
The Anti-Seizure Drugs Compared
Dr. Alastair Greenway
MRCVS
Four drug names do most of the work in canine and feline epilepsy: phenobarbital, Pexion, bromide and Keppra. Once you and your vet agree it's time to treat, the question becomes which of them, and why that one rather than another. There's a lot of strong opinion attached to each name, so what this page offers instead is a steady map: the real options, what each one is genuinely good at, where each one falls down, and how a vet weighs them up for the dog or cat in front of them.
This article assumes the decision to treat has already been made. If you're still weighing up whether to start at all, that's a different conversation, and it lives in when should treatment start. This piece is the other half: not whether, but which.
One thing first. None of these drugs is a cure. The realistic goal is to reduce seizures, not abolish them. The international consensus on treating canine epilepsy puts it plainly: "Seizure eradication is often not likely in dogs. More realistic goals are to decrease seizure frequency, duration, severity and the total number of epileptic seizures" (Bhatti et al., 2015). A dog or cat counts as a "responder" when seizures fall by at least half, and that genuinely is a good result (Bhatti et al., 2015). I'd rather you held that realistic expectation from the start than measured every drug against an impossible standard.
Before any drug: the underlying strategy
Whatever drug your vet reaches for, the strategy is usually the same, and it explains a lot of what follows. The standard approach is monotherapy first: start a single first-line drug at an adequate dose, allow it time to build up to a steady level in the blood, monitor the response, and adjust to effect before anyone reaches for a second drug. Add-on drugs come in only when a single agent, at a proper dose and level, has failed to control the seizures (Bhatti et al., 2015). So if your vet starts with one drug and seems in no hurry to pile on more, that patience is the textbook approach, not a lack of urgency.
The second principle is one that genuinely matters: never stop an anti-seizure drug abruptly. Stopping suddenly, or letting doses lapse, can trigger withdrawal seizures, a cluster, or even status epilepticus, the dangerous prolonged seizure state. If a drug ever needs to be withdrawn or swapped, it's done by slow tapering, with the consensus advising the dose come down by around 20% or less per month (Bhatti et al., 2015). This holds no matter how well your pet seems, and no matter how much you dislike a side effect. The answer to a side effect is a phone call to your vet, never a sudden stop.
And the choice is individualised. There's no league table with a single winner at the top. The right drug depends on the species, the seizure pattern, other health problems, and a few practical realities I'll come to. So treat what follows as a fair description of the contenders, not a recommendation.
Two first-line drugs for dogs
For dogs, the menu of licensed first-line drugs in the UK and Europe is short. There are only two: phenobarbital and imepitoin, the latter sold as Pexion (Bhatti et al., 2015). Everything else is an add-on or used off the licence, so the first real decision usually comes down to a straight choice between these two.
Phenobarbital (phenobarbitone) is the long-established mainstay, for good reason. When the blood level is kept in the right range, it reduces seizure frequency in around 60 to 93% of dogs with idiopathic epilepsy (Bhatti et al., 2015). The catch is that it needs therapeutic drug monitoring: blood tests to check the level sits in the target range, roughly 25 to 30 mg/l for most dogs, with levels above 35 mg/l carrying an increased risk of liver damage and best avoided (Bhatti et al., 2015). Early on it can cause sedation, wobbliness (ataxia), a bigger appetite, and increased thirst and urination, though many of these settle as the dog adjusts (Bhatti et al., 2015; Tipold et al., 2015). Because it's processed by the liver, liver monitoring is part of the deal. That liver question deserves more space than a fair comparison should give it, so I'm handing the full picture to phenobarbital, what to expect and the blood-testing detail to therapeutic drug monitoring.
Imepitoin (Pexion) is the newer option, developed and licensed specifically for dogs (Bhatti et al., 2015; Charalambous et al., 2018). It's licensed first-line for dogs with recurrent single generalised seizures, and the evidence behind it is good. In the pivotal blinded, randomised trial of 226 dogs, imepitoin came out non-inferior to phenobarbital, meaning comparable seizure control (Tipold et al., 2015). Its appeal is tolerability and convenience. It's generally better tolerated, and it needs no routine blood-level monitoring, because it has a wide safety margin and its blood concentration doesn't track neatly with its effect (Tipold et al., 2015; Bhatti et al., 2015). In that head-to-head trial, sedation, increased thirst and increased appetite were all significantly more common in the phenobarbital group, and it was phenobarbital, not imepitoin, that pushed up the liver enzymes (Tipold et al., 2015).
So why isn't imepitoin simply the obvious choice for everyone? One important limit. Its effectiveness hasn't been shown for cluster seizures or status epilepticus. The consensus is careful with its wording: "its efficacy has not yet been demonstrated in dogs with cluster seizures or status epilepticus" (Bhatti et al., 2015). For a dog whose seizures come in clusters, that's a real mark against it. It's given twice daily, usually starting around 10 mg/kg and titrated up towards 30 mg/kg, and it shouldn't be used in dogs with severe liver, kidney or heart problems (Boehringer Ingelheim, n.d.; Bhatti et al., 2015). The full imepitoin story, a dog-only one, lives in imepitoin (Pexion) explained.
When one drug isn't enough: the add-ons
When a first-line drug at a proper dose isn't enough on its own, two other drugs come into play. Both are worth knowing about even now, because they shape where treatment can go.
Potassium bromide (KBr, sold in the UK as Libromide) is the old guard. In most of the UK and Europe it's licensed only as an add-on, for dogs whose epilepsy hasn't responded well to first-line treatment, most often on top of phenobarbital (Bhatti et al., 2015; Dechra, n.d.). It has one standout virtue: it isn't processed by the liver at all but excreted unchanged by the kidneys, which makes it useful for a dog whose liver is already struggling (Bhatti et al., 2015). The trade-off is that it's fussy about diet. Bromide is reabsorbed in the kidney in competition with chloride (salt), so a change in how much salt your dog eats shifts the blood level. Dogs on bromide need a consistent diet to keep the level stable, and it needs blood-level monitoring as phenobarbital does (Bhatti et al., 2015). I'll come to the one absolute rule about bromide and cats shortly, because it matters more than anything else on this page.
Levetiracetam (Keppra) is the well-tolerated all-rounder. Side effects are uncommon and usually mild: some sedation, a touch of wobbliness, a slightly reduced appetite, the odd bout of vomiting (Bhatti et al., 2015). It's used as an add-on, with the consensus judging there to be "fair" evidence to recommend it as an adjunctive drug (Bhatti et al., 2015). In the UK it isn't licensed for veterinary use, so it's prescribed under the cascade, the legal route vets use to reach a human-licensed medicine when no suitable animal-licensed one fits (Bhatti et al., 2015; VMD, n.d.). Two caveats worth knowing. The first is the "honeymoon effect": some dogs respond well at first, then gradually develop tolerance over months, so the benefit can fade (Bhatti et al., 2015). The second is practical: its short action means it's usually given three times a day rather than twice (Bhatti et al., 2015). On the plus side, it lends itself to pulse dosing for dogs that cluster, an initial 60 mg/kg once a seizure starts or warning signs appear, then 20 mg/kg three times daily until the dog has been seizure-free for 48 hours (Bhatti et al., 2015). The at-home rescue side of this belongs in managing cluster seizures at home; I mention it here only as a comparison point.
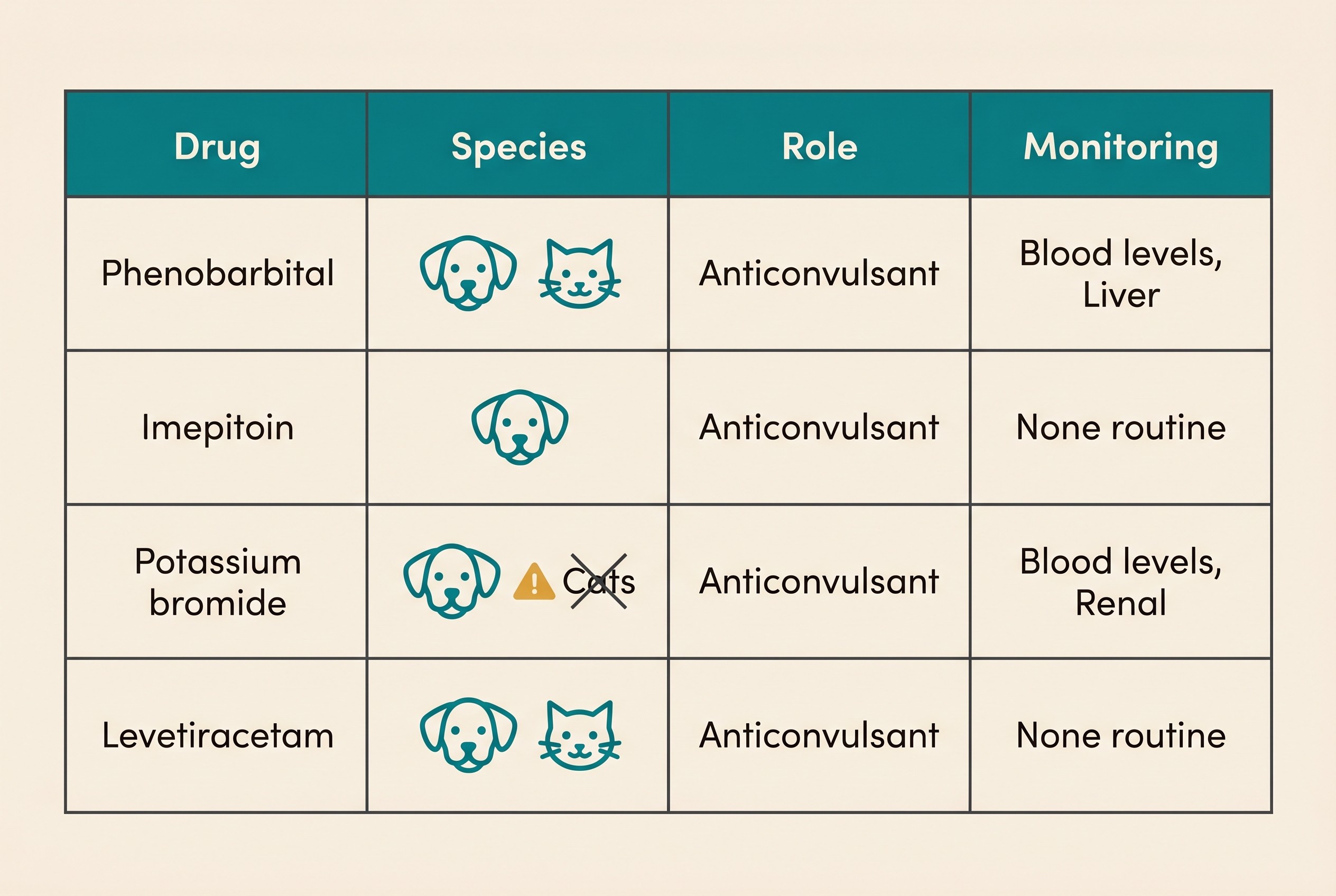
Here's the same picture laid out plainly.
| Drug | Species | Role | Monitoring | Key notes |
|---|---|---|---|---|
| Phenobarbital | Dog and cat | First-line | Blood levels needed (target ~25 to 30 mg/l; avoid above 35) | Effective in roughly 60 to 93% of dogs; processed by the liver; early sedation, appetite and thirst that often settle; feline first-line (Bhatti et al., 2015; Charalambous et al., 2018). |
| Imepitoin (Pexion) | Dog only | First-line | No routine monitoring | Better tolerated, comparable to phenobarbital; not shown to work for clusters or status; not licensed in cats (Tipold et al., 2015; Bhatti et al., 2015). |
| Potassium bromide (Libromide) | Dog only; contraindicated in cats | Add-on (UK) | Blood levels needed | Kidney-excreted so spares the liver; sensitive to dietary salt; causes serious, sometimes fatal airway disease in cats (Bhatti et al., 2015; Bertolani et al., 2012). |
| Levetiracetam (Keppra) | Dog and cat | Add-on / pulse | No levels needed | Well tolerated; honeymoon (tolerance) effect; useful for clusters; three times daily; UK cascade/off-label; feline second-line (Bhatti et al., 2015; Charalambous et al., 2018). |
How your vet actually chooses
So how does a vet land on one drug rather than another? Once you see the reasoning, the choice stops feeling arbitrary. Several threads get woven together.
Species comes first. As you've just seen, dog and cat have different menus, and getting that right is non-negotiable.
Then the seizure pattern. A dog whose seizures come in clusters, or who has had status, points away from imepitoin, whose effect on clusters and status hasn't been shown, and towards phenobarbital, often with levetiracetam or bromide alongside (Bhatti et al., 2015). A dog with isolated, single seizures is a fair candidate for either first-line drug. This is exactly why the record you keep matters so much.
Then other health problems. Existing liver disease tips the balance away from phenobarbital and towards bromide or imepitoin, since bromide is cleared by the kidneys and spares the liver (Bhatti et al., 2015). Severe kidney disease, by contrast, is a reason to be cautious with bromide (Bhatti et al., 2015).
Then the practical realities. Phenobarbital and bromide need regular blood-level monitoring; imepitoin doesn't (Bhatti et al., 2015). Phenobarbital and imepitoin are given twice a day; levetiracetam usually three times (Bhatti et al., 2015). And there's cost and licensing: the licensed options (phenobarbital, Pexion, and Libromide as an add-on) sit alongside cascade or off-label use for levetiracetam (VMD, n.d.; Dechra, n.d.). The lifetime financial picture is its own subject, covered in the cost of epilepsy and how insurance works.
And underneath all of it, the strength of the evidence, plainly stated. The systematic-review evidence is good for phenobarbital and imepitoin, fair for potassium bromide and levetiracetam, and insufficient for most other drugs that occasionally get mentioned (Charalambous et al., 2014). That's why the real choice, for most animals, sits among these four.
Your part: an accurate record
Underneath every driver above sits one piece genuinely in your hands. The seizure pattern, whether a drug is working, whether you've reached that 50% responder mark: all of it traces back to an accurate record of your pet's seizures. Frequency is the number your vet doses against and the yardstick for judging whether the chosen drug is doing its job. Guesswork and memory aren't enough, especially when you're frightened and exhausted and the months blur together.
That's what the Seizure Diary is built for. Logging each seizure, its date and time, how long it lasted, how your pet recovered, and which medication was given or missed, turns a vague impression into the clear picture your vet needs to choose well and adjust sensibly. It's the difference between "I think he's a bit better" and "his seizures have halved since the dose went up." Start it the day treatment begins.
Whichever drug you and your vet settle on, hold the two plain truths. The aim is fewer, milder seizures, not a cure, and that's still a very good outcome. And you never stop the drug suddenly; you pick up the phone instead. From here, the natural next steps are the closer looks at whichever drug is yours, phenobarbital or imepitoin, and, if you're still deciding whether to treat at all, when should treatment start. The choice in front of you has a logic to it, and now you can see it.
References
- Bertolani, C., Hernandez, J., Gomes, E., Cauzinille, L., Poujade, A., & Gabriel, A. (2012). Bromide-associated lower airway disease: a retrospective study of seven cats. Journal of Feline Medicine and Surgery, 14(8), 591-597.
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Mandigers, P. J. M., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
- Boehringer Ingelheim. (n.d.). Pexion (imepitoin) summary of product characteristics / NOAH datasheet (UK).
- Charalambous, M., Brodbelt, D., & Volk, H. A. (2014). Treatment in canine epilepsy: a systematic review. BMC Veterinary Research, 10, 257.
- Charalambous, M., Pakozdy, A., Bhatti, S. F. M., & Volk, H. A. (2018). Systematic review of antiepileptic drugs' safety and effectiveness in feline epilepsy. BMC Veterinary Research, 14, 64.
- Dechra. (n.d.). Libromide (potassium bromide) 325 mg tablets, UK datasheet.
- Tipold, A., Keefe, T. J., Löscher, W., Rundfeldt, C., & de Vries, F. (2015). Clinical efficacy and safety of imepitoin in comparison with phenobarbital for the control of idiopathic epilepsy in dogs. Journal of Veterinary Pharmacology and Therapeutics, 38(2), 160-168.
- Veterinary Medicines Directorate (VMD). (n.d.). The prescribing cascade: guidance on veterinary medicines.
- Vettimes. (n.d.). Feline epilepsy: review of options for treatment and management (with Veterinary Poisons Information Service commentary on permethrin toxicity in cats).
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine