically Yorkshire terriers, achieve remission and recover their albumin on a low-fat diet alone, with no immunosuppression at all (Rudinsky et al., 2017). And where the disease is inflammatory, steroid treatment on its own can be appropriate: adding a second immunosuppressant from the outset did not significantly improve survival in one cohort, and no routine test reliably predicted which dogs would do well (Salavati Schmitz et al., 2019). So even here the same disciplined logic holds: more vigilance and usually a specialist conversation, but not a death sentence and not automatically a maximal-treatment case.
A final note for any dog on these treatments: if one is suddenly off colour, the belly is painful, or they crash, that is not a wait-and-see, and our Vomiting & Diarrhoea Triage and the emergencies guide tell you when it is urgent.
So if you are standing at the foot of this ladder, worried a diagnosis means a lifetime of strong drugs, let the evidence reassure you: most dogs never climb past diet, the ones who do are usually held well on the gentlest dose that works, and even the serious end has good roads out of it. Next time you sit down with your vet, the question is not "steroids or nothing", but the far better one of which rung your dog actually needs, and how little of it will do the job.
References
- Allenspach, K., Rufenacht, S., Sauter, S., Grone, A., Steffan, J., Strehlau, G., & Gaschen, F. (2006). Pharmacokinetics and clinical efficacy of cyclosporine treatment of dogs with steroid-refractory inflammatory bowel disease. Journal of Veterinary Internal Medicine, 20(2), 239-244.
- Allenspach, K., Wieland, B., Grone, A., & Gaschen, F. (2007). Chronic enteropathies in dogs: evaluation of risk factors for negative outcome. Journal of Veterinary Internal Medicine, 21(4), 700-708.
- Coates, V. A. (2023). In dogs with chronic enteropathy (idiopathic inflammatory bowel disease) is budesonide more effective than prednisolone or prednisone in resolving clinical signs? Veterinary Evidence, 8(4).
- Dandrieux, J. R. S. (2016). Inflammatory bowel disease versus chronic enteropathy in dogs: are they one and the same? Journal of Small Animal Practice, 57(11), 589-599.
- Dandrieux, J. R. S., & Mansfield, C. S. (2019). Chronic enteropathy in canines: prevalence, impact and management strategies. Veterinary Medicine: Research and Reports, 10, 203-214.
- Dye, T. L., Diehl, K. J., Wheeler, S. L., & Westfall, D. S. (2013). Randomized, controlled trial of budesonide and prednisone for the treatment of idiopathic inflammatory bowel disease in dogs. Journal of Veterinary Internal Medicine, 27(6), 1385-1391.
- Heilmann, R. M., Jergens, A. E., Kathrani, A., et al. (2026). ACVIM-endorsed statement: consensus statement and systematic review on guidelines for the diagnosis and treatment of chronic inflammatory enteropathy in dogs. Journal of Veterinary Internal Medicine, 40(1), aalaf017.
- Kilpinen, S., Spillmann, T., Syrja, P., Skrzypczak, T., Louhelainen, M., & Westermarck, E. (2011). Effect of tylosin on dogs with suspected tylosin-responsive diarrhea: a placebo-controlled, randomized, double-blinded, prospective clinical trial. Acta Veterinaria Scandinavica, 53, 26.
- Kilpinen, S., Spillmann, T., & Westermarck, E. (2014). Efficacy of two low-dose oral tylosin regimens in controlling the relapse of diarrhea in dogs with tylosin-responsive diarrhea: a prospective, single-blinded, two-arm parallel, clinical field trial. Acta Veterinaria Scandinavica, 56, 43.
- Pilla, R., Gaschen, F. P., Barr, J. W., Olson, E., Honneffer, J., Guard, B. C., Blake, A. B., Villanueva, D., Khattab, M. R., AlShawaqfeh, M. K., Lidbury, J. A., Steiner, J. M., & Suchodolski, J. S. (2020). Effects of metronidazole on the fecal microbiome and metabolome in healthy dogs. Journal of Veterinary Internal Medicine, 34(5), 1853-1866.
- Rudinsky, A. J., Howard, J. P., Bishop, M. A., Sherding, R. G., Parker, V. J., & Gilor, C. (2017). Dietary management of presumptive protein-losing enteropathy in Yorkshire terriers. Journal of Small Animal Practice, 58(2), 103-108.
- Salavati Schmitz, S., Gow, A., Bommer, N., Morrison, L., & Mellanby, R. (2019). Diagnostic features, treatment, and outcome of dogs with inflammatory protein-losing enteropathy. Journal of Veterinary Internal Medicine, 33(5), 2005-2013.
- Toresson, L., Steiner, J. M., Suchodolski, J. S., & Spillmann, T. (2016). Oral cobalamin supplementation in dogs with chronic enteropathies and hypocobalaminemia. Journal of Veterinary Internal Medicine, 30(1), 101-107.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine