Is This an Emergency? Status Epilepticus and Cluster Seizures
Dr. Alastair Greenway
MRCVS
You need an answer now, not a lecture, so here it is.
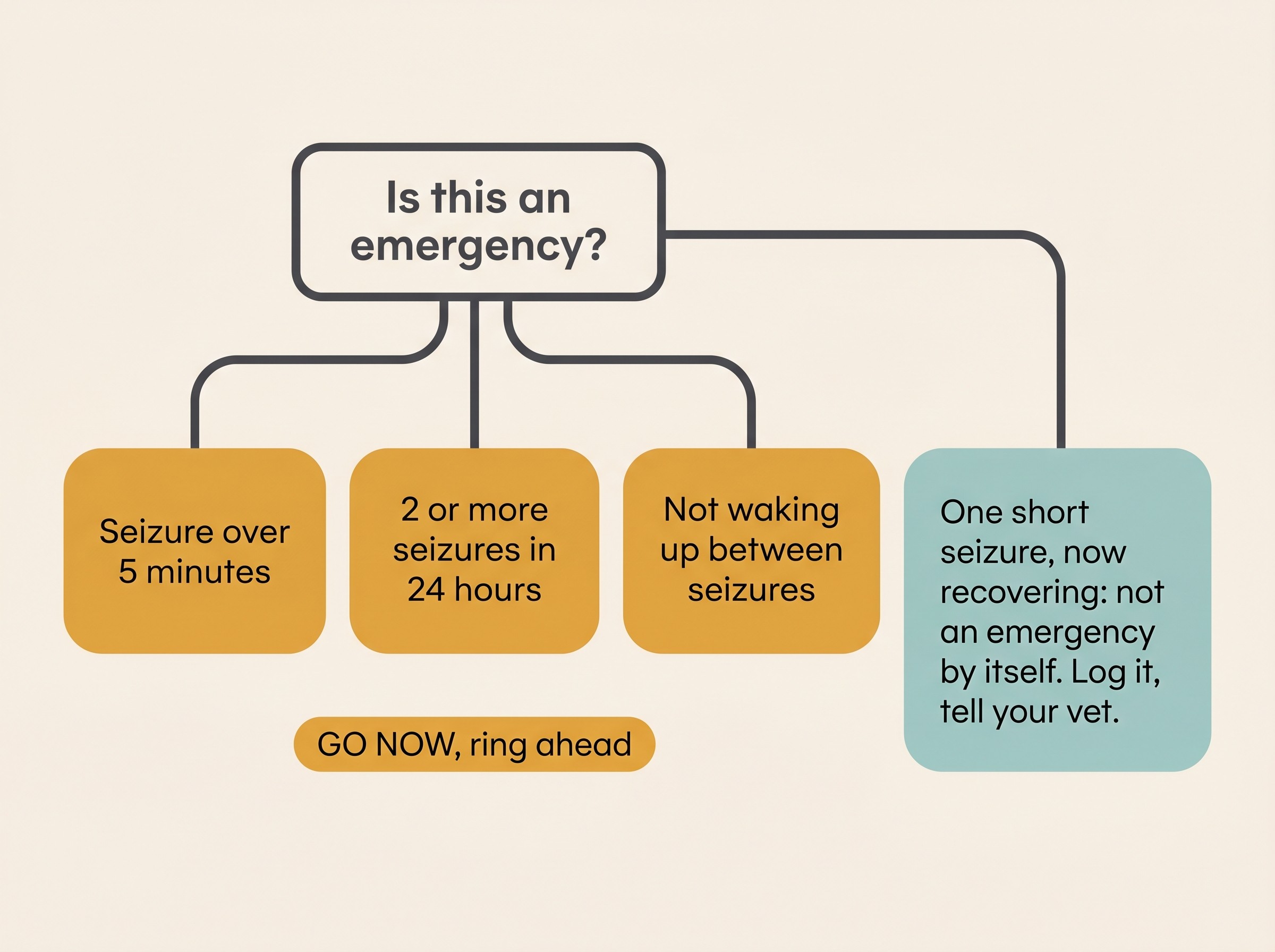
Go to the vet or the emergency clinic straight away, and ring ahead so they're ready, if any of these is true:
- A single seizure has lasted more than 5 minutes. Time it from the moment it starts, and if you're not certain, treat the clock as if it's already past 5.
- Your pet has had two or more seizures in 24 hours. That's a cluster, and it counts even if each one was short and they seemed to recover in between.
- Seizures are running into each other without your pet fully coming round between them.
If none of those applies, and your pet had one seizure that stopped on its own and is now coming back to themselves, you are almost certainly not in an emergency. It's still worth ringing your vet, especially after a first-ever seizure, but you have time.
That's the decision. The rest of this article explains why those three lines are the lines, and what the emergency team will do. If you're mid-event and unsure what to do with your hands, our guide to seizure first aid is the one to open. This article is about recognising the emergency and the decision to go.
Two emergencies, and why the names matter
Two distinct things send people to the emergency clinic, and it helps to know which you're dealing with.
Status epilepticus is the more dangerous. It means either one continuous seizure that doesn't stop, or repeated seizures with no recovery of consciousness in between, so it becomes one long event rather than separate ones (Charalambous et al., 2024). The number that matters in practice is 5 minutes: a generalised convulsive seizure lasting 5 minutes or more is unlikely to stop on its own, and should be treated as status epilepticus from that point (De Risio et al., 2015). Hold two numbers in your head. Five minutes is when you act, because waiting has stopped being safe. Around 30 minutes is the damage point, when lasting brain injury and the death of brain cells become likely (Charalambous et al., 2024). Moving fast keeps your pet well away from that second number.
Cluster seizures, sometimes called acute repetitive seizures, mean two or more separate seizures within a 24-hour period, with your pet recovering in between each one (Charalambous et al., 2024). That recovery is the key difference. In status they don't come round; in a cluster they do, but the seizures keep coming. Both are emergencies, because a cluster can tip into status, and because the brain has clearly become unstable.
Set this against a normal single seizure. A typical isolated epileptic seizure is brief, usually under two to three minutes (Berendt et al., 2015). It can feel like forever to watch, and most owners wildly overestimate how long one lasted, which is exactly why timing it on a clock matters. So if yours genuinely runs past 5 minutes by the clock, that's not just a long ordinary seizure. It's a different and more serious situation.
Why waiting it out works against you
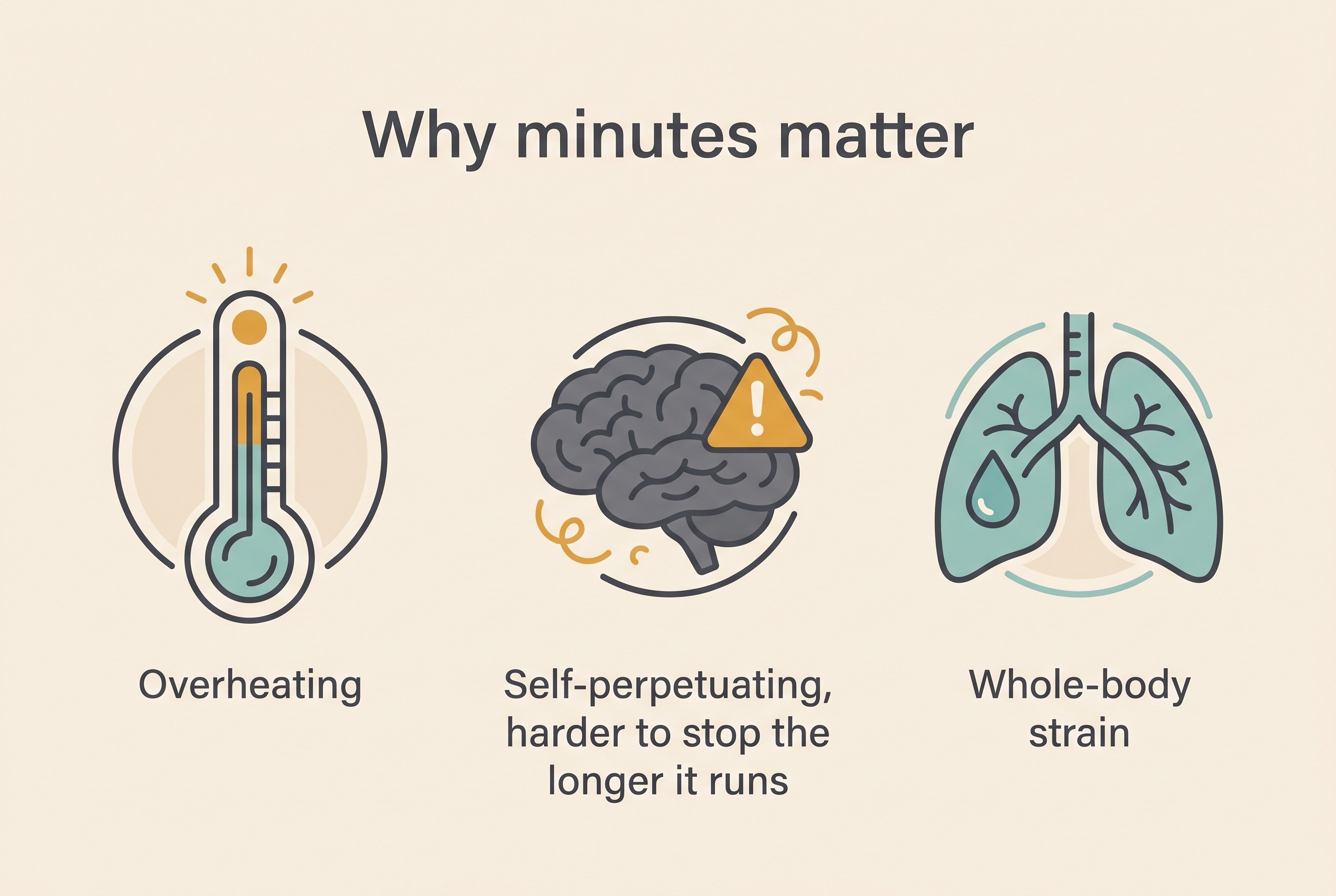
It's natural to hope a seizure will just stop if you give it a few more minutes. With status epilepticus and clusters, that instinct works against you, for three concrete reasons.
Overheating. A convulsing body is doing sustained, violent muscle work, and that generates a lot of heat with no way to shed it. Dangerously high body temperature, hyperthermia, is a real risk of a prolonged or repeated seizure, and pets that arrive at the clinic already overheated tend to do worse (Saito et al., 2001).
The seizure becomes self-perpetuating. A seizure isn't only dangerous because it's long. It gets harder to stop the longer it runs, as the brain's own braking mechanisms, the ones that would normally bring a seizure to an end, begin to fail (Charalambous et al., 2024). That's the whole logic behind the 5-minute rule: act while it's still easy to stop.
The rest of the body suffers too. Beyond the brain, prolonged seizure activity drags the whole system out of balance, with metabolic disturbances and low blood oxygen among the complications the emergency team has to correct (Charalambous et al., 2024).
Put together, that's why this is a genuine neurological emergency, with mortality from status epilepticus reported across animal studies at roughly 25% to 38% (Charalambous et al., 2024). I'm telling you that not to frighten you, but to explain why "let's see if it settles" is the wrong call. The faster your pet reaches someone who can stop the seizure, the better the odds.
There's a longer-term reason to take this seriously too. In one study of dogs with idiopathic epilepsy, those who had episodes of status epilepticus lived on average 8.3 years, against 11.3 years for those who didn't, and about a third of the status dogs eventually died of causes directly linked to their seizure disorder (Saito et al., 2001). That's a small, older, single-centre study, so don't read it as a sentence handed to your own dog. Read it as motivation: this is exactly the kind of event worth preventing and treating fast.
What the emergency team will actually do (it's treatable)
You're not driving towards something hopeless. These are treatable emergencies that clinics deal with regularly, with a clear stepwise approach.
The first move is usually a fast-acting benzodiazepine sedative, midazolam or diazepam, given into a vein or up the nose. These are considered the most effective and safest first step to break a seizure (Charalambous et al., 2024). If that doesn't fully settle things, the team escalates to intravenous anti-seizure drugs, typically levetiracetam and/or phenobarbital. For the small number of cases that still won't stop, the next step is a general anaesthetic, using drugs such as propofol or ketamine, to shut the seizure down completely while the brain settles (Charalambous et al., 2024).
Alongside stopping the seizure, the team works on everything it has knocked out of kilter: actively cooling a pet that's overheated, correcting the metabolic disturbances and low oxygen, and treating any underlying cause (Charalambous et al., 2024). That supportive care matters just as much as the drugs, and the single most useful thing you can do is get there quickly and ring ahead, so they can have a team and a line ready as you arrive.
When your pet is a known "clusterer"
Some dogs, and to a lesser and less well-studied extent some cats, have a pattern of clustering. For them a vet may prescribe an at-home rescue plan: a benzodiazepine you give yourself, intranasal midazolam or rectal diazepam, sometimes with a short pulse of oral levetiracetam, all to a protocol your own vet has written for your own pet (Charalambous et al., 2024).
I'm flagging that rather than walking you through it, for one safety reason: rescue medication is only ever given to a plan your vet has set, never to a dose you've guessed or borrowed from a forum. Our guide to managing cluster seizures at home covers the how-to, and building the written plan with your vet lives in your status epilepticus emergency plan. Having one ready before you need it is one of the most reassuring things you can do.
One related point belongs in any conversation about clusters: never stop your pet's regular anti-seizure medication suddenly, because abruptly withdrawing these drugs can itself trigger cluster seizures or status epilepticus (Bhatti et al., 2015). If side effects or cost are making daily dosing hard, that's a conversation for your vet, not a reason to stop on your own.
When it isn't an emergency, by itself
It's just as important to know when you can breathe out. A single seizure that stops on its own within a minute or two, after which your pet gradually comes back to themselves, is frightening but not, in itself, an emergency. It doesn't need a midnight dash to the clinic.
What it does need is logging, and a phone call to your vet in normal hours, particularly if it's the first one you've ever seen. The disorientated, wobbly, briefly blind or ravenously hungry spell afterwards is the post-ictal phase, a normal part of recovery rather than a new emergency. If that's where you are now, the hours afterwards explains what's normal and what isn't.
This is exactly where the Seizure Diary earns its place. The two facts that drive the emergency decision, how long a seizure lasted and how many have happened in 24 hours, are precisely what the diary captures. Starting the timer the moment a seizure begins gives you the one number you can't judge by feel, and a logged count flags a cluster rather than leaving you to do the maths in a panic. Timing it and logging it isn't admin. It's the thing that tells you, and your vet, whether this is the night you go.
A note for cat owners
Everything above applies to cats just as it does to dogs: the same three lines hold, and all mean go now.
There's one feline-specific emergency worth having on your radar, because it's common and entirely preventable. Permethrin and other pyrethroid insecticides, the active ingredients in many flea spot-on products made for dogs, are highly toxic to cats. It usually happens when a dog's flea treatment is accidentally applied to a cat, or when a cat grooms a dog that's recently been treated. The signs include drooling, twitching of the ears and face, generalised muscle tremors, overheating and then seizures, and it can be fatal. Onset is usually within a few hours but can be delayed up to 24 hours (Boland & Angles, 2010). If there's any chance your seizing cat has been exposed to a dog flea product, say so when you ring the clinic, because it changes how they treat. The deeper feline picture is in what causes seizures in cats and what seizures look like in cats.
The thing worth carrying forward, once tonight is over, is that you don't have to face the next one cold. Agree with your vet, in advance, exactly what your line is and what you'll do when you reach it. The owners who cope best with clusters and status aren't the ones who never feel afraid. They're the ones who decided what "go now" looks like before the night it mattered.
References
- Berendt, M., Farquhar, R. G., Mandigers, P. J. J., Pakozdy, A., Bhatti, S. F. M., De Risio, L., Fischer, A., Long, S., Matiasek, K., Muñana, K., Patterson, E. E., Penderis, J., Platt, S., Podell, M., Potschka, H., Pumarola, M. B., Rusbridge, C., Stein, V. M., Tipold, A., & Volk, H. A. (2015). International veterinary epilepsy task force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research, 11, 182.
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Boland, L. A., & Angles, J. M. (2010). Feline permethrin toxicity: retrospective study of 42 cases. Journal of Feline Medicine and Surgery, 12(2), 61-71.
- Charalambous, M., Muñana, K., Patterson, E. E., Platt, S. R., & Volk, H. A. (2024). ACVIM Consensus Statement on the management of status epilepticus and cluster seizures in dogs and cats. Journal of Veterinary Internal Medicine, 38(1), 19-40.
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Mandigers, P. J. J., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Rusbridge, C., & Volk, H. A. (2015). International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- Saito, M., Muñana, K. R., Sharp, N. J. H., & Olby, N. J. (2001). Risk factors for development of status epilepticus in dogs with idiopathic epilepsy and effects of status epilepticus on outcome and survival time: 32 cases (1990-1996). Journal of the American Veterinary Medical Association, 219(5), 618-623.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Seizure First-Aid Card
PDF · 179 KBWhat to do, and what not to do, during a seizure, on one fridge-ready card. The calm steps that keep your pet safe, the things to avoid (hands away from the mouth), and the clear line for when a seizure becomes an emergency.

Status Epilepticus Emergency Plan
PDF · 224 KBA one-page plan to complete with your vet and pin up at home. The emergency thresholds, who to call, and a place to record any prescribed rescue medication exactly as your vet has set it, so panic never erases the plan when a long seizure happens.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine