
Keeping a Seizure Diary (and Why It Changes Your Vet Visits)
Claire Greenway
MRCVS
Your vet will almost never see your dog have a seizure. By the time you reach the surgery the event is over, and what is left to go on is your account of it. So the single most important piece of evidence in your dog's diagnosis and treatment plan is not a blood test or a scan. It is the record you keep at home. The international veterinary epilepsy task force, whose consensus guidelines underpin how this condition is diagnosed and treated, puts it plainly: "A detailed and accurate history is the foundation for investigation of the seizure patient" (De Risio et al., 2015).
The diary, then, is the one piece of this you genuinely control. You cannot will the next seizure away, but you can keep a clear, dated record, and doing it well is the most useful thing you can do between vet visits. I will cover why it matters, what to write down, and how it changes the consulting room. Triggers, filming an event, and the detail behind the emergency thresholds each have their own article, linked as we go.
What the diary is really for
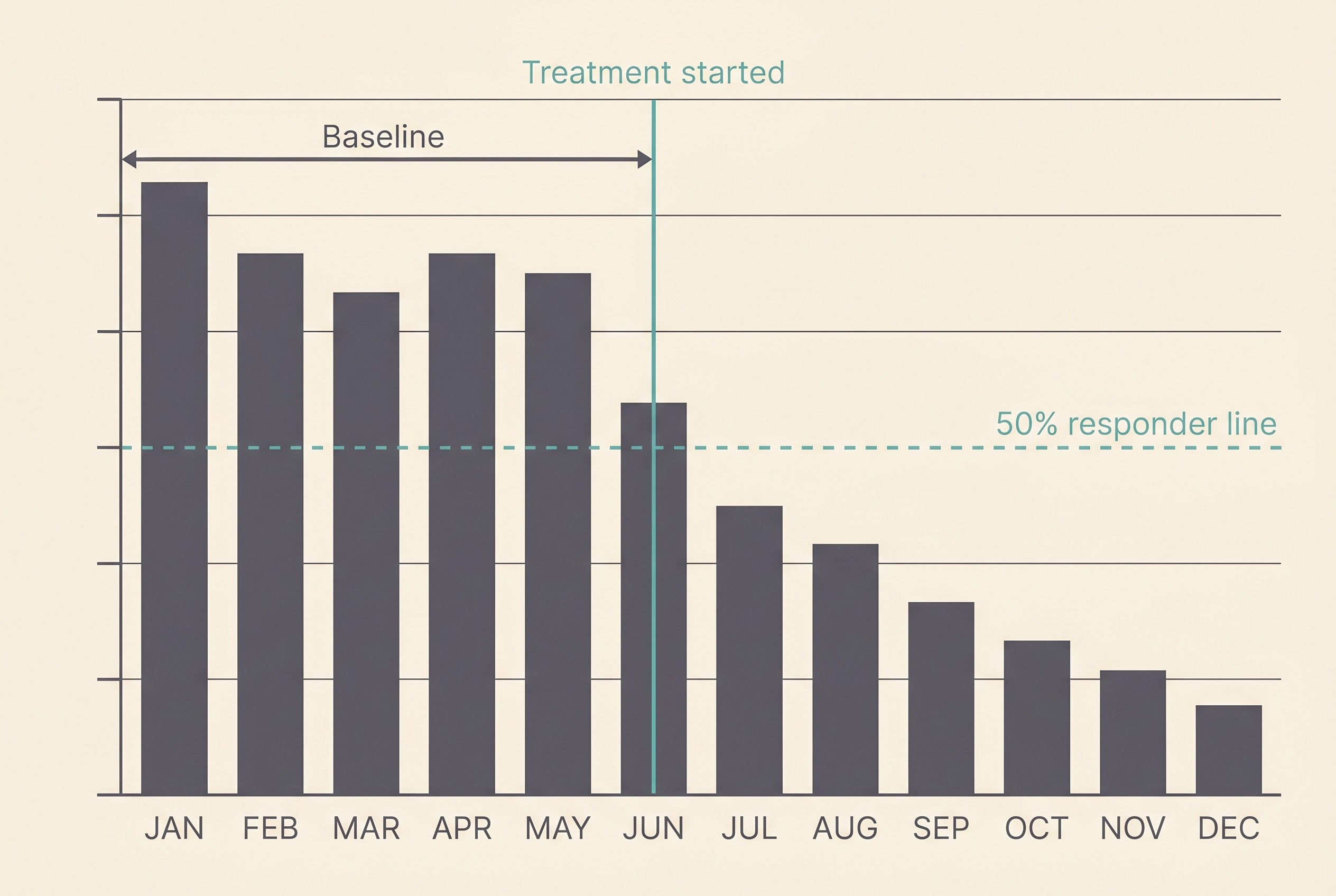
Start with what the diary is really for: counting. Seizure frequency, how many seizures over how much time, is the number your vet doses against and judges treatment by. The IVETF guidelines suggest treatment is generally warranted once a dog has had two or more seizures within a six-month period (Bhatti et al., 2015), and you can only answer that question if someone has kept count, with dates. Once treatment starts, success is measured the same way, by comparing seizure frequency after the drug against the frequency before it (Potschka et al., 2015). A "responder" is conventionally a dog whose seizures drop by at least 50% against its pre-treatment baseline (Potschka et al., 2015; Bhatti et al., 2015), and you cannot know whether your dog has hit that mark without numbers from either side of the change. Why the goal is control rather than cure is its own subject in realistic goals: control, not cure; here, the diary is simply what makes that judgement possible.
The other thing it does is catch what memory cannot. After a seizure you are not at your most precise, and most owners asked weeks later reach for a vague "a few, maybe getting more often". That is not a failing. It is how frightened humans remember frightening things. A contemporaneous log turns that fog into a dated, countable record, and the IVETF names a written seizure diary as a recognised way to establish baseline seizure data (Potschka et al., 2015). The two things memory loses first are exactly the two that matter most: whether seizures are clustering, and whether the trend is creeping upward.
What to record
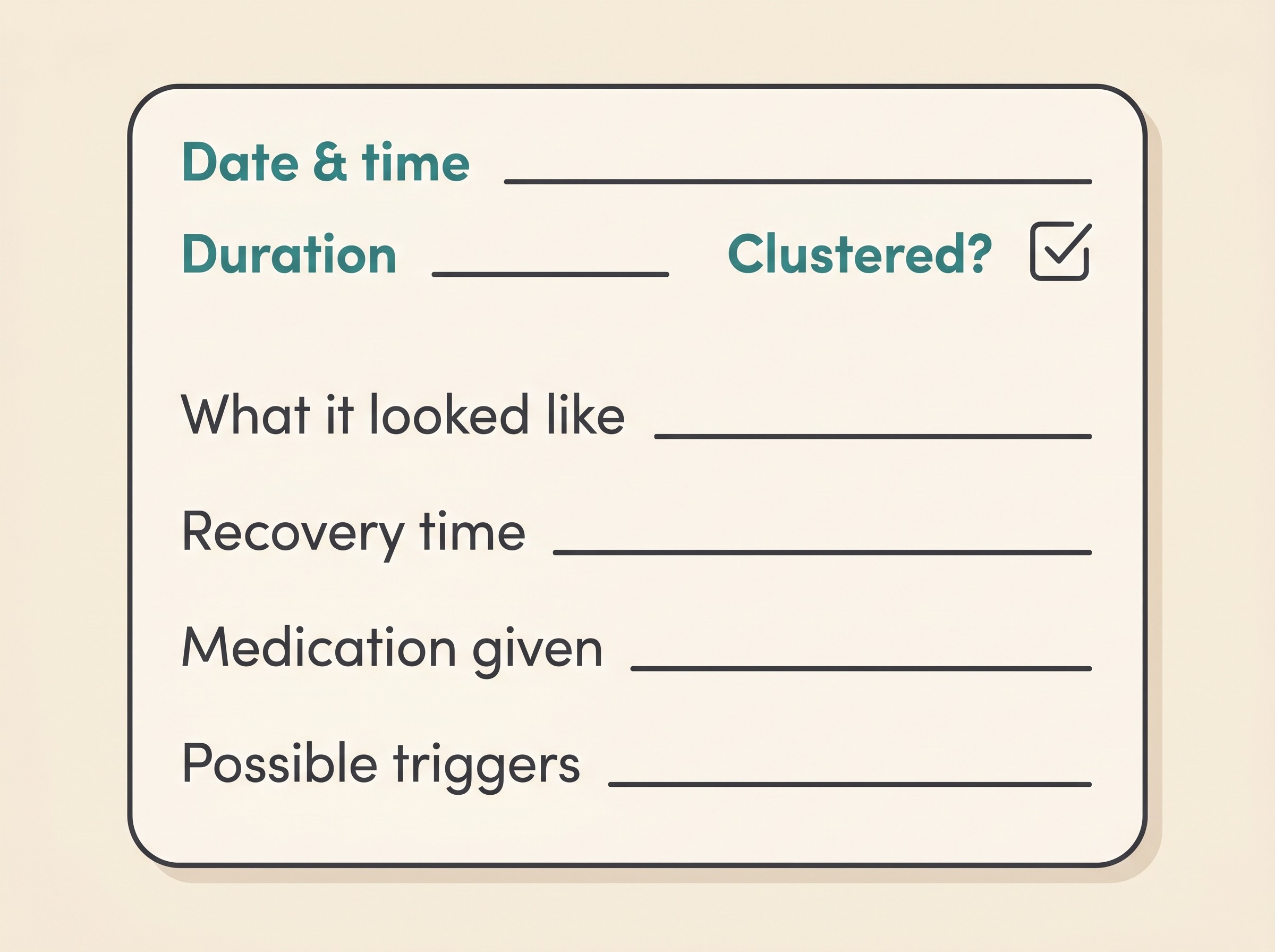
So what goes in it? The IVETF outcome consensus is direct: to judge treatment fairly, "as many data should be collected as possible", and it names the parameters that matter (Potschka et al., 2015). In plain owner-facing terms:
- Date and time, and how long it lasted. Time the seizure itself in seconds and minutes. Duration matters both for spotting patterns and for the emergency line below, and over weeks these dated entries give your vet the frequency, the seizure days, and the seizure-free intervals between them (Potschka et al., 2015).
- What it looked like. Generalised (whole-body collapse, stiffening and paddling) or focal (a localised twitch, a stare, one limb or one side of the face), a distinction the consensus treats as meaningful (Potschka et al., 2015). A few plain words are plenty; the full picture lives in what a seizure actually looks like, and a short video beats any description, which is why filming a seizure is its own guide.
- Whether they clustered. If there was more than one seizure close together, note roughly how many: the consensus tracks clusters, the average number per cluster, and any episode of status epilepticus (Potschka et al., 2015).
- The recovery afterwards. How long your dog was "not quite right" and how severe (pacing, disorientation, hunger, temporary blindness): the consensus records the severity and duration of these post-ictal signs (Potschka et al., 2015), covered in depth in the hours afterwards.
- Medication and any missed doses. What you gave, anything late or missed, and any rescue medication, because drug administration and compliance are part of judging outcome fairly (Potschka et al., 2015).
- Possible triggers and context. Poor sleep, a stressful day, the time of year. Note them, but do not try to decide which are "real" causes; that analysis belongs to identifying and managing seizure triggers.
If that feels like a lot in a frightening moment, hold onto the simple version: how many, how long, how often. Everything else is texture. The headline three are what the treatment is built on.
What it does in the consulting room
Because your vet rarely witnesses a seizure, your diary is what they actually read the appointment from (De Risio et al., 2015; Potschka et al., 2015). It converts a vague "he has had a few bad spells lately" into a dated frequency curve a vet can act on, and it lets the two of you see whether a change really worked: when the dose goes up or a new drug comes in, the only reliable way to judge it is to compare the months before against the months after on the same measure (Potschka et al., 2015). The IVETF guidelines explicitly list "the importance of maintaining a detailed seizure diary" among the things owners should be taught (Bhatti et al., 2015). This is not a habit you have invented. It is part of the recommended standard of care.
And the record is about more than the count. Research consistently finds that owners rate their dog's quality of life as more important than seizure frequency, and that dogs with higher seizure frequency, and those on three or more anti-seizure drugs, are at the greatest risk of reduced quality of life, with dog and owner wellbeing closely linked (Packer & Volk, 2015). So a genuinely useful diary also tracks how your dog is in themselves between seizures, and how you are coping. That lets the conversation weigh control against side effects rather than chase a lower number at any cost, and it has its own home in the emotional toll of caring for a pet with epilepsy.
Where consistency tends to break
I would be doing you a disservice if I made this sound effortless. Keeping it up is the hard part, and owners are human. In a study of owners of dogs with epilepsy, median compliance with the medication itself was just 56%, only a third (33%) were more than 80% compliant, and during the patches when owners slipped, dogs missed a median of six days of treatment (Booth et al., 2021). I share that not to alarm you but to take the pressure off: if you have forgotten a dose or missed logging an event, you are in very normal company.
The same study points to what helps: simpler regimens were easier to stick to, with a lower daily dosing frequency linked to better compliance (Booth et al., 2021). So build the medication and the log into one fixed daily routine and tie logging to dosing, so the two habits hold each other up. The deeper guidance on adherence, and the firm rule never to stop an anti-seizure drug abruptly, live in giving medication reliably. The goal is a sustainable habit, not a perfect record, and a tool that turns logging into a few taps removes most of the friction that makes people give up.
The emergency line (know it before you need it)
Because you will often be reaching for the diary mid-event, you need the emergency threshold to hand. Plainly: a seizure lasting more than five minutes, or two or more seizures in 24 hours, or seizures running into one another without your dog recovering in between, is an emergency. Contact your vet or an emergency clinic now (Berendt et al., 2015). A single short seizure that your dog recovers from is frightening, but it is not, by itself, an emergency. Still log it, and still tell your vet.
This is exactly why timing each seizure and counting them within a day are core diary fields: the clock and the count tell you which side of that line you are on. The full reasoning, and what the emergency clinic actually does, lives in is this an emergency? Status epilepticus and cluster seizures. Read it now, while things are calm, rather than for the first time at 2am.
Doing it well: the Seizure Diary tool
A notebook is far better than nothing. But the friction that defeats most paper diaries, finding it, dating it, doing the counting, is exactly what the Seizure Diary is built to remove. Its features map straight onto what your vet needs:
- a one-tap timer, so you capture duration accurately in the moment rather than guessing later when seconds have blurred into "a minute or two";
- a frequency chart that turns your logged events into the before-and-after trend line your vet doses against;
- an emergency flag reflecting the more-than-five-minutes and two-or-more-in-24-hours line;
- a vet-ready export, so you can hand over or send ahead a clean record before the appointment;
- and the ability to log while logged out and claim the record later, because many people meet this condition in a moment of pure panic, and nothing you capture then should be lost just because you had not signed up yet.
A note for cat owners
Everything here applies just as much to cats. The record is every bit as central, frequency is still the metric, and the same emergency line holds: time it, count it, and treat more than five minutes or two or more in 24 hours as an emergency. Cats present and are treated differently in important ways, and those feline specifics belong to the cat articles. The principle, though, does not change: your contemporaneous record is the foundation the whole plan is built on.
Make it the one thing you control
The diary is the part of epilepsy you fully own, and the most useful thing you can do between appointments (De Risio et al., 2015; Potschka et al., 2015). So make it easy on yourself. Log at a fixed time, tied to a dose. Keep the Seizure Diary on your phone's home screen. Brief everyone who cares for your pet, the dog-walker, the family member, the boarding kennel, so an event is captured even when you are not there. And bring the export, or send it ahead, to every appointment. Do that, and you walk into each visit with the one thing your vet most needs and can rarely get any other way: a clear, true picture of what has really been happening.
References
- De Risio L, Bhatti S, Muñana K, Penderis J, Stein V, Tipold A, Berendt M, Farquhar R, Fischer A, Long S, Mandigers PJM, Matiasek K, Packer RMA, Pakozdy A, Patterson E, Platt S, Podell M, Potschka H, Pumarola MB, Rusbridge C, Volk HA. International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research. 2015;11:148.
- Potschka H, Fischer A, Löscher W, Patterson N, Bhatti S, Berendt M, De Risio L, Farquhar R, Long S, Mandigers PJM, Matiasek K, Muñana K, Pakozdy A, Penderis J, Platt S, Podell M, Rusbridge C, Stein VM, Tipold A, Volk HA. International veterinary epilepsy task force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research. 2015;11:177.
- Bhatti SFM, De Risio L, Muñana K, Penderis J, Stein VM, Tipold A, Berendt M, Farquhar RG, Fischer A, Long S, Mandigers PJM, Matiasek K, Packer RMA, Pakozdy A, Patterson EE, Platt S, Podell M, Potschka H, Rusbridge C, Volk HA. International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research. 2015;11:176.
- Berendt M, Farquhar RG, Mandigers PJM, Pakozdy A, Bhatti SFM, De Risio L, Fischer A, Long S, Matiasek K, Muñana K, Patterson EE, Penderis J, Platt S, Podell M, Potschka H, Pumarola MB, Rusbridge C, Stein VM, Tipold A, Volk HA. International veterinary epilepsy task force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research. 2015;11:182.
- Booth S, Meller S, Packer RMA, Farquhar R, Maddison JE, Volk HA. Owner compliance in canine epilepsy. Veterinary Record. 2021;188(4):e16.
- Packer RMA, Volk HA. Epilepsy beyond seizures: a review of the impact of epilepsy and its comorbidities on health-related quality of life in dogs. Veterinary Record. 2015;177(12):306-315.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Seizure Diary
PDF · 236 KBThe record your vet doses against. Log every seizure: when it happened, how long it lasted, whether it came in a cluster, and how recovery went. Frequency is the number treatment is adjusted against, so a good diary is the single most useful thing you can bring to an appointment.

Trigger Log
PDF · 132 KBA daily log to spot the patterns that set seizures off. Track sleep, stress, missed doses and more alongside seizure days, then look for what keeps turning up in the day or two before. The best-supported triggers are stress, disrupted sleep, hormonal cycles and missed medication.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine