
Realistic Goals: Control, Not Cure
Dr. Alastair Greenway
MRCVS
A few months into treatment, a particular kind of disappointment turns up in the consulting room, and it almost always comes from the same place. The owner started their dog on medication expecting the seizures to stop. Just stop. So when one breaks through, even after months of calm, it lands like a failure: the drug isn't working, we've done something wrong, we're back to square one.
I'd like to head that off before it takes root, because it's built on a misunderstanding of what these medicines are for. Anti-seizure medication is not usually a cure, and it isn't designed to be one. It's designed to give your dog fewer, shorter, gentler seizures and a good life in between them. That's not a watered-down version of success. For most dogs, that is success.
If you haven't yet made the decision to start treatment at all, that's a separate question covered in when should treatment start. This article picks up just after that decision, when the tablets are in the cupboard and you're wondering what to hope for.
What "good control" actually means
The international veterinary epilepsy consensus puts the goal about as plainly as a panel of specialists ever puts anything. The aim of treatment, they write, is "to balance the ability to eliminate epileptic seizures with the quality of life of the patient", and they're candid that "seizure eradication is often not likely in dogs". The more realistic goals, in their words, are "to decrease seizure frequency, duration, severity and the total number of epileptic seizures that occur over a short time span", with side effects you and your dog can live with (Bhatti et al., 2015).
So good control isn't a single number. It's a cluster of improvements, and any of them is worth having:
- Fewer seizures, with a longer stretch of normal days between them.
- Shorter seizures, passing more quickly when they do come.
- Less severe seizures, perhaps a focal twitch where there used to be a full collapse, with a gentler recovery.
- Fewer clusters, less tendency for one seizure to roll into several in a day.
- A side-effect load you and your dog can both live with (Bhatti et al., 2015; Potschka et al., 2015).
That last point matters more than owners expect, and I'll come back to it. For now, hold onto the shape of the thing: you're aiming to bend the curve, not flatten it to zero.
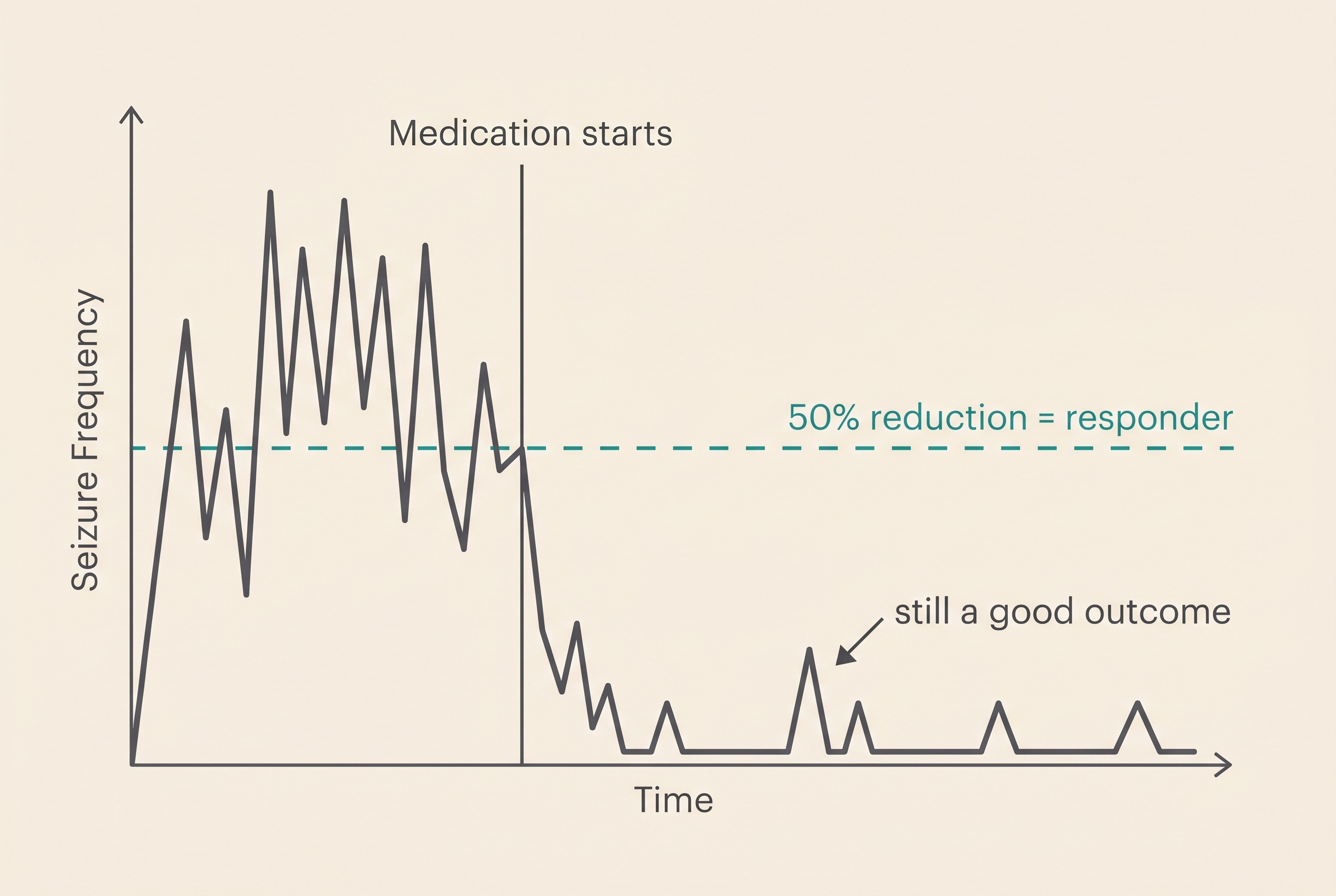
Why a 50% drop counts as a win
In epilepsy medicine, a dog who responds to a drug isn't defined as a dog who never seizes again. A "responder" is conventionally a dog whose seizures drop by at least half: "usually at least 50% or more reduction defines a drug responder" (Bhatti et al., 2015).
If your dog was having a seizure a fortnight and now has one a month, that's a responder. That's the medicine doing its job, by the standard the specialists themselves use. Calling that "the drug failing" is the single most common trap in epilepsy care.
The real-world figures back this up, and they're more encouraging than the forums suggest. In the largest UK study of everyday primary-care epilepsy patients, 344 dogs on phenobarbital, only 14% became completely seizure-free, yet 64.5% reached that 50%-or-better responder threshold (Packer et al., 2014). Complete freedom was the exception, but a substantial, life-changing reduction was the norm for nearly two dogs in three. A smaller group stayed harder to control, and that's a separate story I'll point you to shortly.
Why complete freedom is uncommon
Total seizure freedom does happen. It's just not the realistic benchmark to measure your dog against. Across hospital-based populations, which tend to gather the more stubborn cases, full remission is reported in roughly 15 to 30% of dogs (Bhatti et al., 2015), and the primary-care figure above sat lower still at 14% (Packer et al., 2014).
The consensus on treatment outcomes is deliberately explicit about this, because the specialists know how heavy the word "failure" sits on an owner. Seizure freedom is named as the ideal. But the same document formally recognises partial therapeutic success as a genuine, valuable outcome in its own right: preventing cluster seizures or the dangerous prolonged seizures called status epilepticus, and reducing how often or how severely your dog seizes, all count as real wins (Potschka et al., 2015). Keeping your dog out of the emergency clinic is a success even if the diary never reads zero.
So when you log a seizure after a long quiet spell, the right question isn't "has the treatment failed?" It's "what does the trend look like over months?" One event on a falling curve is not the disease winning.
Treat the dog, not the number
The outcome consensus is clear that treatment should be judged against a whole list of factors, not seizure frequency in isolation, and that list explicitly includes drug side effects and your dog's quality of life (Potschka et al., 2015). You're not managing a graph. You're caring for an animal who has to live inside the results.
That matters because seizure control and side effects pull against each other. Pushing the dose harder to squeeze out the last few seizures can buy you more sedation, wobble, weight gain and thirst. The framing from the people who study this is that treatment is "a fine balance of potential benefits and harms" (Packer & Volk, 2015). A dog who is seizure-free but sleeps through their own life has not necessarily had a better outcome than a dog who has the occasional mild event but is bright and themselves the rest of the time.
This is also why owners' instincts tend to be right. When researchers actually asked, owners rated their dog's quality of life as more important than the raw seizure count, even though most research had historically chased the count (Packer & Volk, 2015). Your sense that a good life is the real prize isn't soft-heartedness getting in the way of the medicine. It's the same conclusion the evidence reaches.
Where the right balance sits is genuinely individual, which is the point of agreeing it with your vet rather than reading it off a chart. One owner will happily accept a seizure every couple of months to keep their dog lively and side-effect-free. Another, watching their dog cluster, will accept a sleepier dog to stay out of the emergency clinic. Both can be exactly right.
Setting the goals, and knowing where you stand
So what does this look like in practice? You and your vet agree two things: roughly what reduction is realistic for this dog, and what level of side effect you're willing to live with to get there. Then you track it, because none of it works on memory and impressions.
This is where a seizure diary stops being admin and becomes the most useful tool you own. It's the objective record that turns "I feel like there have been a few more lately" into a frequency line your vet can act on. Log the date and time of each event, how long it lasted, how severe it was, whether it came as a cluster, and how the recovery went (Bhatti et al., 2015; Potschka et al., 2015). Over months, that record tells you and your vet whether you've hit your responder target, whether there's room to ease off a dose that's causing side effects, or whether it's time to think about the next step.
One firm line while we're on doses. If the seizures improve dramatically, the temptation to wean off the medication and "see if they're cured" can be strong. Don't, and never stop the drugs abruptly, because sudden withdrawal can trigger clusters or status epilepticus (Bhatti et al., 2015). Good control is a reason to stay the course, not to test fate. The day-to-day of dosing, including what to do about a missed one, is covered in giving medication reliably.
It's also worth fixing the emergency line in your mind now, so a bad moment doesn't catch you guessing. A single short seizure that your dog recovers from is frightening but not, by itself, an emergency. What does warrant a call to your vet or the emergency clinic straight away is a seizure lasting more than five minutes, two or more seizures in 24 hours, or seizures coming back-to-back without a clear recovery in between (Bhatti et al., 2015).
A quick word for cat owners
The principle is identical for cats: the goal is reduction and quality of life, not a guaranteed cure (Bhatti et al., 2015). What differs is the medicine cabinet, not the philosophy. Feline epilepsy is treated first with phenobarbital and then levetiracetam, and two drugs you'll see discussed for dogs are off the table for cats: potassium bromide is contraindicated in cats, and imepitoin isn't licensed for them (Bhatti et al., 2015). The drug detail belongs in the comparison pieces, but the target you're aiming at is the same.
What hope realistically looks like
I'd rather you held two true things at once than one comforting half-truth. The expectation to set down is that a cure is uncommon, and a breakthrough seizure on a good run is not a catastrophe or a verdict on your care. The hope to hold up is that most treated dogs improve markedly, and a great many live full, happy lives with their epilepsy as a managed background condition rather than the main event (Packer & Volk, 2015). What that good life actually looks like, day to day and over the years, is its own piece: can a dog with epilepsy live a normal life.
And if your dog turns out to be one of the harder ones to control, that isn't the end of the options, and it's not a reflection of anything you did. A meaningful minority of dogs need more than a first drug at a good dose, and there's a recognised pathway for exactly that, set out in drug-resistant (refractory) epilepsy explained.
For most of you, though, the road ahead is steadier than the first frightening weeks suggest. Aim for fewer, shorter, gentler seizures and a dog who's still recognisably themselves between them. Keep the diary so you can see the curve rather than guess at it. That's not settling for less. It's aiming at the target your dog can actually hit, and most of them do.
References
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Packer, R. M. A., Shihab, N. K., Torres, B. B. J., & Volk, H. A. (2014). Clinical risk factors associated with anti-epileptic drug responsiveness in canine epilepsy. PLoS ONE, 9(8), e106026.
- Packer, R. M. A., & Volk, H. A. (2015). Epilepsy beyond seizures: a review of the impact of epilepsy and its comorbidities on health-related quality of life in dogs. Veterinary Record, 177(12), 306-315.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Farquhar, R., Long, S., Mandigers, P., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine