New and Emerging Treatments, Realistically
Dr. Alastair Greenway
MRCVS
Two appropriate medications in, the seizures are still coming, and the midnight search begins. That is the usual route to a page like this one, and the internet has plenty waiting at the other end: a device that stops seizures, a breakthrough drug, an oil that cured someone's dog completely. When you're frightened and watching a dog you love seize, those promises are very hard to look away from.
There is genuinely promising research happening in epilepsy, but very little of it is yet routine, proven veterinary care. Most of what I'm about to walk through has been studied in a handful of dogs, or in one dog, or borrowed from human medicine and not yet validated in animals at all (Nowakowska et al., 2022; Potschka et al., 2015). Promising is not the same as proven.
This article owns the experimental and future horizon: neurostimulation, genuinely novel approaches, and how to tell a real lead from a marketing claim. For the real, available third and fourth-line options a neurologist can layer on right now, see advanced and add-on treatment options. CBD has its own clear-eyed reckoning in CBD for dogs with epilepsy, and diet in diet and epilepsy.
Two rules that hold for everything on this page
Before any of the exciting bits, two things have to stay visible the whole way through, because they're what separate hope from harm.
Start with the goal. Even the emerging options aim at reduction, not cure. Across this field a "responder" means roughly a 50% or greater fall in seizure frequency, not seizure freedom (Potschka et al., 2015). Almost nothing here promises to stop seizures altogether, and any source that promises a cure should raise your suspicion rather than your hopes.
Then the never-stop rule, which matters more here than anywhere. Nothing on this page is a reason to stop or cut your dog's prescribed anti-seizure medication. Every emerging therapy below has been studied as an add-on to ongoing drugs, never as a replacement (Nowakowska et al., 2022; Potschka et al., 2015). Stopping medication abruptly to "try something natural" can trigger cluster seizures or status epilepticus, the opposite of what you want.
If you're starting to wonder what "drug-resistant" really means, drug-resistant epilepsy explained covers that properly and is worth reading first.
Neurostimulation: what it is, and where the evidence really is
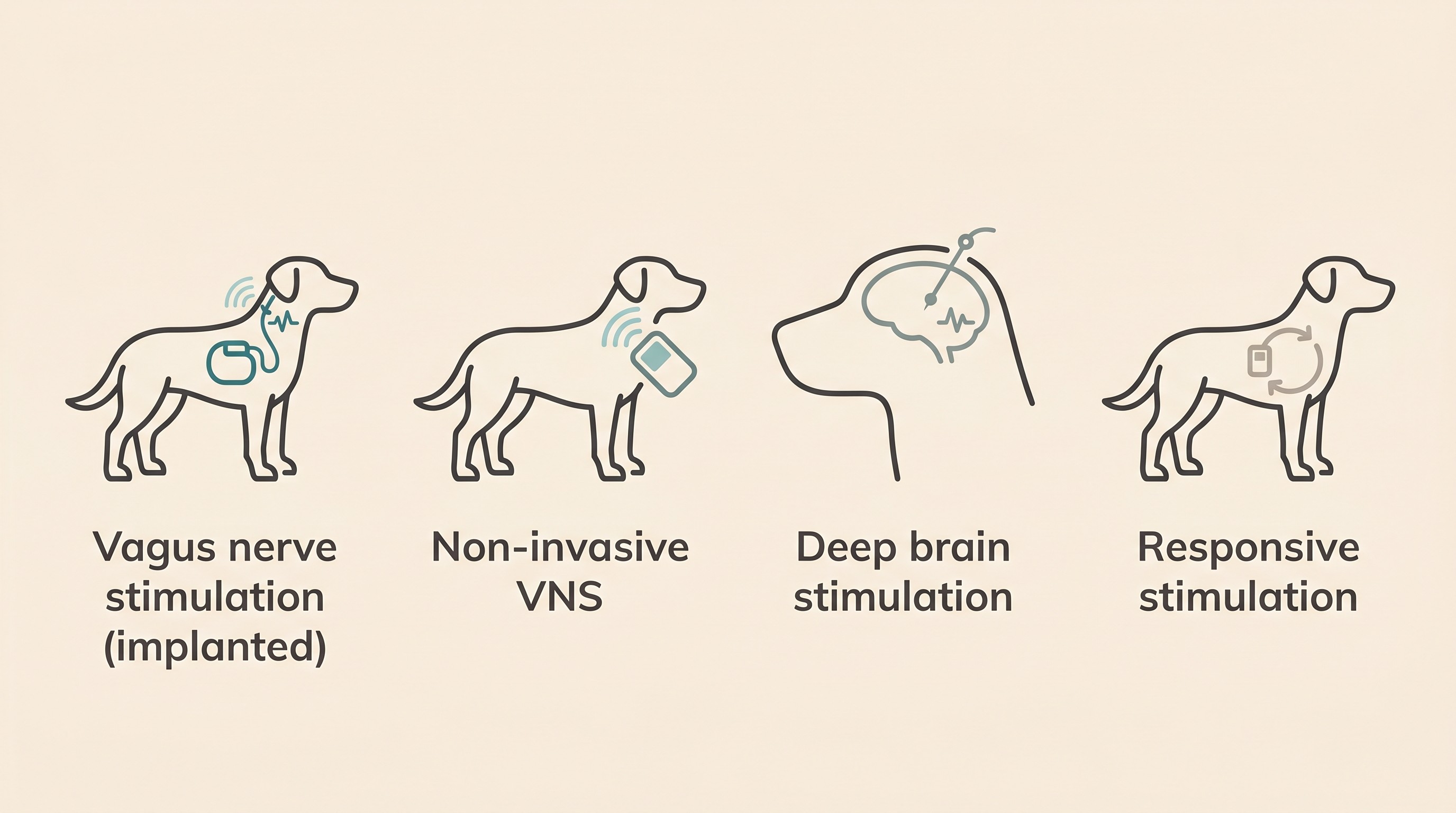
Neurostimulation means using small electrical pulses to change the brain's excitability, either alongside drugs or in place of some of them. In human epilepsy it's an established part of the toolkit. In dogs, it is investigational. I'll walk you through the four approaches plainly, flagging the size of the evidence each time so you can calibrate your own hope (Nowakowska et al., 2022).
Vagus nerve stimulation, the implanted kind. This is the most-studied neurostimulation approach in dogs, and even so it's backed by only a small body of evidence: across every study combined, somewhere around 50 dogs in total (Nowakowska et al., 2022). An implanted, pacemaker-like device delivers intermittent pulses to the vagus nerve in the neck. The original veterinary trial was well designed: a placebo-controlled, double-masked, crossover study in 10 dogs with poorly controlled seizures. Over the full 13-week treatment period there was no significant difference in seizure frequency, duration or severity compared with the control period; only in the final four weeks did a significant 34.4% mean reduction in seizure frequency emerge. The authors concluded that VNS "is a potentially safe approach to seizure control that appears to be efficacious in certain dogs and should be considered a possible treatment option when antiepileptic medications are ineffective" (Muñana et al., 2002).
A more recent long-term study followed 12 dogs with medication-resistant idiopathic epilepsy who kept complete seizure diaries. Seven of the 12, around 58%, met that 50% responder threshold at final assessment, every one of the seven dogs surviving beyond a year was a responder, and monthly seizure frequency kept falling two to three years after the device went in (Harcourt-Brown & Carter, 2023). That is a real, encouraging signal. But the rest of the picture matters: the study was uncontrolled, so we can't be certain the device alone drove the improvement; five of the 12 dogs were euthanised at a median of 256 days after implant; and complications were real, including transient fluid swellings at the surgery site in 8 of the 12, coughing, and two dogs needing a lead replaced. The authors are explicit that prospective controlled trials are still needed before we can claim cause and effect (Harcourt-Brown & Carter, 2023).
So the fair summary for implanted VNS: a real signal, real surgery, real complications, a tiny evidence base, available only at a few specialist and research centres and not a routine option you can simply ask for.
Non-invasive VNS. The appeal here is obvious: a hand-held device (gammaCore VET) that stimulates the vagus nerve through the skin of the neck, with no surgery at all. But the evidence is thinner. The feasibility study was open-label, with no sham device for comparison, and 14 dogs completed it. It found no statistically significant difference in overall seizure frequency versus the control period (p = 0.53), though 4 of the 14 dogs, around 29%, did achieve a 50% or greater reduction. Side effects were mild: a hoarse bark, transient limb trembling, lethargy. The authors called it "a feasible adjunct therapy" that needs "larger sample sizes," and stopped short of endorsing routine use (Robinson et al., 2020). Attractive because it avoids surgery, but no clear group-level benefit yet. Experimental, for now.
Deep brain stimulation. This is electrodes implanted into deep brain structures, in dogs the centromedian nucleus of the thalamus. Here the canine evidence is, quite literally, one dog: a single proof-of-concept case, a 4-year-old mixed-breed with drug-resistant idiopathic epilepsy and status epilepticus, in whom adaptive, rhythm-timed stimulation was associated with no further status epilepticus over about seven months, fewer of the most severe seizures, and a modest reduction in medication. The researchers frame this as exactly what it is, experimental, investigational-device, single-subject pilot work, not established practice (Zamora et al., 2021; Nowakowska et al., 2022). Genuinely interesting science, but one dog, requiring advanced neurosurgery, nowhere near a treatment you can choose.
Responsive neurostimulation. This is the cleverest idea of the four: a "closed-loop" device that detects abnormal brain activity and stimulates only in response, when a seizure is brewing. In dogs, it's the most speculative of all. A couple of dogs have had devices that tracked their seizure activity, but the reports didn't establish whether seizures were actually suppressed (Nowakowska et al., 2022). Tracking a seizure is not the same as treating it, and there's no efficacy data in dogs yet at all.
What runs through all four: they're studied as long-term add-ons for drug-resistant epilepsy, the reported side effects tend to be mild and often local, and the evidence base in dogs is small and mostly uncontrolled (Nowakowska et al., 2022; Potschka et al., 2015). Real ideas, early days.
The other frontiers, briefly
You'll also see talk of novel anti-seizure drugs and of dietary and cannabinoid approaches. These are active areas of research. But the two that owners ask me about most, CBD and diet, are covered properly by sibling articles, and a thin version here would do you a disservice. For CBD, including what the trials found and the important interaction with phenobarbital, read CBD for dogs with epilepsy. For MCT and ketogenic diets, read diet and epilepsy.
Beyond those, I'll resist the temptation to list speculative drug names and doses, and I'd gently encourage you to be suspicious of any page that does. As above, these methods are being studied as long-term adjuncts for drug-resistant epilepsy, the evidence in dogs is still small and largely uncontrolled, and that's the truth a frightened owner deserves rather than a list of compounds nobody can yet stand behind (Nowakowska et al., 2022; Potschka et al., 2015).
Sizing up a "new treatment" claim
You'll keep encountering claims online, in forums, sometimes in a clinic, so here's a short test you can apply to anything you're shown.
Was it studied in dogs (or cats), or only in rodents and humans? Borrowed human results don't automatically transfer to your dog. How many animals were involved, and was there a control or placebo group? A single dramatic case, however moving, is the weakest form of evidence; the strongest veterinary signals here come from controlled studies, and even those are small (Muñana et al., 2002; Robinson et al., 2020). Does the claim promise a cure, or tell you that you can stop the drugs? Both are red flags; the truthful framing is always reduction, as an add-on (Potschka et al., 2015). Is it offered through a specialist or a registered clinical trial, with consent and monitoring, or sold direct to owners on the strength of testimonials? Prefer the former. And run it past your own vet or a neurologist before changing anything, because that conversation catches the things a checklist can't.
If a treatment passes those questions, it's worth a serious conversation. If it fails several, you've probably found marketing wearing the costume of medicine.
The constructive route: clinical trials
Here's the part I actually find hopeful, and it's a real door rather than a false one. If your dog has drug-resistant epilepsy, taking part in a registered clinical trial is often the most responsible way to access something genuinely new. A trial is monitored, properly consented, and it contributes to the evidence other owners will rely on after you. You're not being experimented on in the frightening sense; you're being looked after carefully while helping move the whole field forward.
There are reputable routes to find these. The AKC Canine Health Foundation funds and lists canine epilepsy studies, from dietary and genetic work to home protocols for cluster seizures, and directs owners to its participation pages (AKC Canine Health Foundation, 2024). Veterinary teaching hospitals and neurology referral centres run trials too. Recruitment opens and closes, so rather than chase a specific study, ask your neurologist what's currently recruiting. The practicalities of that referral live in when your vet refers you to a neurologist.
A trial will want a clean, reliable seizure record, and so will any decision about an experimental option. That's exactly what the Seizure Diary is built to produce, a clear log of frequency, duration and clusters that turns a year of frightening nights into evidence a specialist can actually use.
A note for cat owners
I've written this article dog-led for a reason. Almost all of the neurostimulation and emerging-therapy evidence above is in dogs, and the feline evidence is even thinner (Nowakowska et al., 2022). I won't imply any of these options are established for cats, because they aren't. If you're caring for a cat with seizures, the most useful thing I can do is point you back to your vet and to the cat-specific articles, starting with what causes seizures in cats.
Where this leaves you
The realistic message is the one to hold onto when the next miracle claim lands in your feed. Neurostimulation has produced real signals in small numbers of dogs, novel approaches are being studied, and trials are recruiting. But almost none of it is yet routine care, the goal everywhere is reduction rather than cure, and nothing replaces your dog's prescribed medication.
So the useful next steps are small and concrete. Keep the diary, because it's your passport to a trial and to good decisions. Ask your neurologist what's recruiting, and what they can offer today through advanced and add-on treatments. And if you're here because you're wondering how much more your dog can take, that's not a failure of hope; it's a question that deserves its own gentle, candid space, which is quality of life and difficult decisions. The most hopeful thing you can do is stay close to the people who know your dog, and learn to tell the real signal from the noise.
References
- AKC Canine Health Foundation. (2024). Canine epilepsy research initiatives and Participate in Research pages. akcchf.org/epilepsy. Accessed 10 June 2026.
- Harcourt-Brown, T. R., & Carter, M. (2023). Long-term outcome of epileptic dogs treated with implantable vagus nerve stimulators. Journal of Veterinary Internal Medicine, 37(6), 2102-2108.
- Muñana, K. R., Vitek, S. M., Tarver, W. B., Saito, M., Skeen, T. M., Sharp, N. J. H., Olby, N. J., & Haglund, M. M. (2002). Use of vagal nerve stimulation as a treatment for refractory epilepsy in dogs. Journal of the American Veterinary Medical Association, 221(7), 977-983.
- Nowakowska, M., Üçal, M., Charalambous, M., Bhatti, S. F. M., Denison, T., Meller, S., Volk, H. A., Kanber, B., et al. (2022). Neurostimulation as a method of treatment and a preventive measure in canine drug-resistant epilepsy: current state and future prospects. Frontiers in Veterinary Science, 9, 889561.
- Potschka, H., Fischer, A., Löscher, W., Patterson, N., Bhatti, S., Berendt, M., De Risio, L., Farquhar, R., Long, S., Mandigers, P., Matiasek, K., Muñana, K., Pakozdy, A., Penderis, J., Platt, S., Podell, M., Rusbridge, C., Stein, V., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: outcome of therapeutic interventions in canine and feline epilepsy. BMC Veterinary Research, 11, 177.
- Robinson, K., Platt, S., Stewart, G., Reno, L., Barber, R., & Boozer, L. (2020). Feasibility of non-invasive vagus nerve stimulation (gammaCore VET) for the treatment of refractory seizure activity in dogs. Frontiers in Veterinary Science, 7, 569739.
- Zamora, M., Meller, S., Kajin, F., Sermon, J. J., Toth, R., Benjaber, M., Dijk, D. J., Bhatti, S. F. M., Volk, H. A., Sharott, A., Denison, T., et al. (2021). Case report: embedding "digital chronotherapy" into medical devices, a canine validation for controlling status epilepticus through multi-scale rhythmic brain stimulation. Frontiers in Neuroscience, 15, 734265.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine