
Managing Cluster Seizures at Home: Rescue Medication
Dr. Alastair Greenway
MRCVS
Cluster seizures have a cruelty of their own. The seizure in front of you is only half of it; the other half is knowing another may follow within hours, and waiting for it. If your vet has handed you a rescue kit, or has started talking about one, this article turns that waiting into a plan you can actually carry out.
Here is what this piece does, and what it doesn't. It teaches you how to use the rescue medication your vet has prescribed: how it works, how to give it calmly, what to expect afterwards, and the firm line where home care stops and the emergency clinic begins. It does not teach you to build your own protocol, change a dose, or pick a drug, because those are your vet's decisions, made for your individual pet. Recognising the emergency itself, the thresholds that mean "go now", is covered in is this an emergency? status epilepticus and cluster seizures, and the personalised written plan you'll keep with the kit lives in your status epilepticus emergency plan.
What a cluster is, and why a home plan helps
A cluster is two or more seizures within a 24-hour period, with your pet regaining consciousness between them (Charalambous et al., 2024). That recovery in between is what separates a cluster from status epilepticus, which is a single seizure lasting more than five minutes, or seizures running into one another with no recovery at all (Charalambous et al., 2024). The emergency article holds the full detail on those lines, but they're the spine of everything below.
Clusters matter because they're both common and serious. In one large study of dogs with idiopathic epilepsy, 41% (169 of 407) experienced cluster seizures, and dogs with frequent clusters were significantly more likely to be put to sleep because of them (Monteiro et al., 2012). That's the real reason this gets its own plan: clusters are linked to a lower chance of seizure freedom and a shorter survival, and they often arise in epilepsy that's harder to control, the subject of drug-resistant (refractory) epilepsy explained. A home protocol is how owners take back some control.
The same logic sits behind rescue medication. The expert consensus panel notes that high-frequency clusters can pose a risk similar to status epilepticus and are "unlikely to cease or be appropriately controlled without rescue medication" (Charalambous et al., 2024). Catching a cluster early, at home, can stop it escalating, and the original work on home rescue medication showed it could reduce the total number of cluster-seizure events a dog suffered (Podell, 1995). The kit on your shelf is there to break the cycle before it gathers pace, and to keep you out of the emergency clinic when it works.
The rescue options your vet may use
The two main owner-given options are both benzodiazepines: intranasal midazolam and rectal diazepam. There's also an emerging option, rectal levetiracetam, and a related oral strategy I'll come to. Which one you've been given depends on your pet and your vet's judgement, and whatever you've been prescribed, the dose and the rules are your vet's, not something to read off a webpage.
Intranasal midazolam is the preferred home rescue in dogs, and the evidence is clear about why. In a randomised trial it stopped status epilepticus in 70% of dogs (14 of 20), against just 20% (3 of 15) for rectal diazepam, and the authors concluded it was a quick, safe and effective first-line medication superior to rectal diazepam (Charalambous et al., 2017). Owner experience backs this up: in a survey, intranasal midazolam had a reported success rate of 97% versus 63% for rectal diazepam, with better compliance (95% versus 66%) and owners finding it easier to give (Kähn et al., 2023). The dose used in the trials and quoted in UK clinical references is 0.2 mg/kg (Charalambous et al., 2019; Royaux, 2024).
You give it with a small mucosal atomisation device that fits onto the syringe and turns the liquid into a fine mist for fast absorption across the lining of the nose; that device was used in around 89% of intranasal administrations in the owner study (Kähn et al., 2023). The one real drawback is a few more preparation steps than the rectal route, drawing the drug up and fitting the atomiser, which is why you should practise it before you ever need it in a crisis.
Rectal diazepam is the long-standing fallback. The original home protocol used 0.5 mg/kg of the injectable solution per rectum and significantly reduced the number of seizure events in treated dogs (Podell, 1995); reported effective doses across studies range from 0.5 to 2.0 mg/kg (Platt, 2020). One detail explains why your vet's dose might look higher than a friend's: in dogs on long-term phenobarbital the diazepam dose is commonly increased, often to 2 mg/kg, because phenobarbital speeds up how the liver clears diazepam and lowers its blood levels, a real effect measured directly in dogs (Wagner et al., 1998). Rectal diazepam still has a place when intranasal midazolam isn't available, though it's "unlikely to be as potent or fast acting" (Charalambous et al., 2024).
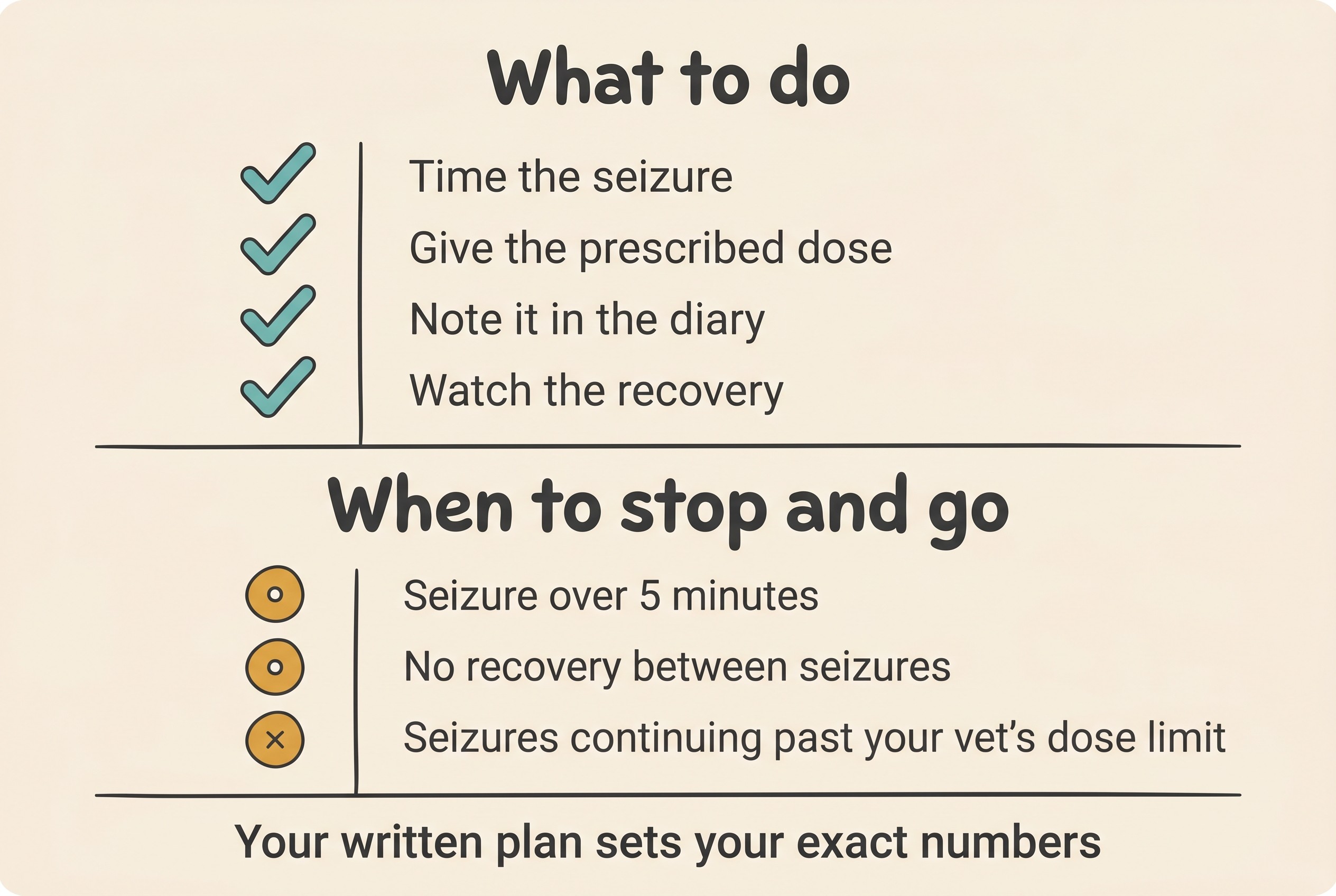
Repeat dosing and the line where home care ends. Rescue doses can generally be repeated up to three times within 24 hours, waiting around two minutes between boluses (Royaux, 2024). After that, or if seizures keep coming despite the doses your vet authorised, the next step is veterinary care, typically an intravenous infusion you can't give at home (Charalambous et al., 2024; Royaux, 2024). The principle to hold onto is that rescue medication exists to break a cluster early, not to manage an indefinite siege. If a seizure doesn't stop, if seizures keep recurring past the doses your vet set, if any single seizure lasts more than five minutes, or if your pet doesn't recover between them, that's the emergency clinic, now. Your exact dose limit and threshold come from your individual written plan, the document to fill in with your vet and keep beside the kit.
Giving rescue meds safely
It all comes down to a handful of calm habits.
Give exactly to the written protocol. Your vet's drug, dose, route, maximum number of doses, and "go to the clinic at this point" line. Never guess or scale a dose up because the seizure looks bad.
Practise before you need it. Rehearse the sequence with your vet or nurse when nobody is in crisis, so your hands already know how to fit the atomiser or give the rectal dose, time a seizure, and recognise "recovered between seizures" in your own pet.
Know what's normal afterwards. Marked sleepiness and wobbliness are expected and are not the same as an overdose. In the trial comparing intranasal and intravenous midazolam, severe sedation or ataxia occurred in 88% of the intranasal dogs with no serious adverse events (Charalambous et al., 2019). A drowsy, unsteady dog after a rescue dose is usually just the drug doing its job, so expect it and don't let it alarm you, though do ring your vet if you're unsure.
Look after the kit. Keep it somewhere everyone knows, check the expiry dates, replace anything you use, and train everyone who looks after your pet, from family to the dog-walker and boarding kennel. Keep the written plan with the kit so the steps are there even when panic erases your memory.
Record every use in the diary. Log the date and time, which seizure in the cluster it was, the dose you gave, and how your pet responded, in the Seizure Diary. This isn't box-ticking: it's what tells your vet whether the protocol is working and whether the daily maintenance medication needs adjusting. Filming the event and logging it remain the two most useful things you can do.
Cats cluster too
Cats have clusters as well, and the same emergency lines apply. The evidence for owner-given rescue medication in cats is thinner than in dogs, so the consensus panel withholds a formal recommendation for both intranasal midazolam and rectal diazepam in cats, while still citing the 0.2 mg/kg midazolam dose (Charalambous et al., 2024).
One point reassures many cat owners. You may have read that diazepam causes fatal liver damage in cats, but that risk is linked to the oral tablet form given repeatedly, and has not been reported with a single emergency injectable or rescue dose, so a rescue dose should not be withheld from a cat in crisis (Royaux, 2024). For longer-acting oral benzodiazepine pulses the panel does flag liver toxicity as a specific feline concern (Charalambous et al., 2024). As always, follow your vet's plan. Two maintenance-drug facts are worth remembering, both covered in the anti-seizure drugs compared: potassium bromide is contraindicated in cats, and imepitoin is not licensed for cats.
The rules that never bend
Whatever shape the night takes, a few things stay fixed. Rescue medication is always vet-prescribed and vet-dosed; this article helps you use a plan, not invent one. Never stop or abruptly reduce the daily maintenance medication, because sudden withdrawal can itself trigger clusters or status; any reduction is gradual, no more than around 20% a month, and only with your vet (Bhatti et al., 2015). Never put anything in the mouth of an actively seizing pet. And rescue drugs buy time, they don't replace the emergency clinic once the thresholds are crossed.
If your vet has given you a kit, you're already ahead. Make it second nature: rehearse the steps until your hands know them, write your thresholds into your status epilepticus emergency plan, and log every event and dose in the Seizure Diary. A plan you've practised, kept in date and shared with everyone who loves your pet turns the dread of the next cluster into something you can meet steadily, one calm step at a time.
References
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Cagnotti, G., Odore, R., Bertone, I., Corona, C., Dappiano, E., Gardini, G., Iulini, B., Bellino, C., & D'Angelo, A. (2019). Open-label clinical trial of rectally administered levetiracetam as supplemental treatment in dogs with cluster seizures. Journal of Veterinary Internal Medicine, 33(4), 1714-1718.
- Charalambous, M., Bhatti, S. F. M., Van Ham, L., Platt, S., Jeffery, N. D., Tipold, A., Siedenburg, J., Volk, H. A., Hasegawa, D., Gallucci, A., Gandini, G., Musteata, M., Flegel, T., Berendt, M., & De Risio, L. (2017). Intranasal midazolam versus rectal diazepam for the management of canine status epilepticus: a multicenter randomized parallel-group clinical trial. Journal of Veterinary Internal Medicine, 31(4), 1149-1158.
- Charalambous, M., Volk, H. A., Tipold, A., Erath, J., Huenerfauth, E., Gallucci, A., Gandini, G., Hasegawa, D., Pancotto, T., Rossmeisl, J. H., Platt, S., De Risio, L., & Bhatti, S. F. M. (2019). Comparison of intranasal versus intravenous midazolam for management of status epilepticus in dogs: a multicenter randomized parallel group clinical study. Journal of Veterinary Internal Medicine, 33(6), 2709-2717.
- Charalambous, M., Muñana, K., Patterson, E. E., Platt, S. R., & Volk, H. A. (2024). ACVIM consensus statement on the management of status epilepticus and cluster seizures in dogs and cats. Journal of Veterinary Internal Medicine, 38(1), 19-40.
- Kähn, C., Bhatti, S. F. M., Meller, S., Meyerhoff, N., Volk, H. A., & Charalambous, M. (2023). Out-of-hospital rescue medication in dogs with emergency seizure disorders: an owner perspective. Frontiers in Veterinary Science, 10, 1278618.
- Monteiro, R., Adams, V., Keys, D., & Platt, S. R. (2012). Canine idiopathic epilepsy: prevalence, risk factors and outcome associated with cluster seizures and status epilepticus. Journal of Small Animal Practice, 53(9), 526-530.
- Packer, R. M. A., Nye, G., Porter, S. E., & Volk, H. A. (2015). Assessment into the usage and side effects of phenobarbital and levetiracetam in a canine epilepsy clinic. BMC Veterinary Research, 11, 25.
- Platt, S. (2020). Status epilepticus and cluster seizures in dogs and cats. Improve Veterinary Education Clinical Library.
- Podell, M. (1995). The use of diazepam per rectum at home for the acute management of cluster seizures in dogs. Journal of Veterinary Internal Medicine, 9(2), 68-74.
- Royaux, E. (2024). Management of status epilepticus and cluster seizures (in dogs and cats). Improve Veterinary Education Clinical Library.
- Wagner, S. O., Sams, R. A., & Podell, M. (1998). Chronic phenobarbital therapy reduces plasma benzodiazepine concentrations after intravenous and rectal administration of diazepam in the dog. Journal of Veterinary Pharmacology and Therapeutics, 21(5), 335-341.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine