
When the First Drug Isn't Enough: Adding On vs Switching
Claire Greenway
MRCVS
A meaningful minority of dogs keep seizing after the first anti-seizure drug is started and given faithfully, and that is a normal point on this journey rather than a dead end. If you've done it all by the book, given the medicine religiously and sat through the blood tests, and the seizures haven't stopped, it's easy to read that as failure. It isn't. Continuing seizures on a first drug is common and expected, and there's a clear next step.
This article is about one fork in the road: do you add a second drug on top of the first, or swap the first one out for something else? It covers only that first step. A third or fourth drug, surgery or devices lives in advanced add-on treatments, and what it means when seizures resist treatment long-term belongs to refractory epilepsy explained.
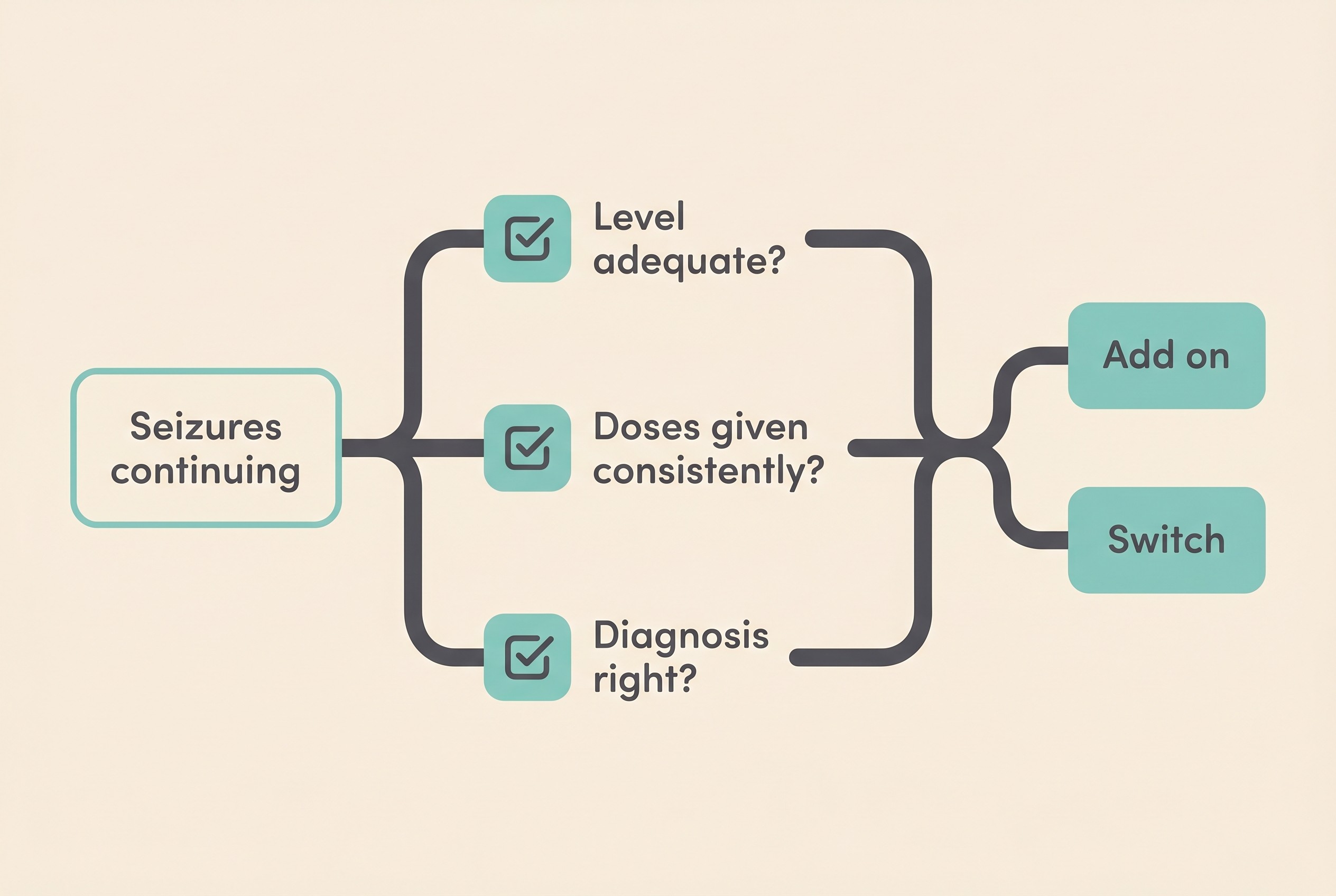
First, is it really not working?
Before anyone concludes a drug has failed, three things have to be confirmed, and this is the part most owners skip past: that the dose and blood level are genuinely adequate, that the medicine is actually getting into your dog consistently, and that the diagnosis is right in the first place. The epilepsy task force calls apparent failure caused by an inadequate dosing or treatment regime pseudoresistance, and is blunt about it: every drug trial must have been used at optimal doses before you can call it a failure (Potschka et al., 2015).
This isn't a technicality dreamed up by specialists. In a study of 152 dogs referred as medication-resistant, 27% of them, 41 dogs, weren't truly resistant at all. They were pseudoresistant, and all but one came under control once the protocol was corrected (Kajin et al., 2023). The commonest reasons were low serum drug levels (42% of cases), inadequate drug choice or dose (22%), misclassified seizures (22%) and outright misdiagnosis (9%) (Kajin et al., 2023).
So the first conversation isn't "what's the next drug", it's "are we sure the current one has had a fair go". Drawing a blood level sits in therapeutic drug monitoring; pushing the first drug to the top of its range lives in how dose titration works. One quiet word about numbers: if your dog is well controlled but the blood level reads a little below the textbook range, that doesn't automatically mean the dose needs to go up. That level may be enough for your individual dog, and the principle vets use is to treat the dog, not the number (Bhatti et al., 2015).
What "an adequate level" actually means
For phenobarbital, the therapeutic serum range runs from 15 to 40 mg/l, most dogs need around 25 to 30 mg/l for good control, and levels above 35 mg/l start to raise the risk of liver damage and are best avoided (Bhatti et al., 2015). That's why the rule is to use the blood level to guide dose increases before reaching for a second drug, not to leap straight to adding one (Bhatti et al., 2015).
It also helps to be clear about what "working" means, because the bar isn't zero. A "responder" is formally a dog with at least 50% fewer seizures, and that's the realistic target: complete freedom does happen but is uncommon, with reported remission in only 15 to 24% of dogs (Potschka et al., 2015; Bhatti et al., 2015). Fewer, shorter, less severe seizures is the pass mark.
Add on, or switch?
If the first drug is helping but not enough, the mainstream approach is to add a second rather than swap, after the first has been taken to the top of its range or the maximum your dog tolerates, so you keep the control it's already buying you (Bhatti et al., 2015). For a dog poorly controlled on phenobarbital alone, the task force specifically supports adding potassium bromide, and the same applies where the phenobarbital dose has to be pulled back because of side effects (Bhatti et al., 2015). For a dog on imepitoin (Pexion) still seizing at its maximum dose of 30 mg/kg twice daily, the recommendation is to add phenobarbital (Bhatti et al., 2015).
Switching makes most sense for a different reason: when the first drug isn't tolerated rather than simply not strong enough. If side effects are severe enough to force the drug out, you withdraw it and replace it (Bhatti et al., 2015). The rule of thumb, then, is to add on if the drug is working a bit but not enough, and switch if it's intolerable or never helped at all.
Now the safety line that overrides everything. You never stop an anti-seizure drug abruptly. If a drug is being withdrawn, the dose comes down by 20% or less per month, because a sudden stop can trigger withdrawal seizures or even status epilepticus (Bhatti et al., 2015). So a "switch" is never a clean overnight swap, it's a careful taper of one while the other comes on board. Please never skip or stop a dose yourself to "see if it's still needed", because that single decision is one of the ways a stable dog ends up in an emergency clinic.
The common second drugs
A handful of drugs usually come up as the second agent, and the evidence behind them varies. The per-drug detail and the dog-versus-cat split live in the drugs compared; here I'll stick to what they offer as an add-on.
Potassium bromide (KBr) is, in most of the UK and EU, licensed only as an add-on for dogs that haven't responded to first-line treatment, and it works synergistically with phenobarbital (Bhatti et al., 2015). The classic evidence is encouraging: adding bromide to dogs poorly controlled on phenobarbital reduced total seizures in 83% of them and rendered 26% seizure-free, and the phenobarbital dose could be cut in 35% (Podell & Fenner, 1993). Paired with phenobarbital, the target bromide level is around 1000 to 2000 mg/l (Bhatti et al., 2015). One practical catch: it's sensitive to how much salt is in the diet, since chloride intake shifts the blood level (Bhatti et al., 2015).
Levetiracetam (Keppra) is a popular, well-tolerated add-on. In a UK epilepsy clinic series, 69% of dogs were responders and 15% became seizure-free on it (Packer et al., 2015), and a systematic review graded its evidence as an adjunct as "fair", the best-supported of any add-on in that review (Charalambous et al., 2014). The counterweight: the single best-designed trial we have, a blinded, placebo-controlled, crossover study in dogs already resistant to phenobarbital and bromide, couldn't show levetiracetam beat placebo (seizures fell by 1.1 against 1.5 on placebo, not significant), although seizures did drop significantly from the dogs' own baseline while on it, and the study was underpowered with a notable placebo response (Muñana et al., 2012). So: widely used and often genuinely helpful in practice, but keep expectations realistic.
There's a second quirk, sometimes called the honeymoon effect. Some dogs respond beautifully at first then lose ground over weeks or months as tolerance builds, documented for both levetiracetam and zonisamide in dogs, and one reason vets sometimes use a pulse or interval dosing protocol (Packer et al., 2015; Bhatti et al., 2015).
After imepitoin specifically, there's direct evidence for what to add. A randomised trial in dogs still seizing on maximum imepitoin found responder rates of 79% when phenobarbital was added and 69% when bromide was, both significantly cutting seizures and generally well tolerated (Royaux et al., 2017). A separate study of imepitoin plus phenobarbital found 36 to 42% of dogs achieved at least a halving of seizures, but flagged an important limit: that combination did not suppress cluster seizures (Neßler et al., 2017). If clusters are part of your dog's pattern, raise it with your vet; the at-home side is covered in managing cluster seizures at home.
Setting your expectations for the next step
Expect waiting. Bromide has a long half-life, so you judge whether it's helping over weeks to months, not days, in a rhythm of recheck and adjust rather than an overnight fix (Bhatti et al., 2015).
This is where your seizure diary becomes the evidence the whole decision turns on. Your vet doses against frequency, so how often seizures came before a change versus after it is the single number that says whether the new drug is earning its place. Logging every event in the Seizure Diary, with dates, length and any missed doses, is the most useful thing you can do before the next recheck.
A note for cat owners
The trial evidence above is mostly canine, and the feline picture is genuinely different, so please don't transfer it across. In cats, first-line is phenobarbital and the recognised second drug is levetiracetam, full stop (Bhatti et al., 2015). The two drugs that loom large in the canine add-on conversation are off the table: potassium bromide is contraindicated in cats because it can cause fatal lower-airway and lung disease, and imepitoin isn't licensed for cats at all, so neither should ever be a feline second drug (Bhatti et al., 2015). The evidence for levetiracetam as a feline add-on is admittedly thin: in a small series of 12 cats given it on top of phenobarbital, 4 of the 7 with clear before-and-after data responded, but it is the established feline second agent and generally well tolerated (Bailey et al., 2008).
When this means drug-resistant epilepsy
There's a threshold worth naming, gently. If your dog keeps seizing despite two appropriately chosen, well-tolerated, adequately dosed drugs, whether on their own or in combination, that meets the formal definition of drug-resistant, or refractory, epilepsy (Potschka et al., 2015). Roughly 20 to 40% of dogs with epilepsy never reach fully satisfactory control and fall into this group, and one expert review argues the true figure in dogs may be even higher than in people, partly because the drugs licensed for dogs largely share a single mechanism of action (Löscher, 2022).
Reaching that point is not a verdict on you or your dog. It's a recognised stage, and crossing into it doesn't mean the options are exhausted; it means the conversation widens into what refractory epilepsy explained and advanced add-on treatments cover. So if your dog or cat is still seizing on their first drug, the useful next move isn't despair, it's a methodical one: confirm the basics, then decide with your vet whether to add a second drug or carefully change course. Bring your diary. The numbers in it are what turn this from a frightening guess into a plan you can both act on.
References
- - Bailey KS, Dewey CW, Boothe DM, Barone G, Kortz GD. Levetiracetam as an adjunct to phenobarbital treatment in cats with suspected idiopathic epilepsy. Journal of the American Veterinary Medical Association. 2008;232(6):867-872.
- - Bhatti SFM, De Risio L, Muñana K, Penderis J, Stein VM, Tipold A, Berendt M, Farquhar RG, Fischer A, Long S, Löscher W, Mandigers PJJ, Matiasek K, Pakozdy A, Patterson EE, Platt S, Podell M, Potschka H, Rusbridge C, Volk HA. International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research. 2015;11:176.
- - Charalambous M, Brodbelt D, Volk HA. Treatment in canine epilepsy: a systematic review. BMC Veterinary Research. 2014;10:257.
- - Kajin F, Meyerhoff N, Charalambous M, Volk HA. "Resistance Is Futile": a pilot study into pseudoresistance in canine epilepsy. Animals. 2023;13(19):3125.
- - Löscher W. Dogs as a natural animal model of epilepsy. Frontiers in Veterinary Science. 2022;9:928009.
- - Muñana KR, Thomas WB, Inzana KD, Nettifee-Osborne JA, McLucas KJ, Olby NJ, Mariani CJ, Early PJ. Evaluation of levetiracetam as adjunctive treatment for refractory canine epilepsy: a randomized, placebo-controlled, crossover trial. Journal of Veterinary Internal Medicine. 2012;26(2):341-348.
- - Neßler J, Rundfeldt C, Löscher W, Kostic D, Keefe T, Tipold A. Clinical evaluation of a combination therapy of imepitoin with phenobarbital in dogs with refractory idiopathic epilepsy. BMC Veterinary Research. 2017;13:33.
- - Packer RMA, Nye G, Porter SE, Volk HA. Assessment into the usage of levetiracetam in a canine epilepsy clinic. BMC Veterinary Research. 2015;11:25.
- - Podell M, Fenner WR. Bromide therapy in refractory canine idiopathic epilepsy. Journal of Veterinary Internal Medicine. 1993;7(5):318-327.
- - Potschka H, Fischer A, Löscher W, Patterson N, Bhatti S, Berendt M, De Risio L, Farquhar R, Long S, Mandigers P, Matiasek K, Muñana K, Pakozdy A, Penderis J, Platt S, Podell M, Rusbridge C, Stein V, Tipold A, Volk HA. International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research. 2015;11:177.
- - Royaux E, Van Ham L, Broeckx BJG, Van Soens I, Gielen I, Deforce D, Bhatti SFM. Phenobarbital or potassium bromide as an add-on antiepileptic drug for the management of canine idiopathic epilepsy refractory to imepitoin. The Veterinary Journal. 2017;220:51-54.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine