
Advanced and Add-On Treatment Options
Dr. Alastair Greenway
MRCVS
By the time an owner reaches this point, the harder parts are usually behind them. Your dog has been on treatment for a while, the first add-on has been tried, and the seizures still keep coming. So let me be straight: yes, there are more options, and many of them help. But there's no hidden cure waiting at the end of the queue, and I'd rather say that plainly than let a single line on this page raise a hope I can't support.
This article is for dogs whose seizures persist despite two appropriately chosen drugs given at adequate doses, with the levels checked. That's the formal definition of drug-resistant epilepsy: failure of adequate trials of two tolerated, appropriately chosen and used drug schedules, whether on their own or together, to achieve sustained seizure freedom (Potschka et al., 2015). What "refractory" means, why some epilepsy resists drugs and how common it is all belong to drug-resistant epilepsy explained. This piece picks up afterwards, at the practical question: what now?
Hold onto one thing first. Adding a third or fourth drug means layering it onto what your dog already takes, not swapping it in. You never stop or abruptly cut a current anti-seizure drug to "make room" for a new one: sudden withdrawal can trigger a cluster of seizures or even status epilepticus, the very emergencies you're trying to prevent (Bhatti et al., 2015). Every change here is made gradually, by your vet or neurologist, with the existing regimen kept stable underneath.
Third- and fourth-line drugs
Here's how specialists tend to layer the additional drugs: what each does, what the studies showed, and where it falls short.
Levetiracetam (Keppra) is the best-supported of the lot, which is why I'm starting here. It works differently from the older drugs, binding a protein called SV2A on the nerve endings and dialling down the release of the chemicals that fire seizures (Bhatti et al., 2015). The numbers are encouraging: in dogs already pharmacoresistant on phenobarbital plus bromide, 8 of 14 dogs evaluated were responders at two months, with seizure frequency falling by about 77% on average, and it was very well tolerated, with sedation in only one dog (Volk et al., 2008). But there's an important catch, often called the honeymoon effect: in that same study, 6 of the 9 dogs that initially responded drifted back towards their old seizure frequency after four to eight months of continuous use, a recognised tolerance phenomenon (Volk et al., 2008). One practical wrinkle too: phenobarbital speeds up the clearance of levetiracetam, so when the two are given together the dose often needs to be higher (Bhatti et al., 2015). Giving levetiracetam in bursts to sidestep the honeymoon effect and cover clusters is pulse dosing, and it belongs to managing cluster seizures at home.
Zonisamide is a sulphonamide-based drug that works on several fronts at once: blocking sodium and calcium channels, boosting the calming neurotransmitter GABA, and reducing the excitatory one, glutamate (Bhatti et al., 2015). Two open-label studies give the practical picture. In one, 7 of 12 refractory dogs achieved at least a 50% reduction in seizures (Dewey et al., 2004), and in another, 9 of 11 did, with some dogs able to reduce their phenobarbital afterwards (von Klopmann et al., 2007). The common side effects are sedation, wobbliness, a reduced appetite and vomiting, with rare but serious idiosyncratic risks to the liver and kidneys (Bhatti et al., 2015). Despite those encouraging response rates, the formal verdict remains insufficient evidence, for want of controlled trials (Bhatti et al., 2015).
Gabapentin binds a modulatory part of the voltage-gated calcium channels, reducing the release of excitatory neurotransmitters. Its short half-life means giving it several times a day to keep levels steady (Bhatti et al., 2015). The add-on evidence is modest: in one case series, 6 of 11 refractory dogs achieved at least a 50% reduction (Platt et al., 2006), and a separate series also reported a benefit (Govendir et al., 2005). The main downsides are sedation and wobbliness. Verdict: insufficient evidence (Bhatti et al., 2015; Charalambous et al., 2014).
Pregabalin is a close relative of gabapentin, more potent because it grips its target more tightly. It's been studied as an add-on in dogs already on phenobarbital with or without bromide, with sedation, wobbliness and weakness the side effects to watch for. Verdict, again: insufficient evidence (Dewey et al., 2009).
Topiramate has several mechanisms rolled into one, boosting GABA, blocking sodium and calcium channels, and inhibiting an enzyme called carbonic anhydrase (Bhatti et al., 2015). As an add-on in 10 refractory dogs, 5 of the 10 responded, with a meaningful drop in seizure frequency of around 66% over six months, and the side effects, weight loss, sedation and wobbliness, often eased off with time (Kiviranta et al., 2013). Verdict: insufficient evidence (Kiviranta et al., 2013).
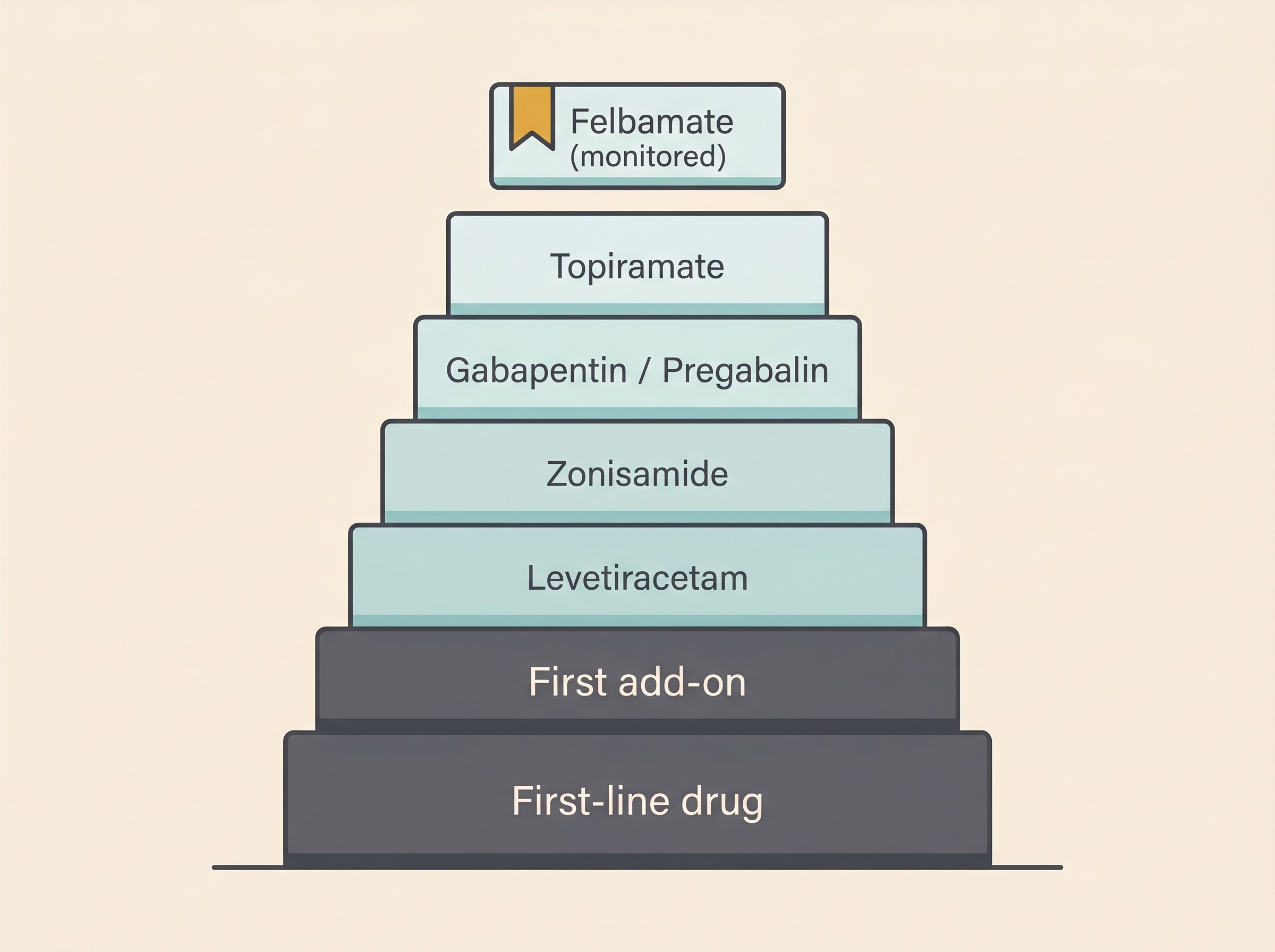
Felbamate sits apart as a reserve drug rather than a routine next step. It works partly through the NMDA-glycine site and partly on sodium and calcium channels, and it can be effective: in one small series, all 6 dogs improved and 2 became seizure-free (Bhatti et al., 2015; Ruehlmann et al., 2001). What holds it back is safety. Felbamate carries the serious toxicity flags that ended its routine use in human medicine: aplastic anaemia, potentially fatal liver damage, dry eye (keratoconjunctivitis sicca) and blood disorders (Bhatti et al., 2015; Ruehlmann et al., 2001). The Task Force is explicit that it should be reserved for dogs that have failed the other, better-studied and safer drugs, and it needs frequent blood and liver monitoring, monthly for the first six to twelve months (Bhatti et al., 2015). A real option, then, but a carefully watched one.
Living with polypharmacy
One thread runs through all of this. Most escalation in hard-to-control epilepsy is additive: a second and then sometimes a third drug stacked onto what your dog already takes, rather than a clean switch from one to another (Bhatti et al., 2015). The first time that decision comes up, add versus switch at first-line failure, is owned by when the first drug isn't enough. This article lives further down that road, at the second and third add-on.
And the trade-off sharpens with every drug you add. More agents can mean more seizure control, but they also tend to mean more sedation, more wobbliness, more hunger and weight gain, and more blood tests. A specialist's job at this stage isn't simply to keep adding drugs. It's to weigh each incremental gain against the cumulative cost in side effects and quality of life, and to know when the next drug would take more from your dog's daily life than it gives back (Bhatti et al., 2015; Potschka et al., 2015). That judgement is difficult and deeply individual, which is the strongest argument for having a specialist in your corner.
Where do surgery and devices fit?
This is where owners' hopes often turn, usually after reading about epilepsy surgery in people. So let me be plain: there is no routine epilepsy surgery in dogs or cats comparable to the resective surgery offered to some people. It isn't an everyday option in veterinary medicine.
Implanted devices are a more interesting story, but the fair summary is "promising and experimental", not "available and proven". Vagus nerve stimulation, where a small implanted device stimulates a nerve in the neck on a cycle, has been trialled in dogs. In a placebo-controlled crossover study of 10 dogs, there was no significant overall reduction across the 13-week treatment period, although a roughly 34% fall emerged in the final four weeks, and the authors concluded it was potentially safe and possibly helpful in certain dogs when drugs fail (Muñana et al., 2002). A newer, non-invasive version held against the neck has also been tested: in a feasibility study of 14 dogs, 9 showed some reduction but only 4 were true responders, with no statistically significant difference from the control condition. The authors called it a small feasibility study that needs larger trials (Robinson et al., 2020).
So the realistic bottom line: neurostimulation is promising but experimental and limited, available mainly through research projects or specialist centres rather than your local practice. The wider view of what's on the horizon, deep brain stimulation, responsive stimulation and novel drugs, deserves its own careful map in new and emerging treatments, realistically.
Non-drug adjuncts worth knowing about
Drugs and devices aren't the whole story, and two adjuncts are worth raising with your vet.
Start with diet. A diet supplemented with medium-chain triglycerides is a legitimate adjunct for some refractory dogs, used alongside medication rather than instead of it. What the trials showed, and what they didn't, is covered in diet and epilepsy, so I'll point you there rather than half-tell the story.
Then there's rescue medication at home. If your dog has clusters, there are protocols using rectal or intranasal medication, and levetiracetam given in bursts, that your vet can set up so you're not helpless at three in the morning. That's owned by managing cluster seizures at home. It's also the moment to be clear about what still counts as an emergency while you work through these options: a seizure lasting more than five minutes, two or more seizures in 24 hours, or seizures coming back to back without a full recovery between them all mean a vet or emergency clinic now. A single short seizure your dog recovers well from is not, by itself, an emergency.
You may also be wondering about CBD. The short version is that it's not a cure and not a substitute for prescribed anti-seizure drugs, it interacts with phenobarbital, and product quality varies a great deal. The full, cited picture lives in its own article, which is the better read than a rushed paragraph here.
Why a neurologist earns their place
You'll have noticed a pattern. Layering a third or fourth drug, interpreting blood levels as the picture grows more complex, weighing a device against more medication, knowing when to stop adding and start subtracting: this is specialist territory, where a neurologist adds value a general practice, however good, can struggle to match (Bhatti et al., 2015; De Risio et al., 2015). What a referral involves, what it costs and how care is shared afterwards is owned by seeing a neurologist.
Whatever you and your specialist try next, one thing stays constant. Every decision on this page, whether a new drug is genuinely helping or just adding side effects, is judged against your dog's seizure record: not a feeling, or a good week, or a bad one, but the logged frequency and severity over time. Keeping that record well, and bringing it to every appointment, turns a vague "I think he might be a bit better" into evidence your specialist can act on. The Seizure Diary is built for exactly this: log each event, watch the frequency line, and export it for your neurologist. As you work through the options here, the diary is what tells you which ones are earning their place.
References
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Charalambous, M., Brodbelt, D., & Volk, H. A. (2014). Treatment in canine epilepsy: a systematic review. BMC Veterinary Research, 10, 257.
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Mandigers, P. J. J., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- Dewey, C. W., Guiliano, R., Boothe, D. M., Berg, J. M., Kortz, G. D., Joseph, R. J., & Budsberg, S. C. (2004). Zonisamide therapy for refractory idiopathic epilepsy in dogs. Journal of the American Animal Hospital Association, 40(4), 285–291.
- Dewey, C. W., Cerda-Gonzalez, S., Levine, J. M., Badgley, B. L., Ducoté, J. M., Silver, G. M., Cooper, J. J., Packer, R. A., & Lavely, J. A. (2009). Pregabalin as an adjunct to phenobarbital, potassium bromide, or a combination of phenobarbital and potassium bromide for treatment of dogs with suspected idiopathic epilepsy. Journal of the American Veterinary Medical Association, 235(12), 1442–1449.
- Govendir, M., Perkins, M., & Malik, R. (2005). Improving seizure control in dogs with refractory epilepsy using gabapentin as an adjunctive agent. Australian Veterinary Journal, 83(10), 602–608.
- Kiviranta, A.-M., Laitinen-Vapaavuori, O., Hielm-Björkman, A., & Jokinen, T. (2013). Topiramate as an add-on antiepileptic drug in treating refractory canine idiopathic epilepsy. Journal of Small Animal Practice, 54(10), 512–520.
- Muñana, K. R., Vitek, S. M., Tarver, W. B., Saito, M., Skeen, T. M., Sharp, N. J. H., Olby, N. J., & Haglund, M. M. (2002). Use of vagal nerve stimulation as a treatment for refractory epilepsy in dogs. Journal of the American Veterinary Medical Association, 221(7), 977–983.
- Platt, S. R., Adams, V., Garosi, L. S., Abramson, C. J., Penderis, J., De Stefani, A., & Matiasek, L. (2006). Treatment with gabapentin of 11 dogs with refractory idiopathic epilepsy. Veterinary Record, 159(26), 881–884.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Farquhar, R., Long, S., Mandigers, P., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
- Robinson, K., Platt, S., Stewart, G., Reno, L., Barber, R., & Boozer, L. (2020). Feasibility of non-invasive vagus nerve stimulation (gammaCore VET™) for the treatment of refractory seizure activity in dogs. Frontiers in Veterinary Science, 7, 569739.
- Ruehlmann, D., Podell, M., & March, P. (2001). Treatment of partial seizures and seizure-like activity with felbamate in six dogs. Journal of Small Animal Practice, 42(8), 403–408.
- Volk, H. A., Matiasek, L. A., Luján Feliu-Pascual, A., Platt, S. R., & Chandler, K. E. (2008). The efficacy and tolerability of levetiracetam in pharmacoresistant epileptic dogs. The Veterinary Journal, 176(3), 310–319.
- von Klopmann, T., Rambeck, B., & Tipold, A. (2007). Prospective study of zonisamide therapy for refractory idiopathic epilepsy in dogs. Journal of Small Animal Practice, 48(3), 134–138.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine