The treatments compared: Apoquel, Cytopoint, steroids, ciclosporin and immunotherapy
Dr. Alastair Greenway
MRCVS
Look up any of these itch drugs online and you'll spot a pattern fast: almost every page explaining them is published by the company that makes one of them. Apoquel's makers tell you about Apoquel, Cytopoint's about Cytopoint, each leaving the quiet impression that theirs is the answer. This is the version none of them can write. No brand is the hero here. For most itchy pets the real answer isn't a single drug but a tailored combination chosen with your vet, layered on two non-negotiable basics and adjusted as your pet's life and the seasons change. And not one of these treatments cures the disease.
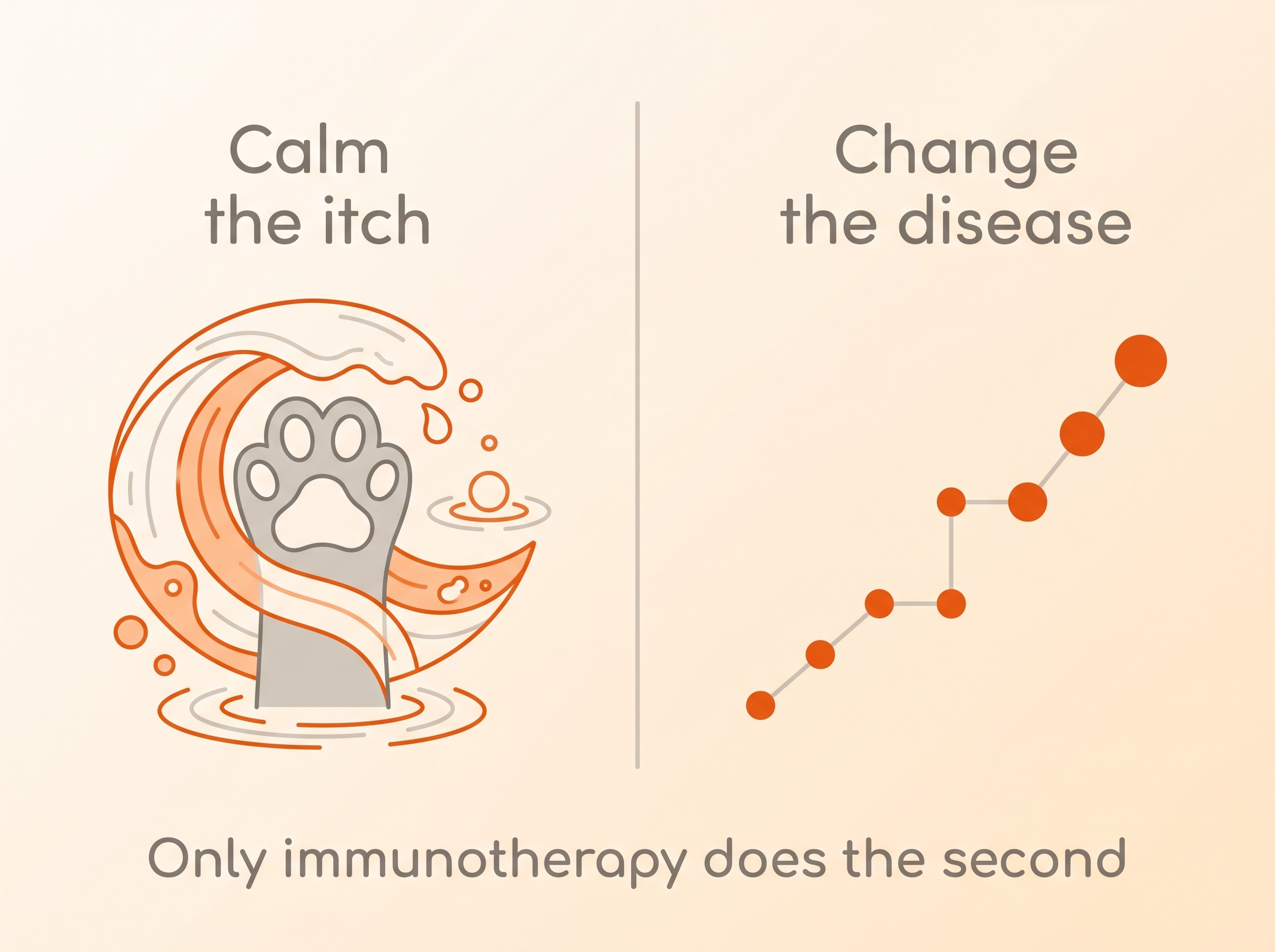
Two jobs, and only one drug does the second
It helps enormously to see that there are two completely different jobs to be done, and most of these treatments only do the first. The first job is stopping the suffering now: calming the itch and clearing the inflamed, sore skin so your pet can sleep, settle and stop chewing. The second job is changing the underlying allergy over time, so the pet needs less treatment in the first place. Almost everything you'll be offered does the first job. Only one thing, allergen-specific immunotherapy, attempts the second (Olivry et al., 2015).
The other thing to hold onto is that atopic dermatitis, the most common reason for this kind of lifelong itch, is managed and not cured. The international veterinary dermatology guidelines (ICADA) are built entirely around control, and say openly that treatment must be adjusted across a pet's life and between flare and calm (Olivry et al., 2015). The drug-maker pages tend to skip past this. It's kinder to say it plainly: you're choosing a way to keep your pet comfortable for years, not a one-off fix.
Sort the foundations before any drug
Before any itch drug can work properly, two things underneath it have to be sorted, because no medicine works well over the top of them. The first is fleas. A single untreated flea problem can drive an allergic pet's itch on its own, and the guidelines are clear that year-round, rigorous flea control is foundational (Olivry et al., 2015). The mechanics of getting fleas genuinely gone live in flea control that works. The second is infection. Allergic skin and ears very commonly develop secondary bacterial or yeast infections that are intensely itchy in their own right, and what looks like a drug "not working" is frequently an untreated infection sitting underneath, which is exactly why the guidelines name secondary infection a common cause of flares (Olivry et al., 2015). That belongs to skin and ear infections. Get those two right, and the picture often improves before you've changed the allergy medicine at all.
Drugs that stop the itch fast
Oclacitinib (Apoquel) is a daily tablet and, for many dogs, the fastest relief on offer. It is a Janus kinase (JAK) inhibitor: it blocks the internal signalling of a range of pro-inflammatory and itch-driving cytokines that depend on JAK enzymes, including IL-31, the key "itch" messenger (Cosgrove et al., 2013a). In its large blinded, placebo-controlled trial of 299 dogs it gave rapid, effective control of both itch and skin lesions, with relief often inside a day (Cosgrove et al., 2013b), and a decade of real-world use has confirmed that fast onset and generally good tolerability (Marsella, 2023). It is licensed in dogs for atopic and allergic dermatitis, given twice daily for up to 14 days then once daily for maintenance, and it is not for dogs under 12 months or 3 kg, nor those with evidence of immune suppression or progressive cancer (EMA Apoquel SPC; Cosgrove et al., 2013b).
It deserves a fair word too. It is an immunomodulator, and that is not nothing: it can increase susceptibility to infection and is best paired with periodic check-ups, watching for infection and skin masses, plus bloodwork on long-term use (EMA Apoquel SPC; Cosgrove et al., 2015). The cancer question has been raised, partly by analogy with human JAK inhibitors. The largest study to look, an age- and breed-matched retrospective cohort of 660 allergic dogs, found no significant difference in malignancies between dogs treated long-term with oclacitinib and those treated without it (Lancellotti et al., 2020); the candid ten-year review agrees the data are reassuring but stops short of calling long-term oncological safety fully settled, and recommends ongoing monitoring (Marsella, 2023). And the step down to once-daily is where some dogs lose ground: twice daily controls itch better but is only licensed for the first fortnight (Cosgrove et al., 2013b; Olivry et al., 2015).
Ilunocitinib (Zenrelia) is the newer arrival, and it works the same way: another once-daily JAK-inhibitor tablet, licensed in dogs for the same allergic and atopic dermatitis, and about as fast to quieten the itch (Zenrelia UK SPC, 2025; Forster et al., 2025). Its selling point is the dosing. It is once daily from day one, with no twice-daily fortnight to step down from, and that step-down is exactly where oclacitinib can wobble: in the head-to-head trial some dogs' itch crept back as Apoquel dropped to once-daily around days 14 to 28, while the ilunocitinib group kept improving, leaving its itch and skin scores slightly lower from day 28 on (Forster et al., 2025). The trade-offs, though, are Apoquel's trade-offs, because it is the same class of drug: an immunomodulator not for dogs with immune suppression or progressive cancer, best with periodic bloodwork on long-term use, and not for pups under 12 months (Zenrelia UK SPC, 2025). It is also genuinely new, without the decade of real-world tracking that now sits behind oclacitinib. An alternative to Apoquel, then, rather than a leap past it.
Lokivetmab (Cytopoint) takes a more targeted route. It is a caninised antibody that mops up IL-31, the key itch cytokine, before it can signal (Michels et al., 2016b). It is given as a subcutaneous injection by your vet, roughly monthly; a single dose works fast, within about a day, and in around four out of five dogs lasts the full month, with some getting four to eight weeks and a minority less (Michels et al., 2016b; EMA Cytopoint, 2017). Head to head with ciclosporin it matched it for itch relief at day 28 (about 52% versus 44%), although it did not meet the bar for the skin-lesion score at that early timepoint, with a good safety record (Moyaert et al., 2017).
Because it is a large protein rather than a small-molecule drug, it is not processed by the liver or kidneys, which often makes it the choice for older dogs or those with other illnesses, and it spares the household a daily pill. Its real limits: it treats itch, not the wider inflammation, so some dogs still need a partner; a minority of dogs make antibodies against it or simply stop getting a full month per dose over time; and because both it and oclacitinib ultimately target IL-31, dogs who did not respond to one are less likely to respond to the other (Moyaert et al., 2017). One important point for cat owners: both Apoquel and Cytopoint are licensed in dogs only.
Glucocorticoids (steroids), such as oral prednisolone or a potent topical spray, are cheap, available, and genuinely fast for a bad flare, and the guidelines rate them well (Olivry et al., 2015). They deserve respect rather than fear. A short course to break a flare is reasonable and useful; the trouble is repeated or long-term use. The common dose-related effects are increased thirst, urination and appetite, and in a large UK primary-care study of dogs these were the most reported side effects, prompting a dose reduction in roughly a third of affected dogs and stopping in about a sixth (Elkholly et al., 2020). Long-term, steroids risk iatrogenic Cushing's disease, muscle wastage, thin skin, infections and diabetes (Merck Veterinary Manual). That is precisely why steroid-sparing maintenance exists, and why steroids are best thought of as a short-term tool, not the long-term plan.
Holding the line without the steroids
Ciclosporin (Atopica) is an oral immunomodulator, and it is licensed for both dogs and cats, which gives cat owners a properly studied option. For atopic dermatitis its effect is comparable to oral steroids: in the pivotal head-to-head trial, lesion scores fell about 52% on ciclosporin versus 45% on methylprednisolone, with similar itch relief, and the systematic review confirms equivalent efficacy with a more favourable long-term safety profile (Steffan et al., 2003; Steffan et al., 2006). Its catch is speed. It takes four to six weeks to work, so it is a maintenance drug, not a rescue, and vets often bridge that gap with a short steroid or oclacitinib overlap at the start. The commonest side effects are gastrointestinal, usually transient, and it is suitable for lifelong use with monitoring (Nuttall et al., 2014).
The one treatment that changes the disease
Allergen-specific immunotherapy (ASIT) is the odd one out, and the only one doing that second job. Tiny, gradually rising doses of your pet's own relevant allergens, identified by testing in an already-diagnosed atopic pet, retrain the immune response away from over-reaction. It is the only treatment shown to alter the underlying disease and, alongside proactive topical steroid, to delay flare recurrence (Olivry et al., 2015). Realistically, roughly two thirds of dogs improve (Olivry et al., 2015), and it can reduce or remove the need for daily drugs. It is slow, often taking up to a year to judge, and it is a commitment of years, available as injections or sublingual drops (Mueller et al., 2018). It is uniquely worth raising for young or year-round patients. The full picture lives in immunotherapy for pet allergies, and the testing that selects the allergens in allergy testing.
Don't overlook the plain stuff
Topical and barrier care, regular bathing and omega-3 supplements are real adjuncts with modest evidence: the guidelines grade essential fatty acids as a small benefit, too slow for a flare, and support bathing and topical therapy (Olivry et al., 2015). They lower the overall load rather than fix the problem alone. The daily routine that ties them together belongs to living with an atopic pet.
Putting it together
This is why the guidelines call combination, proactive therapy the standard, not one drug alone: the disease is, in their words, "multifaceted", and treatments "should be combined for a proven (or likely) optimal benefit" (Olivry et al., 2015). Each treatment chips away at a different part of the load, so pairing two with different jobs, say a fast itch-stopper while immunotherapy slowly takes hold, often beats pushing one drug harder. It is the same logic as the itch threshold, the reason lowering several small triggers at once works better than hunting for a single villain, explained in the itch threshold. And if a well-chosen drug still is not holding, look underneath again: an untreated food driver may be sitting below the threshold, and an elimination diet is the only way to test it, which the Elimination-Diet Companion runs for you.
For cats the toolkit is narrower: steroids and ciclosporin (Atopica) are the licensed options, with oclacitinib used off-label by some dermatologists on smaller but reasonable evidence, where most treated cats improve by at least half (Carrasco et al., 2022). Cytopoint has no feline licence at all. The fuller feline story is in feline atopic syndrome.
One problem runs through all of this: you cannot tell whether a treatment is truly working from a gut feeling, because flares come and go on their own. The only reliable way to know is a tracked itch score over weeks, and the Skin & Itch Tracker makes that easy. It matters most for the slow burners: a logged trend on ciclosporin at four to six weeks, or immunotherapy across months, is what tells you and your vet whether to hold, step up or switch, rather than abandoning something that simply had not had time to work yet.
To turn this comparison into a plan for an itchy pet, read calming the flare and controlling the itch; and if you are tired of firefighting and want to change the disease rather than chase it, immunotherapy is where to look next.
References
- Olivry T, DeBoer DJ, Favrot C, et al. Treatment of canine atopic dermatitis: 2015 updated guidelines from the International Committee on Allergic Diseases of Animals (ICADA). BMC Vet Res. 2015;11:210.
- Cosgrove SB, Wren JA, Cleaver DM, et al. A blinded, randomized, placebo-controlled trial of the efficacy and safety of the Janus kinase inhibitor oclacitinib (Apoquel) in client-owned dogs with atopic dermatitis. Vet Dermatol. 2013;24(6):587-597. [cited as Cosgrove et al., 2013b].
- Cosgrove SB, Wren JA, Cleaver DM, et al. Efficacy and safety of oclacitinib for the control of pruritus and associated skin lesions in dogs with canine allergic dermatitis. Vet Dermatol. 2013;24(5):479-e114. [cited as Cosgrove et al., 2013a].
- Gadeyne C, Little P, King VL, et al. Efficacy of oclacitinib (Apoquel) compared with prednisolone for the control of pruritus and clinical signs in dogs with allergic dermatitis. Vet Dermatol. 2014;25(6):512-e86.
- Marsella R. Oclacitinib 10 years later: lessons learned and directions for the future. J Am Vet Med Assoc. 2023;261(S1):S36-S43.
- Cosgrove SB, Cleaver DM, King VL, et al. Long-term compassionate use of oclacitinib in dogs with atopic and allergic skin disease: safety, efficacy and quality of life. Vet Dermatol. 2015;26(3):171-e35.
- Michels GM, Ramsey DS, Walsh KF, et al. A blinded, randomized, placebo-controlled, dose determination trial of lokivetmab (ZTS-00103289), a caninized, anti-canine IL-31 monoclonal antibody in client-owned dogs with atopic dermatitis. Vet Dermatol. 2016;27(6):478-e129. [Michels et al., 2016b].
- Michels GM, Walsh KF, Kryda KA, et al. A blinded, randomized, placebo-controlled trial of the safety of lokivetmab (ZTS-00103289), a caninized anti-canine IL-31 monoclonal antibody in client-owned dogs with atopic dermatitis. Vet Dermatol. 2016;27(6):505-e136. [Michels et al., 2016a].
- Moyaert H, Van Brussel L, Borowski S, et al. A blinded, randomized clinical trial evaluating the efficacy and safety of lokivetmab compared to ciclosporin in client-owned dogs with atopic dermatitis. Vet Dermatol. 2017;28(6):593-e145.
- Steffan J, Favrot C, Mueller R. A systematic review and meta-analysis of the efficacy and safety of cyclosporin for the treatment of atopic dermatitis in dogs. Vet Dermatol. 2006;17(1):3-16.
- Nuttall T, Reece D, Roberts E. Life-long diseases need life-long treatment: long-term safety of ciclosporin in canine atopic dermatitis. Vet Rec. 2014;174(Suppl 2):3-12.
- Elkholly DA, Brodbelt DC, Church DB, et al. Side Effects to Systemic Glucocorticoid Therapy in Dogs Under Primary Veterinary Care in the UK. Front Vet Sci. 2020;7:515.
- Merck Veterinary Manual. Corticosteroids in Animals (Pharmacology). (reputable reference, not primary)
- European Medicines Agency. Apoquel (oclacitinib maleate): Summary of Product Characteristics / EPAR. (regulator/datasheet)
- Zenrelia (ilunocitinib) 4.8 mg and 15 mg film-coated tablets for dogs: UK Summary of Product Characteristics. Veterinary Medicines Directorate; issued August 2025. (regulator/datasheet)
- Forster S, Boegel A, Despa S, et al. Comparative efficacy and safety of ilunocitinib and oclacitinib for the control of pruritus and associated skin lesions in dogs with atopic dermatitis. Vet Dermatol. 2025;36(2):165-176.
- Forster S, Trout CM, Despa S, et al. Efficacy and field safety of ilunocitinib for the control of atopic dermatitis in client-owned dogs: a multicentre, double-masked, randomised, placebo-controlled clinical trial. Vet Dermatol. 2025. (registration field study)
- European Medicines Agency. Cytopoint (lokivetmab): EPAR / Summary of Product Characteristics. Approved 2017. (regulator/datasheet)
- Mueller RS, Jensen-Jarolim E, Roth-Walter F, et al. Allergen immunotherapy in people, dogs, cats and horses: differences, similarities and research needs. Allergy. 2018;73(10):1989-1999.
- (The 664-case retrospective on subcutaneous immunotherapy efficacy in atopic dogs.) Likely: Vovk LU, et al. Efficacy of subcutaneous allergen immunotherapy in atopic dogs: a retrospective study of 664 cases. (open-access, PMC9544551)
- Carrasco I, Ferrer L, Puigdemont A. Efficacy of oclacitinib for the control of feline atopic skin syndrome: correlating plasma concentrations with clinical response. J Feline Med Surg / Vet Dermatol. 2022.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing allergies & skin. Free to join.
Join PetsLikeMine