
When Should Treatment Start?
Dr. Alastair Greenway
MRCVS
Your dog has had a seizure, maybe two. The bloods and the examination point towards epilepsy, and now the question on the table is whether to put a young, otherwise healthy animal on a tablet every twelve hours for life. It is one of the hardest conversations I have, and it usually lands at the worst possible moment. Search online and you'll find people who started after a single fit and swear it saved their dog, others who waited years and managed beautifully, and plenty who'll tell you you're either jumping the gun or leaving it dangerously late. Small wonder it feels impossible.
There is no rule that fires on seizure count alone, and no forum verdict can settle this for your individual animal. The decision to start anti-seizure medication is a shared, individualised one, made with your vet, and it rests on a handful of specific things: the cause of the seizures, how likely they are to recur, their type and severity, the side effects you'd be taking on, and your own circumstances (Bhatti et al., 2015). This article owns that decision and its timing. It doesn't cover which drug to choose, what good control looks like long-term, or how to give medication day to day, and I'll point you to the home of each as we go.
Starting isn't failure, and waiting isn't automatically safer
Neither path is a moral one. Starting medication doesn't mean you've given up on your dog, and holding off isn't the cautious, virtuous choice it can feel like at two in the morning. Both "treat now" and "watch and wait" are legitimate medical positions, and which one is right depends entirely on the picture in front of you.
What makes this answerable rather than agonising is that two large, independent expert panels have looked hard at exactly this question and landed in almost the same place. When the International Veterinary Epilepsy Task Force in Europe (Bhatti et al., 2015) and the American College of Veterinary Internal Medicine panel in the United States (Podell et al., 2016) reach near-identical conclusions working separately, you can lean on their criteria with confidence.
What tips the balance towards treating
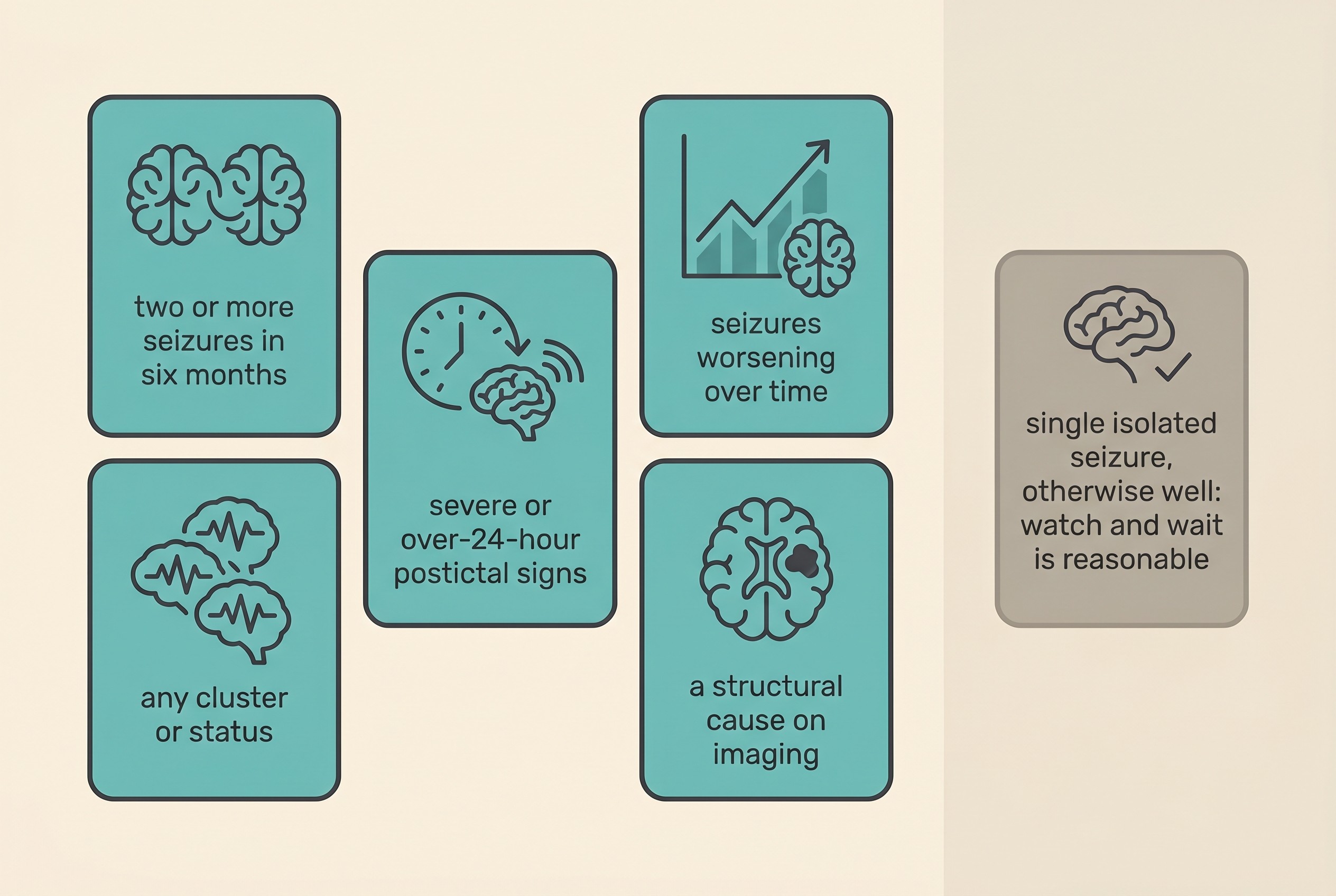
The IVETF recommends starting long-term medication when any one of the following is present (Bhatti et al., 2015):
- Two or more seizures within a six-month period (put another way, an interictal period, the gap between seizures, of six months or less).
- Cluster seizures or status epilepticus (more than one seizure in a day, or a prolonged seizure).
- Postictal signs that are especially severe, such as aggression or blindness, or that last longer than 24 hours.
- Seizures getting worse over time: increasing in frequency or duration, or deteriorating in severity, across three interictal periods.
The ACVIM panel echoes that list and adds one trigger explicitly: a known structural cause, meaning an identifiable lesion on imaging or a prior history of brain disease or injury, is itself a clear reason to treat (Podell et al., 2016).
Notice what these criteria have in common. None is a tally of seizures for its own sake. They are about pattern and risk: seizures coming close together, running into each other, recovering badly, or trending the wrong way, plus the separate flag of a visible cause in the brain. That framing is deliberate, and it's a sounder way to think than "we'll start after the third one."
When watch-and-wait is reasonable
Look back at that list and you'll see that a single seizure, or a rare and isolated one, in an animal who is otherwise well, with a normal examination and no structural or metabolic cause found, doesn't meet any of the triggers. So for that animal, watching and waiting is a perfectly reasonable plan (Bhatti et al., 2015; Podell et al., 2016). It isn't negligence, and it isn't fobbing your dog off. It's a proportionate response to a single event that may never repeat.
The condition attached to watching and waiting is the part people skip, and it's the most important bit: you have to actually watch, and you have to log. Every seizure, with its date, time, duration, what it looked like, and how the recovery went. Those are the exact inputs the criteria above are built on, and they turn a vague "he's had a few" into a clear picture your vet can act on. This is where our Seizure Diary earns its place, and where filming an event becomes genuinely useful: video and a good diary are repeatedly singled out as the two most valuable things an owner can bring (De Risio et al., 2015). If anything changes, more frequent seizures, a longer one, a rough recovery, you go back to your vet, and the conversation may well shift towards treating.
There's an important earlier fork too. A one-off seizure caused by a toxin, low blood sugar, or another metabolic insult is a reactive seizure, not epilepsy, and the answer is to treat the underlying cause, not to commit your animal to lifelong anti-seizure drugs (Berendt et al., 2015). That's precisely why the diagnostic workup comes before the treatment decision.
What starting actually commits you to
If the decision goes towards treating, it's only fair to be clear about what you're taking on. It means daily, lifelong dosing, typically every twelve hours, given consistently. For the drugs that need it, phenobarbital and bromide, it means routine blood tests to monitor levels and organ health (Bhatti et al., 2015). And it means one non-negotiable safety rule that I'll repeat in every article where dosing comes up: you never stop anti-seizure medication abruptly. Suddenly withdrawing the drug can trigger cluster seizures or status epilepticus, sometimes worse than anything your animal had before. If a dose ever needs to come down, it's done gradually and under veterinary direction, the IVETF suggests by no more than around 20% per month (Bhatti et al., 2015). This isn't a tablet you start on a whim and stop when you feel like it, which is part of why the decision deserves real thought rather than a panic call after one frightening night.
The mechanics of a reliable daily routine, missed doses and pilling a reluctant patient live in giving medication reliably, and the choice between drugs belongs in the anti-seizure drugs compared. Here I just want you to hold the shape of the commitment in mind as part of the decision.
The goal is reduction, not cure
Before you say yes, set your expectations clearly, because this single point prevents a lot of later heartache. The aim of treatment is to reduce seizures, not to abolish them. In the words of the consensus itself, "seizure eradication is often not likely in dogs" (Bhatti et al., 2015). The conventional definition of a treatment "responder" is a 50% or greater reduction in seizure frequency, and that, not zero seizures, is what success usually looks like (Bhatti et al., 2015; Potschka et al., 2015).
Hearing that now, at the point of deciding, is far kinder than discovering it after months of feeling the medication has "failed" because the odd seizure still gets through. It hasn't failed: fewer, shorter, less severe seizures is the win we're playing for, and many dogs do very well by that measure. What good control actually looks like is the job of realistic goals: control, not cure.
Treating early helps, but it's pattern that counts, not a race
You'll often hear that the sooner you start, the better the long-term control, and there is something to it. The IVETF notes that control "is thought to be most successful when appropriate AED therapy is started early in the course of the disease, especially in dogs with a high seizure density," and points to the human-medicine observation that a high seizure frequency before treatment tends to predict a poorer response (Bhatti et al., 2015). Taken alone, that sounds like a clear case for not dawdling.
But the best canine data complicate the simple "treat sooner equals better" story. When researchers looked at what actually predicts whether a dog responds to medication, the total number of seizures before treatment was not a significant predictor. What did predict a poorer outcome was seizure density and cluster seizures, and being male (Packer et al., 2014). It isn't a stopwatch running against a seizure count, it's the pattern that counts, which is exactly why clusters and status are hard triggers to treat in the first place. So don't let anyone frighten you that you've "missed the window" because you sensibly watched and waited after one isolated seizure, and don't let anyone tell you a single fit means you must medicate this afternoon or doom your dog.

The broader prognosis is worth knowing, lightly, because it motivates treating the difficult patterns rather than despairing of them. In a referral population, only around 14% of treated dogs with idiopathic epilepsy reached complete, seizure-free remission, while around 64.5% achieved that 50%-or-better reduction; dogs with cluster seizures did markedly worse, with roughly 17.9% reaching remission (Packer et al., 2014). That's real support for "control, not cure," and a reason to take the cluster and high-density patterns seriously rather than read the numbers as defeat. A referral population is, by definition, weighted towards the trickier cases, and plenty of dogs managed in first-opinion practice never become a statistic like this.
A note for cat owners
The decision framework above applies just as much to cats. The same questions, recurrence risk, severity, pattern and cause, drive the call. What differs is the drug set, and here the safety rules are firm. In cats, phenobarbital is the first-line choice, followed by levetiracetam (Charalambous et al., 2018). Two drugs you'll see discussed for dogs must not be carried across: potassium bromide is contraindicated in cats, because it can cause severe and sometimes fatal lower-airway disease, and imepitoin (Pexion) is not licensed for cats, its authorisation covers dogs only (European Medicines Agency, 2013). Please don't let a dog forum talk you into either for your cat.
One feline cause deserves a mention because it changes the decision entirely. Permethrin or pyrethroid toxicity, usually a dog spot-on flea treatment accidentally applied to a cat, is a common cause of feline seizures, and it's a reactive seizure and an emergency, not epilepsy (Berendt et al., 2015). The treatment is removing and reversing the poison, urgently, not starting a lifelong anti-seizure drug. The feline drugs themselves are covered in the anti-seizure drugs compared.
How to have the conversation
When you sit down with your vet, arrive with evidence rather than impressions: how many seizures, over what span of time, whether any came in clusters or ran long, how your animal recovered each time, and whether the trend is upward. Those are the precise inputs to the criteria, and a well-kept diary turns them from guesswork into something you can both reason from (De Risio et al., 2015).
The emergency line sits above all of this and overrides any "let's watch and wait" plan: a seizure lasting more than five minutes, or two or more seizures in 24 hours, or seizures running into one another without a recovery in between, is an emergency. Get to your vet or an emergency clinic now, and ring ahead. A single short seizure with a normal recovery is frightening, but it isn't, by itself, an emergency. Knowing that distinction is part of being ready to decide calmly rather than in a panic.
No single right moment is written down for every animal, but there is a clear, evidence-based map of when treatment is warranted, and you don't have to read it alone. Whether the answer today is "let's start" or "let's keep watching together," you'll be making it from the same place your vet is: the actual pattern of your animal's seizures, rather than the loudest voice on the internet. Keep logging in the Seizure Diary, because whichever way the decision goes now, that record is what will guide every adjustment that comes after it.
References
- Berendt, M., Farquhar, R. G., Mandigers, P. J. J., Pakozdy, A., Bhatti, S. F. M., De Risio, L., Fischer, A., Long, S., Matiasek, K., Muñana, K., Patterson, E. E., Penderis, J., Platt, S., Podell, M., Potschka, H., Pumarola, M. B., Rusbridge, C., Stein, V. M., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research, 11, 182.
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Charalambous, M., Pakozdy, A., Bhatti, S. F. M., & Volk, H. A. (2018). Systematic review of antiepileptic drugs' safety and effectiveness in feline epilepsy. BMC Veterinary Research, 14(1), 64.
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Mandigers, P. J. J., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Pumarola, M. B., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- European Medicines Agency. (2013). Pexion (imepitoin): EPAR and summary of product characteristics. Authorised indication: reduction of the frequency of generalised seizures due to idiopathic epilepsy in dogs. Target species: dogs. European Medicines Agency / EU Commission Register.
- Packer, R. M. A., Shihab, N. K., Torres, B. B. J., & Volk, H. A. (2014). Clinical risk factors associated with anti-epileptic drug responsiveness in canine epilepsy. PLoS ONE, 9(8), e106026.
- Podell, M., Volk, H. A., Berendt, M., Löscher, W., Muñana, K., Patterson, E. E., & Platt, S. R. (2016). 2015 ACVIM Small Animal Consensus Statement on Seizure Management in Dogs. Journal of Veterinary Internal Medicine, 30(2), 477-490.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Farquhar, R., Long, S., Mandigers, P., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine