
Your Status Epilepticus Emergency Plan
Claire Greenway
MRCVS
I've watched this play out more times than I'd like. A dog who has had seizures for a while has a bad one, a long one, and the owner who asked all the right questions at the calm consultations freezes. The out-of-hours number is somewhere in an email. The rescue medicine is in a drawer, possibly in date, nobody is quite sure. Precious minutes go by, not because anyone did anything wrong, but because panic erases recall. The capable owner I met in the consulting room is gone, replaced by a frightened person trying to think while their dog convulses on the floor.
A written emergency plan exists for exactly that moment. It does the remembering when you can't. This isn't a tidy-minded nicety, because the consensus is blunt about what's at stake: status epilepticus and cluster seizures are "common challenging disorders with complex pathophysiology, rapidly progressive drug-resistant and self-sustaining character, and high morbidity and mortality" (Charalambous et al., 2024). The longer a severe seizure runs, the harder it becomes to stop and the worse the outlook. Your role is bigger than you might think: owners "have a substantial role in seizure control because appropriate administration of antiseizure drugs at home could prevent seizure progression to SE or reduce the risk of progression to more refractory stages" (Charalambous et al., 2021). When it counts, you are the first responder, and the plan lets you act like one under pressure.
This article is about building that plan, the one-page document you agree with your vet and pin to the fridge. It doesn't teach you which rescue medicine to give or how, that's owned by managing cluster seizures at home, and it doesn't relitigate why these thresholds are emergencies, which lives in is this an emergency?. This is the "what do I do, in what order, with which numbers" document.
Why five minutes is the line
The most important number in the plan is five minutes. A seizure that lasts longer than that is unlikely to stop on its own: the consensus defines status epilepticus as seizure activity persisting past the five-minute mark, the point at which "the mechanisms responsible for seizure termination" have failed, with the risk of lasting harm, neuronal death and altered brain networks, mounting after thirty minutes (Charalambous et al., 2024). The brain's own brakes for a seizure have stopped working. That's why the plan acts rather than waits and sees: status epilepticus "can lead to irreversible brain damage and systemic complications, especially if treatment is delayed" (Charalambous et al., 2024).
Put the threshold line at the very top
Anyone reading your plan, a panicking teenager, a dog-sitter, a relative, needs to know in one glance when it activates. So the top line states the emergency definition plainly:
A single seizure lasting more than five minutes, OR two or more seizures in 24 hours (cluster seizures), OR seizures running back-to-back without full recovery in between = emergency. Contact your vet or the nearest emergency clinic now, and ring ahead so they're ready for you.
A single short seizure with full recovery is frightening, but it is not, by itself, an emergency. Still log it and tell your vet, but you don't need to drive into the night for one brief seizure your dog recovers cleanly from. Cluster seizures are defined as more than two self-limiting seizures over 24 hours, status epilepticus as activity past that five-minute mark (Charalambous et al., 2024; De Risio et al., 2015). The reasoning behind the line, the hyperthermia, the self-perpetuation, what the emergency team does when you arrive, belongs to is this an emergency?.
What actually goes in the plan
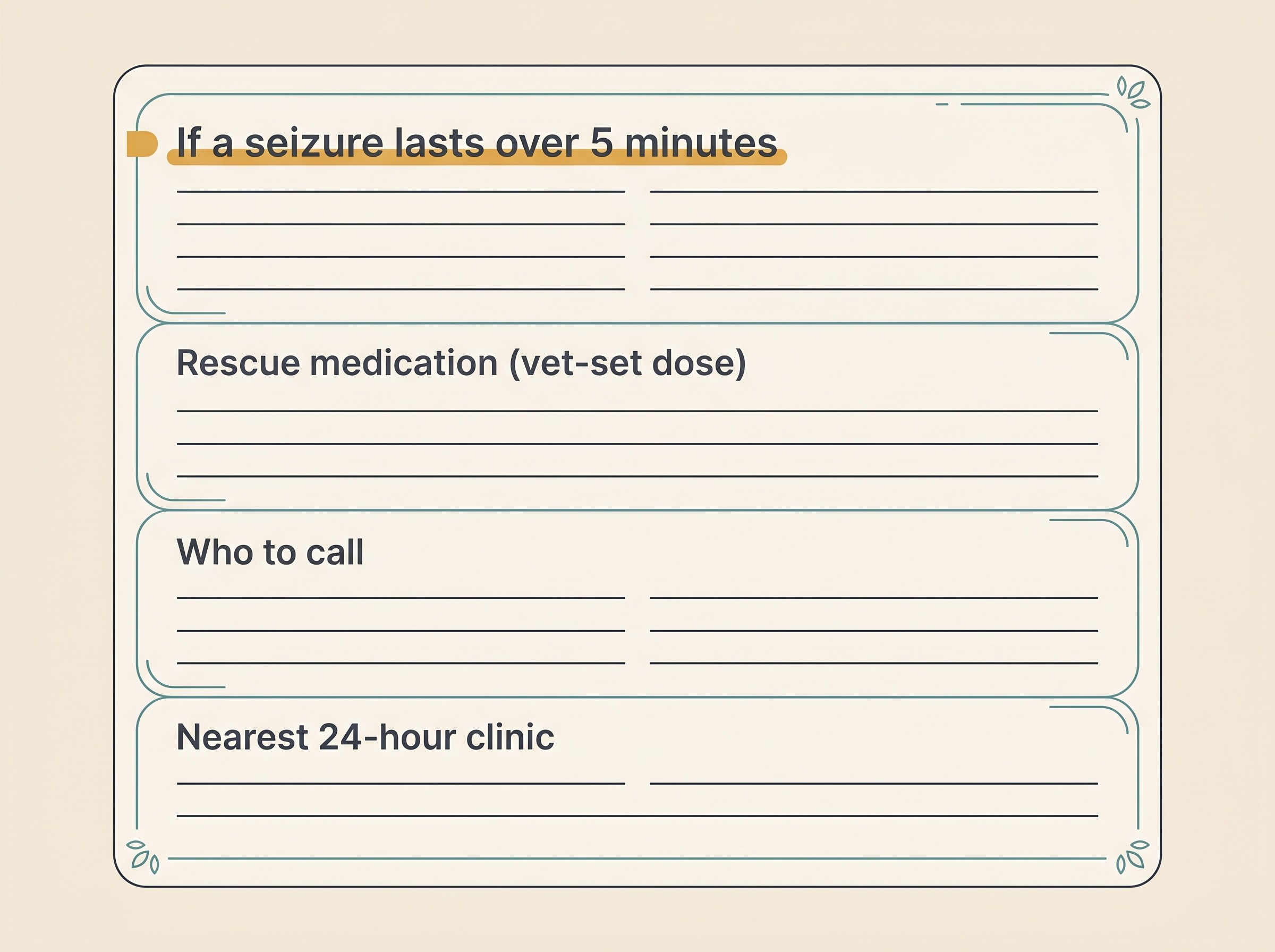
Build this with your vet, in order. Each section answers one question, and together they take you from "something is happening" to "we're getting help" without you having to think.
1. The threshold line. The emergency definition above, written at the top so anyone holding the plan knows it's time to act.
2. The rescue-medication step, exactly as your vet has set it. This is the heart of the plan. If your dog is prone to clusters, your vet may prescribe a rescue medicine to give at home, and the plan records exactly what they've directed: the medicine, the dose, how and when to give it, and how long to wait. It is filled in by your vet, for your individual dog, so please don't treat anything you read online, here or anywhere, as a dose to choose yourself. The technique and storage detail lives in managing cluster seizures at home; on the plan it's a box your vet completes and you follow. There's a clinical reason it happens early: a rescue benzodiazepine's effect "may gradually decrease with prolonged SE due to reduced synaptic targets" (Charalambous et al., 2021), so it works better the sooner it's given.
3. The "leave for the vet now" trigger. The line that gets you into the car. Your vet will specify it, typically if the seizure hasn't stopped, or a second one begins, within the time they tell you. "Should we go yet?" is the question panic answers worst, so make the decision in advance, in pen.
4. Who to call and where to go. The daytime practice number. The separate out-of-hours or emergency number, often a different clinic in a different place. The address, and a route you've actually driven. At 3am with your hands shaking, you don't want to be hunting for it.
5. Your pet's key details for the clinic. The receiving vet needs these first, and you won't reliably recall them under stress: current anti-seizure medications and doses, the date of the last blood-level check, any known triggers, and, crucially, whether you've given the rescue dose and at what time. That last detail shapes what the emergency team does next.
Getting the kit ready behind the plan
A plan is only as good as the kit behind it. This is the part you can sort out this week.
Keep the rescue medication stocked and in date. A perfect plan is useless if the medicine expired in March, or you used the last dose two clusters ago and forgot to reorder. Build in a recurring reminder to check the expiry and refill the prescription. Don't stockpile and don't self-prescribe. It's vet-supplied to your protocol, but do make sure it's there when you need it.
Have the carrier, lead and route ready. Know the fastest way to the emergency clinic before the night you need it, ideally having driven it once. For a cat, that means the carrier is accessible, not buried in the loft. Programme the numbers into every household phone now, not later.
Brief everyone who looks after your pet. Dog walkers, family, pet-sitters and boarding kennels should have a copy of the plan and know the threshold line and where the rescue medicine is kept. The consensus is clear that at-home rescue treatment is only appropriate for caregivers who've actually been shown how, with the more involved routes reserved for "medically-trained" caregivers (Charalambous et al., 2024), so your plan should name who is authorised to give what. Not everyone holding it will be able to give the medicine, and that's fine: it still tells them when to call and where to go.
Don't stop or reduce the daily medication to "save it" or because things have been calm. Abruptly stopping an anti-seizure drug can itself trigger cluster seizures or status epilepticus, the very emergency the plan is for. If a drug is ever changed, it's tapered slowly, by about 20% or less per month, and only on your vet's instruction (Bhatti et al., 2015). Rock-steady daily dosing is your first line of defence against ever needing the rescue step, and the day-to-day of getting it in reliably lives in giving medication reliably.
Log every event. Record the date, time, duration, whether you gave the rescue dose and when, and how the recovery went. This tells your vet whether the plan is working and whether the daily treatment needs changing. It matters more than owners realise: a documented cluster or episode of status epilepticus is itself a recognised reason to start or step up long-term treatment (Bhatti et al., 2015), so every logged emergency also helps prevent the next one. The Seizure Diary is where the plan and its events live, and its emergency flag mirrors the same threshold line. The steps for the seizure itself, clearing hazards, not touching the mouth, noting the time, filming if it's safe, belong to seizure first aid.
A note for cat owners
The same plan structure and the very same emergency thresholds apply to cats, so everything above stands. The one caveat is that the rescue-medication options a vet might set for a cat rest on weaker evidence than in dogs: the consensus grades the at-home options for cats at its lowest confidence level (Charalambous et al., 2024). All the more reason the rescue step on a cat's plan must come from your vet and no one else.
There's also one feline-specific prevention line worth writing in, because it's the most useful thing a cat owner can do. Never apply a dog flea "spot-on" to a cat, and keep treated dogs apart from your cat until the product is fully dry. Permethrin poisoning, almost always a dog product used on a cat, is one of the most common toxic causes of feline death, triggering tremors in the great majority of cats and seizures in around a third (Boland & Angles, 2010). It's an emergency in its own right. This is a reactive cause, not epilepsy, and the detail belongs to what causes seizures in cats, but on a prevention plan it earns one firm line: don't do this, and if it happens, go straight in.
What "ready" actually looks like
You'll know the plan is doing its job when it has become boring: in date, in every phone, a route you've driven, a copy at the kennels. On the worst night you don't have to be brilliant or quick-thinking, you just read the page and do the next thing on it.
So sit down with your vet, fill in the rescue-medication box and the "leave now" trigger in their words, then print the plan for the fridge. Set up the Seizure Diary so it's ready to capture the next event and flag an emergency the moment one starts. The hope is that you never need any of it. The reassurance is that if you do, the remembering is already done.
References
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Mandigers, P. J. M., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Boland, L. A., & Angles, J. M. (2010). Feline permethrin toxicity: retrospective study of 42 cases. Journal of Feline Medicine and Surgery, 12(2), 61-71.
- Charalambous, M., Muñana, K., Patterson, E. E., Platt, S. R., & Volk, H. A. (2024). ACVIM Consensus Statement on the management of status epilepticus and cluster seizures in dogs and cats. Journal of Veterinary Internal Medicine, 38(1), 19-40.
- Charalambous, M., Volk, H. A., Van Ham, L., & Bhatti, S. F. M. (2021). First-line management of canine status epilepticus at home and in hospital: opportunities and limitations of the various administration routes of benzodiazepines. BMC Veterinary Research, 17, 103.
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Matiasek, K., Packer, R., Patterson, E., Pakozdy, A., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. (2015). International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine