
How Dose Titration Works
Dr. Alastair Greenway
MRCVS
A medication has been started, and now your vet keeps talking about "adjusting the dose." You go back for a blood test, the dose changes, you go back again. Meanwhile your dog has had another seizure, and the question that nearly everyone asks at this point is a fair one: is this actually working, or are we just fiddling?
The process stops feeling like guesswork once you can see what it's doing, which is a careful search for the right amount of drug for your particular dog. That search has a name, titration, and it's meant to be gradual and take time. A seizure while you're still in the middle of it doesn't mean the drug has failed. Here's why.
Why there's no single "correct" dose
There isn't one right dose of an anti-seizure drug that works for every dog of a given weight. Two dogs of identical size, given the same dose in milligrams per kilogram, can end up with quite different amounts of drug in their bloodstream, because their bodies absorb and break it down at different rates. So the label dose is a sensible starting point, not a finished answer.
That's why your vet doesn't simply set a dose and walk away. The international veterinary epilepsy consensus is unusually clear on this: "A dog with adequate seizure control, but serum drug concentrations below the reported therapeutic range, does not require alteration of the drug dose, as this serum concentration may be sufficient for that individual" (Bhatti et al., 2015). That overturns what most of us assume. If your dog's seizures are well controlled, a blood level that looks "low" on paper is not a problem to be fixed. The dog is the evidence, not the number.
The goal isn't to hit a textbook figure. It's to find, as the consensus puts it, "the lowest possible concentration associated with >50% reduction in seizure frequency or seizure-freedom and absence of intolerable adverse effects" (Bhatti et al., 2015): the smallest amount of drug that gets the seizures under control without making your dog feel rotten. That sweet spot is personal to your dog, and titration is the process of feeling your way towards it.
What your vet weighs at every adjustment
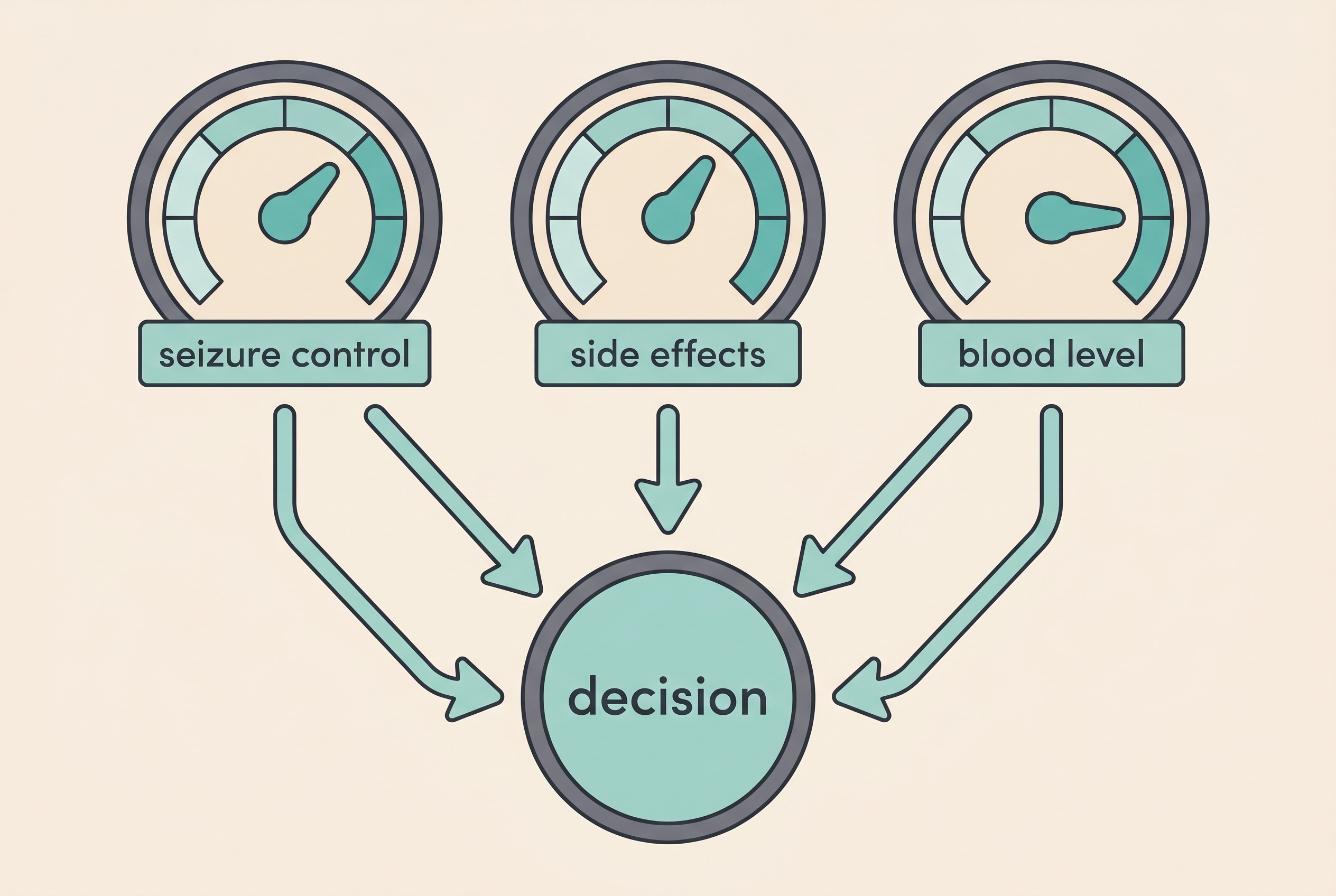
A dose change is never decided on one piece of information alone. Your vet holds three things in mind at once and balances them. The first is seizure control: are the seizures getting less frequent, shorter, milder, measured against where you started (Bhatti et al., 2015)? The second is side effects: is your dog wobbly, flat, ravenous, drinking the water bowl dry? A dose that stops the seizures but leaves your dog miserable hasn't hit the target. The third, for some drugs but not all, is the blood level, an objective read on how much drug is actually circulating.
That blood number is never read in isolation. It informs the decision, it doesn't make it, and it sits alongside the diary and how your dog is coping (Bhatti et al., 2015). The mechanics of the test, when it's taken, what trough and peak mean, how to read the figures, are covered in therapeutic drug monitoring. For now, all you need to hold onto is that levels guide titration; they don't dictate it.
Steady state, and why the waiting is the point
The hardest part of titration to sit with is the waiting, and the reason for it is genuinely reassuring.
When you start a daily medication, the amount in the bloodstream doesn't jump to its final level overnight. It climbs over several doses until it reaches a stable plateau, where what goes in each day balances what the body clears. Pharmacologists call this steady state, and it's the moment a dose can be fairly judged. Judge it before then and you're judging a level that's still on its way up.
How long that takes depends entirely on the drug, and the contrast between them is the clearest way to see why titration is patient by nature.
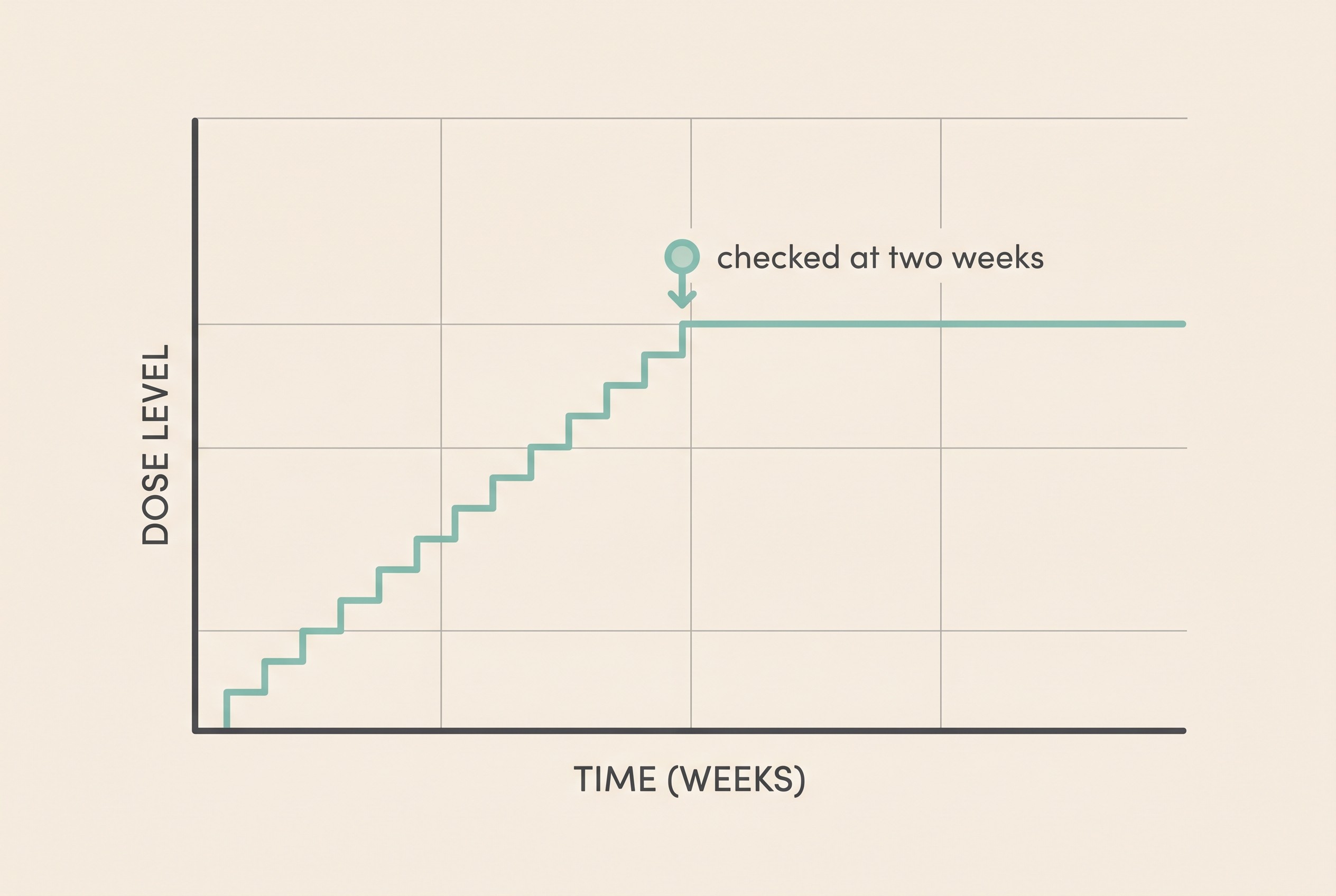
Take phenobarbital, one of the mainstay drugs. Its starting dose in dogs is usually around 2.5 to 3 mg/kg twice daily, then adjusted from there (Bhatti et al., 2015). The first blood level isn't checked on day two or three; it's checked at fourteen days, because that's roughly how long the level takes to settle (Bhatti et al., 2015). So you're already looking at a fortnight before the first proper assessment.
There's also a wrinkle that shows why titration is iterative rather than one-and-done. Phenobarbital nudges the body into clearing it faster over the first few weeks, a quirk called auto-induction. As the consensus describes it, "with chronic PB administration in dogs, its total body clearance increases and elimination half-life decreases progressively which stabilizes between 30 to 45 days after starting therapy" (Bhatti et al., 2015). So a level which looked fine at two weeks can quietly drift down by week six, which is exactly why a second check is often done then (Bhatti et al., 2015). A small upward adjustment at that point isn't a sign anything's gone wrong; it's the system working as designed.
Potassium bromide, another option in dogs, sits at the far end of the patience scale. Its half-life is long, between 25 and 46 days, and "it can take several months (approximately 3 months) before steady-state concentrations after treatment initiation at maintenance dose are reached" (Bhatti et al., 2015). With bromide you genuinely wait a season to judge a single dose change; the patience is built into the chemistry of the drug. One important caution: potassium bromide is not used in cats, where it can cause serious lung disease. The full drug-by-drug picture lives in the anti-seizure drugs compared.
Titration doesn't always mean blood tests at all. Imepitoin, sold in the UK as Pexion, is titrated purely on response. The starting dose is 10 mg/kg twice daily, and "if seizures are not adequately reduced following a minimum of 1 week of treatment at the current dose, the dose can be increased by 50 to 100% increments up to a maximum dosage of 30 mg per kg administered twice daily" (Pexion SPC; consistent with Bhatti et al., 2015, who note there's no useful correlation between its blood concentration and effect). No bloods to chase, just a stepwise climb judged on the seizures themselves: proof that "titration" and "blood tests" aren't the same thing. How Pexion works is covered in imepitoin explained.
Seizures during titration are expected
Seizures can still happen while you're titrating, and that is expected. It does not mean the drug has failed.
It follows from everything above. Because the level is still climbing to steady state, two weeks for phenobarbital or three months for bromide, and because dose-finding happens in steps rather than one leap, a breakthrough seizure during this window is normal (Bhatti et al., 2015). A drug deserves a fair trial, at an adequate dose, for an adequate length of time, before anyone concludes it isn't working (Bhatti et al., 2015; Potschka et al., 2015). The temptation after another frightening seizure is to feel the medication is useless, but usually the opposite is kindest: hold steady, keep logging, and give the dose the time it needs.
Your part in this: the diary
Your vet can only titrate against evidence, and the most useful evidence is your record of the seizures. Frequency is the main thing treatment is measured against, alongside how long each seizure lasts, how severe it is, whether any came in clusters, how your dog recovers afterwards, and which doses were given or missed (Potschka et al., 2015; Bhatti et al., 2015).
A good diary turns "I think he's maybe a bit better?" into something a vet can act on: "seizures went from three a month to one a month after the dose went up." That before-and-after is the whole point, because a dose change is judged against your dog's baseline. The yardstick most vets use is the responder threshold, a 50% or greater reduction in seizure frequency (Bhatti et al., 2015), and you can't know whether you've cleared it without the numbers from before and after each adjustment. What "success" really means, and why complete freedom from seizures is an uncommon goal, is explored in realistic goals: control, not cure.
This is what the Seizure Diary is built for. It timestamps each event, charts your dog's frequency so you and your vet can see the trend at a glance, and gives you a record to bring to every appointment. Logging well is the most powerful way you can take part in your dog's titration.
Two things never to do yourself
There's one firm safety rule. Never adjust or stop the medication on your own, and never stop it abruptly. Stopping suddenly can trigger cluster seizures or even status epilepticus, the prolonged, dangerous kind. Even when a drug is being deliberately withdrawn under veterinary direction, the consensus advises tapering slowly: "to prevent withdrawal seizures or status epilepticus it is advised to decrease the dose with 20% or less on a monthly basis" (Bhatti et al., 2015). That tells you how cautiously these drugs are handled, even on the way down.
So titration is your vet's call, made on the evidence you provide; your part is consistency. The practical side of that, missed doses, pilling a reluctant dog, building a reliable routine, is covered in giving medication reliably.
When one drug stops being enough
Titration isn't infinite. There's a ceiling, and phenobarbital shows it clearly. For most dogs, good control needs a level around 25 to 30 mg/l, and concentrations above 35 mg/l start to carry a real risk of liver damage (Bhatti et al., 2015). So once your dog is up near that safe upper limit and the seizures still aren't acceptably controlled, the answer is not to keep pushing the same drug higher. The conversation changes.
At that point, the rational next step is usually to add a second drug rather than force the first past its safe range. There's even a formal name for the situation where two well-chosen, properly used and tolerated drugs both fail to bring sustained control: drug-resistant epilepsy (Potschka et al., 2015). Recognise this transition when it arrives, but don't read it as the end of the road, because it isn't. Whether to add on or switch, and which second drug to reach for, lives in when the first drug isn't enough.
A note for cat owners
The principle is identical for cats: start sensibly, give it time to reach steady state, then adjust to the seizures, the side effects and, where relevant, the level. What differs is the toolkit. In cats, phenobarbital is first-line, with levetiracetam second. Potassium bromide is not used in cats at all, because of the risk of serious lung disease, and imepitoin isn't licensed for them either (Bhatti et al., 2015). So apply the phenobarbital timeline above to your cat and set the bromide one aside. The feline drug picture in full is covered in the anti-seizure drugs compared and what causes seizures in cats.
Give yourself permission to be patient. Titration looks like uncertainty from the outside, but from the inside it's methodical, and seizures along the way are part of the journey, not proof of failure. Your most valuable contribution is the unglamorous one: every dose on time and a faithful Seizure Diary. And if you reach the ceiling of one drug and the seizures still aren't where you want them, that's not a dead end. It's the cue to move on to when the first drug isn't enough.
References
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Farquhar, R., Long, S., Mandigers, P., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
- Pexion (imepitoin) 100 mg / 400 mg tablets for dogs. UK Summary of Product Characteristics, Boehringer Ingelheim. NOAH Compendium / VMD Product Information Database. Accessed June 2026.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine