Drug-Resistant (Refractory) Epilepsy Explained
Claire Greenway
MRCVS
You give the tablets on time. You've sat through the blood tests, watched the dose creep up, and still, every few weeks, your dog goes down again. Then a vet uses a word that sounds like a door closing: refractory. Drug-resistant. And underneath every other worry sits the frightening one: have we run out of options?
The plain answer is no. Refractory does not mean untreatable, and it is not the end of the road. It means the disease in front of you is one of the harder ones to suppress, and the plan now changes shape. It stops being "find the right dose of the right drug" and becomes something more structured and patient. This article is about what that word actually means, why some epilepsy behaves this way, and the single most useful thing to do before you accept the label at all. The specific next treatments live in their own guides, linked as we go.
What "drug-resistant" actually means
The word gets used loosely, so it's worth pinning down. The International Veterinary Epilepsy Task Force, the consensus group whose work underpins how most vets approach this disease, defines drug-resistant epilepsy as the failure of adequate trials of two tolerated, appropriately chosen and properly used anti-seizure drug schedules, whether given alone or in combination, to achieve sustained freedom from seizures (Potschka et al., 2015). Two words in that sentence carry most of the weight.
The first is adequate. A drug only counts as a failed trial if it was actually given a fair chance: the right dose, kept up long enough to reach steady state in the bloodstream, with serum levels checked where that drug needs checking (Potschka et al., 2015; Bhatti et al., 2015). A low dose that never reached a therapeutic level hasn't failed; it was never really tested. The second is tolerated. If a drug was stopped only because the side effects were unbearable, not because it failed to control the seizures, that doesn't count as drug resistance either (Potschka et al., 2015; Bhatti et al., 2015). It might have worked beautifully at a dose your dog simply couldn't live with, a different problem with different answers.
The task force also encourages vets to be specific, to say "phenobarbital-resistant" or "bromide-resistant" rather than just "resistant", because which drugs your dog has genuinely failed shapes what's tried next (Potschka et al., 2015).
How common refractory epilepsy really is
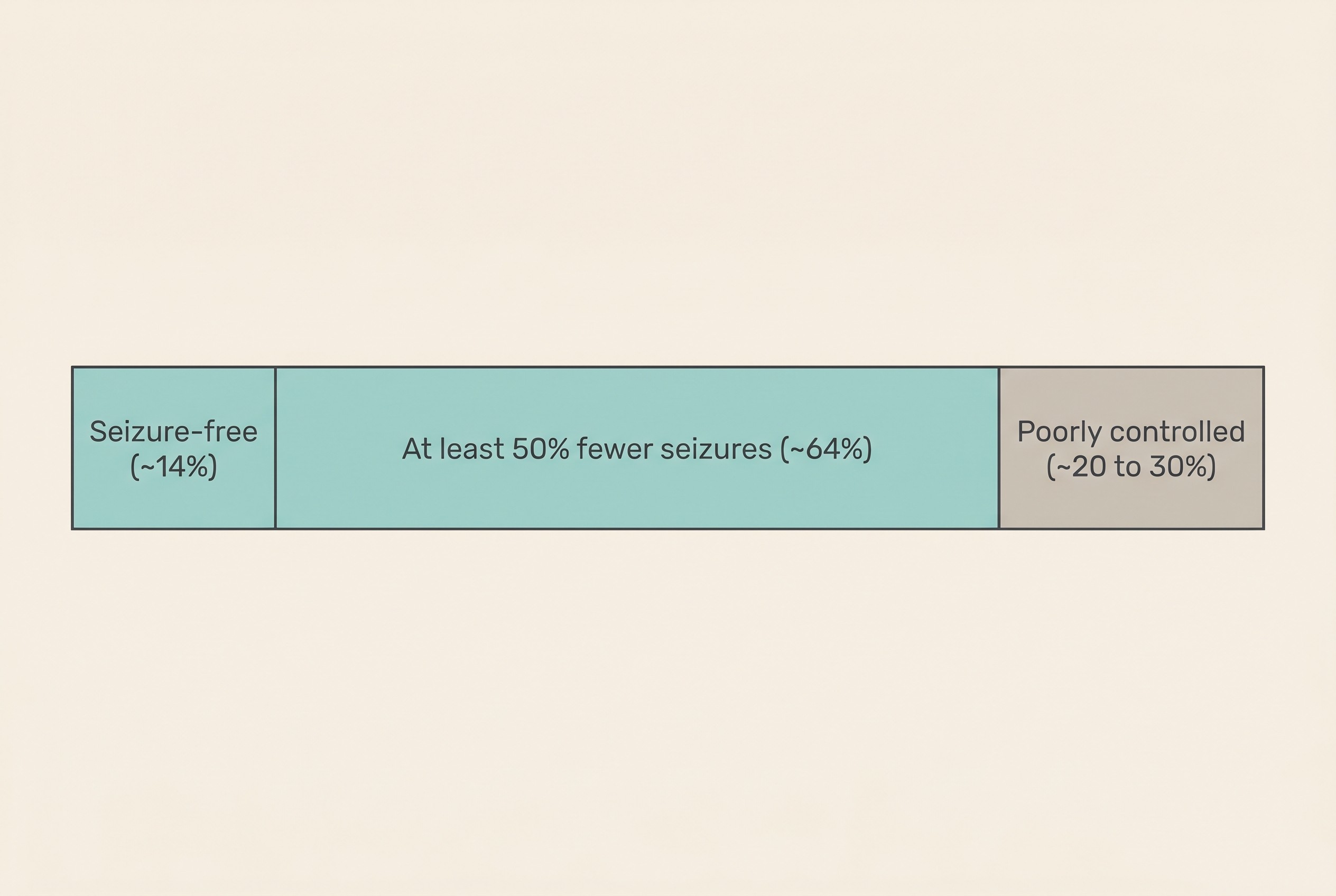
Owners are often told their dog is unlucky, as though refractory epilepsy were rare. It isn't, and there's some cold comfort in that. Roughly a quarter to a third of dogs with idiopathic epilepsy remain poorly controlled despite treatment, around 20 to 30% still seizing more than we'd like (less than a 50% reduction) despite phenobarbital, potassium bromide, or both (Kajin et al., 2023; Packer et al., 2014).
It also helps to be clear about what "success" usually looks like, because the bar is lower than most people assume. In one large referral population of treated dogs, only about 14% became completely seizure-free, while around 64.5% achieved at least a halving of their seizure frequency (Packer et al., 2014); the task force's outcome review similarly puts drug-induced remission of one to three years at only 15 to 24% of dogs (Potschka et al., 2015). Complete freedom from seizures was always the exception, not the expectation.
This isn't a dog-only problem either. Cats treated for suspected primary epilepsy show strikingly similar proportions, with roughly 30% poorly controlled on phenobarbital (Pakozdy et al., 2013), so there's nothing aberrant about being in that minority whichever animal you're caring for.
Why some epilepsy resists treatment
This is the question that keeps owners awake, and the truthful answer is that we don't fully know, and we can't know which mechanism is at play in your individual dog. There are two leading theories, not mutually exclusive, and neither proven in any single patient (Potschka et al., 2015).
The first is the transporter hypothesis: the brain over-produces tiny molecular pumps at the blood-brain barrier, especially one called P-glycoprotein (made by the ABCB1, also written MDR1, gene), which push the anti-seizure drug back out before it reaches the misfiring tissue, so the brain sees far less drug than the bloodstream suggests (Potschka et al., 2015). The second is the target hypothesis: disease-driven or inherited changes alter the drug's actual targets in the affected brain, so even when the drug arrives, the lock it's meant to turn no longer responds to the key (Potschka et al., 2015).
On the genetics, I have to be straighter than most websites are willing to be. The evidence in dogs is early and contradictory. One study in Border Collies linked a particular ABCB1 variant to phenobarbital-resistant epilepsy (Mizukami et al., 2013). But a separate study in Collies found the opposite of what the transporter theory predicts: dogs carrying the well-known MDR1 mutation actually had better seizure control, which the authors put down to differences in intrinsic seizure severity rather than drug pumps (Muñana et al., 2012). So be wary of any genetic test that promises to tell you why your dog is resistant. The science isn't there yet.
Refractory epilepsy is best understood as the underlying brain disorder simply being more severe and harder to suppress in some individuals, the way some asthma is mild and some is brittle. It is not a sign that you dosed wrong or your vet chose badly (Muñana et al., 2012).
First, re-check the basics: the "false" refractory
Before you accept the label at all, there is one step that matters more than any other. A surprising number of dogs that look drug-resistant are not. The term for this is pseudoresistance: epilepsy that appears refractory but is really something fixable wearing a refractory costume.
The scale of it is striking. In a study of 152 dogs referred to a specialist as medication-resistant, 27% turned out to be pseudoresistant rather than truly resistant: more than a quarter of "we've run out of options" dogs still had straightforward options left (Kajin et al., 2023). And the reasons were exactly the unglamorous, fixable things you'd hope for: serum drug levels simply too low (42%, the commonest culprit), an inappropriate drug or dose choice (22%), the seizure type misclassified (22%), a wrong diagnosis where the pet didn't actually have epilepsy at all (9%), and poor compliance with the medication (9%) (Kajin et al., 2023).
So before "refractory" sticks, this is the checklist a good vet works through, and one you can think about alongside them (Kajin et al., 2023; Bhatti et al., 2015):
- Is the diagnosis right? Are these definitely epileptic seizures from a primary brain disorder, and not something else mimicking them?
- Is the dose genuinely adequate, and have blood levels been confirmed at steady state? The dose on the box and the level in the blood are not the same thing, because every animal metabolises differently.
- Is the medication actually getting in, on time, every single time? Missed or late doses, a pill spat out unnoticed, a tablet hidden in food that gets left.
- Has anything diluted the level? Weight gain, a drug interaction, a change of product or formulation.
- Are obvious triggers being managed? Disrupted sleep, missed meds, the avoidable destabilisers.
Sorting these out resolves a meaningful share of apparently refractory cases (Kajin et al., 2023). This is precisely where a reliable record earns its keep, because frequency is both the number your vet doses against and how the re-check is judged. If you're not already keeping one, the Seizure Diary is built to capture exactly this (Bhatti et al., 2015).
What "harder to control" does, and doesn't, mean
Once true drug resistance is confirmed, the question turns to outlook, and here I want to hold two plain truths at once: this is serious, and it is far from hopeless.
Start with the reassurance, because it's real. Refractory triggers a different, structured pathway rather than a dead end: re-check the basics, then add-on and third-line drugs, rescue protocols for clusters, specialist referral, and dietary approaches (all linked at the end). The goal also stays what it always was: reduction, not cure. The task force frames the realistic aim as decreasing the frequency, duration and severity of seizures with no or only limited and acceptable side effects, and a "responder" is usually a dog achieving at least a 50% reduction in seizure frequency (Bhatti et al., 2015). Halving the seizures is a genuine win, not a failure to reach zero.
Now the harder part. Some patterns do predict a more difficult road. Dogs with a history of cluster seizures, and male dogs, are significantly less likely to reach remission: in one study, dogs with no prior cluster seizures were around six times more likely to remit, and females around twice as likely (Packer et al., 2014). Tellingly, it's the pattern and density of seizures, the tendency to come in clusters, that predicts resistance more than the raw headline frequency, which is why the diary's job isn't only to count but to show the shape (Packer et al., 2014).
Why does getting on top of this matter so much? Dogs with idiopathic epilepsy have a near-normal median lifespan, around 9.2 years, against about 5.8 years for dogs whose seizures come from structural brain disease (Berendt et al., 2007). Well managed, the disease itself is compatible with a good, long life. But poorly controlled seizures carry real risk: status epilepticus, the prolonged seizure emergency, is associated with shorter survival, a mean lifespan of 8.3 years against 11.3 years in dogs that never had it (Saito et al., 2001), and most epilepsy-related deaths are not the seizures themselves but euthanasia chosen when seizures can no longer be controlled (Berendt et al., 2007). That's exactly why the emergency line and a rescue plan exist: they're the safety net that buys the good years.
So keep this line somewhere you can find it at 2am. A seizure lasting more than five minutes, or two or more seizures in 24 hours, or seizures running into one another without a real recovery in between, is an emergency: vet or emergency clinic, now (De Risio et al., 2015; Bhatti et al., 2015). A single short seizure your dog recovers from is frightening but not, by itself, an emergency. For refractory dogs especially, an at-home rescue plan agreed in advance is one of the most protective things you can do, covered in managing cluster seizures at home.
A note for cat owners
For a cat, the concept is the same but the rulebook is not, and getting the drugs wrong here can be fatal. Potassium bromide is contraindicated in cats. Roughly 40% of cats given it develop moderate-to-severe lower-airway disease, an asthma-like inflammation of the lungs that has proved fatal in some (Boothe et al., 2002; Bertolani et al., 2012), so it should never be offered as a feline option. Imepitoin is not licensed for cats either. The feline approach is phenobarbital first, with levetiracetam as the usual add-on, though the cat evidence for it is thin: the main supporting study was a small open-label one of 12 poorly-controlled cats, more than half of which achieved a greater than 50% reduction in seizures and tolerated it well (Bailey et al., 2008; Pakozdy et al., 2013). A reasonable next step, just not a guarantee.
What never changes, whatever comes next
Whatever the next move is, adding a drug, switching one, trying a diet, one rule holds without exception: never stop an anti-seizure medication abruptly. Sudden withdrawal can itself trigger a cluster or status epilepticus. If a drug ever does need to come out, it's tapered slowly, by around 20% or less per month, and only ever under your vet's direction (Bhatti et al., 2015). This applies even when a drug seems to be doing nothing; "nothing" abruptly removed can still provoke a crisis.
The path from here is genuinely a path, not a cliff edge. The add-on and third-line drugs your specialist can layer in are covered in advanced and add-on treatment options. Using rescue medication safely at home, so a cluster doesn't become an emergency dash every time, is in managing cluster seizures at home. And if you reach the harder questions about your pet's day-to-day happiness, quality of life and difficult decisions is written gently, for exactly that. None is a step you have to take today. They're proof that the door "refractory" seemed to close is, in fact, several doors still open. Your job right now is the unglamorous, powerful one: keep the diary, give the meds on time, and walk this next stretch with your vet rather than the internet.
References
- Bailey, K. S., Dewey, C. W., Boothe, D. M., Barone, G., & Kortz, G. D. (2008). Levetiracetam as an adjunct to phenobarbital treatment in cats with suspected idiopathic epilepsy. Journal of the American Veterinary Medical Association, 232(6), 867-872.
- Berendt, M., Gredal, H., Ersbøll, A. K., & Alving, J. (2007). Premature death, risk factors, and life patterns in dogs with epilepsy. Journal of Veterinary Internal Medicine, 21(4), 754-759.
- Bertolani, C., Hernandez, J., Gomes, E., Cauzinille, L., Poujade, A., & Gabriel, A. (2012). Bromide-associated lower airway disease: a retrospective study of seven cats. Journal of Feline Medicine and Surgery, 14(8), 573-577.
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Boothe, D. M., George, K. L., & Couch, P. (2002). Disposition and clinical use of bromide in cats. Journal of the American Veterinary Medical Association, 221(8), 1131-1135.
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Mandigers, P. J. J., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- Kajin, F., Meyerhoff, N., Charalambous, M., & Volk, H. A. (2023). "Resistance is futile": a pilot study into pseudoresistance in canine epilepsy. Animals, 13(19), 3125.
- Mizukami, K., Yabuki, A., Kohyama, M., Kushida, K., Rahman, M. M., Kim, S., Sasaki, F., & Yamato, O. (2013). High frequency of a single nucleotide substitution (c.-6-180T>G) of the canine MDR1/ABCB1 gene associated with phenobarbital-resistant idiopathic epilepsy in Border Collie dogs. Disease Markers, 2013, 695918.
- Muñana, K. R., Nettifee-Osborne, J. A., Bergman, R. L. Jr., & Mealey, K. L. (2012). Association between ABCB1 genotype and seizure outcome in Collies with epilepsy. Journal of Veterinary Internal Medicine, 26(6), 1358-1364.
- Packer, R. M. A., Shihab, N. K., Torres, B. B. J., & Volk, H. A. (2014). Clinical risk factors associated with anti-epileptic drug responsiveness in canine epilepsy. PLoS ONE, 9(8), e106026.
- Pakozdy, A., Sarchahi, A. A., Leschnik, M., Tichy, A. G., Halasz, P., & Thalhammer, J. G. (2013). Treatment and long-term follow-up of cats with suspected primary epilepsy. Journal of Feline Medicine and Surgery, 15(4), 267-273.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Cizinauskas, S., Farquhar, R., Jokinen, T. S., Long, S., Mandigers, P. J. J., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V. M., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
- Saito, M., Muñana, K. R., Sharp, N. J. H., & Olby, N. J. (2001). Risk factors for development of status epilepticus in dogs with idiopathic epilepsy and effects of status epilepticus on outcome and survival time: 32 cases (1990-1996). Journal of the American Veterinary Medical Association, 219(5), 618-623.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine