Giving Your Cat the Best Shot at Remission: The Playbook
Dr. Alastair Greenway
MRCVS
When an owner first hears that a cat, unlike a dog, can sometimes stop being diabetic, the next question is almost always the practical one. Not "is it true," but "what do I actually do?" The why and the biology live in feline diabetic remission, and I'd read that first if you haven't. This page is the doing: the playbook a motivated owner follows, with their vet, to give a cat the best possible shot at coming off insulin.
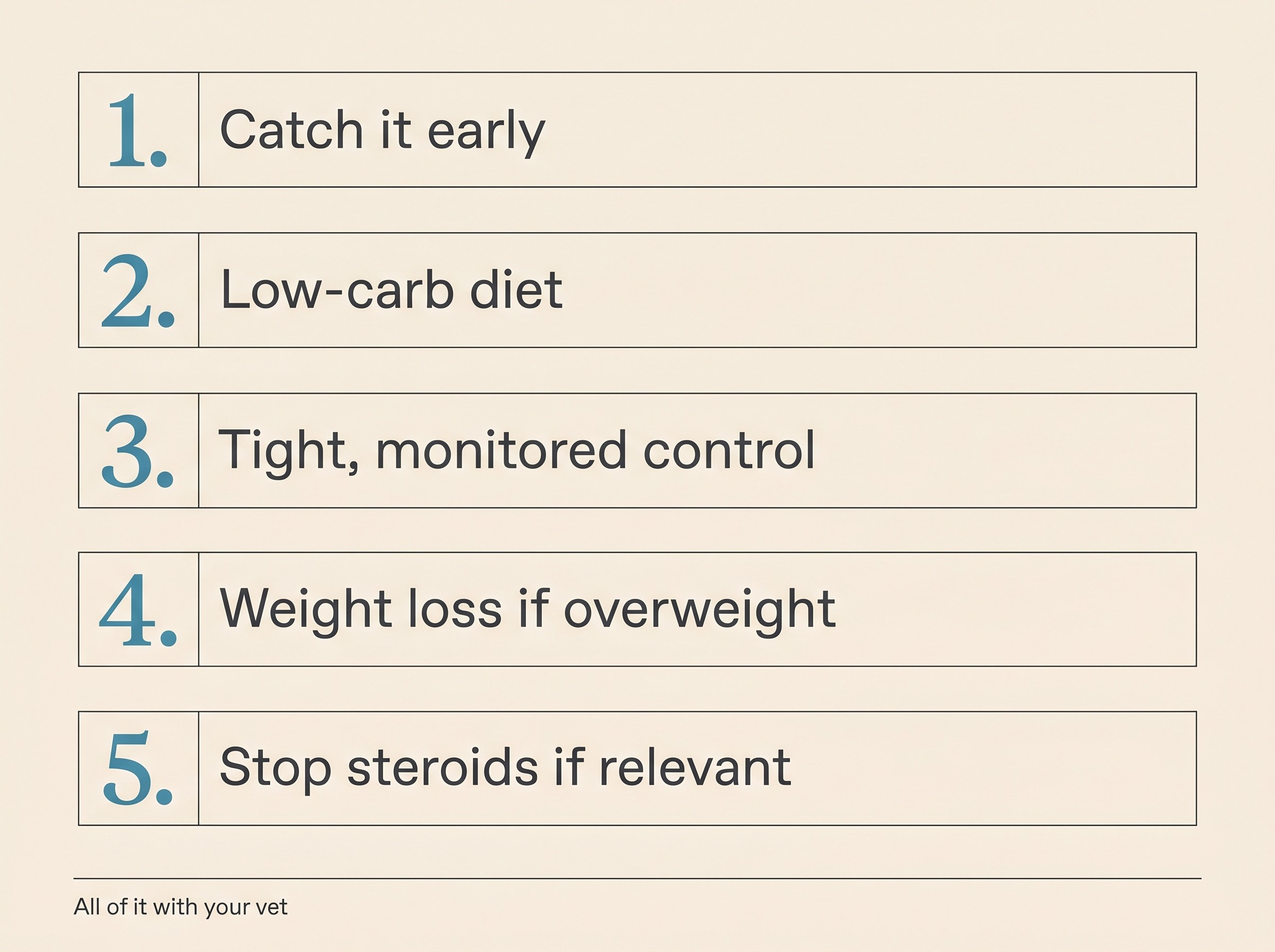
There is a recipe, and it's well evidenced: start early, feed a strict low-carbohydrate diet, get appropriately tight glucose control with monitoring, get an overweight cat losing weight, and strip out any drugs pushing the glucose up. All of it with your vet, never freelanced off a forum. The more of those levers you pull, and the sooner, the better your cat's odds.
First, the real odds, because you deserve a true number rather than a sales pitch. The reported rates are genuinely wide: "variable incidence rates for diabetic remission of 11% to over 60% have been reported in different studies" (Taylor et al., 2025). In a large real-world group on a sensible home protocol, 47% came off insulin (Gottlieb et al., 2024); in the most intensive diet-and-monitoring protocols the figure reaches 64% overall (Roomp & Rand, 2009); and in one small study of newly diagnosed cats started promptly on glargine, every one of eight cats achieved remission (Marshall et al., 2009). So the headline is this: with the right plan, roughly half of cats can come off insulin, and a well-selected, early-treated cat does better still. It's never guaranteed, and a cat who doesn't remit is no failure, but the odds are good enough that the effort is worth it.
Start early: the window narrows fast
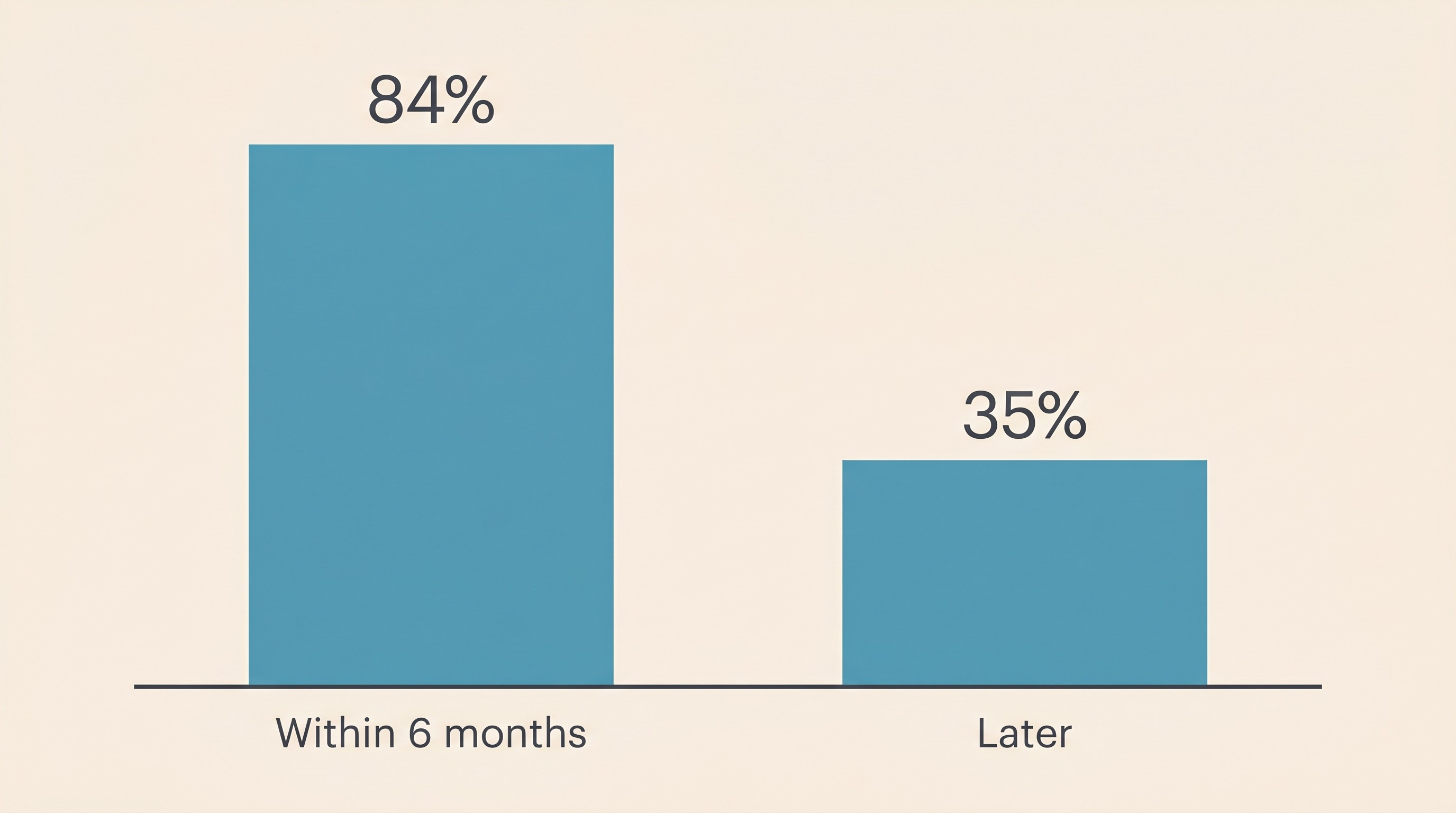
If there's one thing to carry away from this page, it's that the most time-sensitive lever you hold is time itself. The consensus is blunt, "diagnosis and treatment early in the course of the disease can optimise the chance of diabetic remission" (Taylor et al., 2025), and the number behind it is striking. In the intensive-protocol cohort, remission was achieved in 84% of cats started within six months of diagnosis, against only 35% of those who began more than six months after (Roomp & Rand, 2009). More than double the chance, bought purely by not drifting. So don't wait. If your cat has just been diagnosed, the weeks ahead are the most valuable they will ever be for this.
One caveat for expectations. Remission is more likely in cats "with a shorter duration of DM and less severe hyperglycaemia at diagnosis, as well as those achieving good glycaemic control rapidly" (Taylor et al., 2025). A cat already showing the weak, dropped-hock stance of diabetic neuropathy has usually been hyperglycaemic a long time, and such cats "are less likely to enter remission" (Taylor et al., 2025). If that's your cat, it doesn't make the playbook pointless. It makes a comfortable, well-controlled diabetic life the win to aim for, and none of it is your fault.
Feed a strict low-carbohydrate diet
Diet is the biggest dietary move you can make, and it's not a tweak. In the cornerstone trial of 63 diabetic cats over 16 weeks, "significantly more of the cats fed the LC-LF [low-carbohydrate-low-fibre] food (68%, 22/31), compared to the cats fed the MC-HF [moderate-carbohydrate-high-fibre] food (41%, 13/32), had reverted to a non-insulin-dependent state (P = 0.03)" (Bennett et al., 2006). The consensus target is "a diet with a low-carbohydrate content (<25% dry matter, <15% metabolisable energy, <5 g/100 kcal)" (Taylor et al., 2025), and the most aggressive protocols pushed to ultra-low-carbohydrate diets around 10% of metabolisable energy or less (Roomp & Rand, 2009). In practice that's a low-carbohydrate, higher-protein, usually wet or canned food. The why, the protein and carnivore physiology and the dog contrast, belongs to diet for diabetic dogs and cats. Here it's simply step one.
Now the part I will not let you miss, because it's where cats get hurt. Switching to low-carbohydrate food sharply reduces how much insulin a cat needs, often quickly: when diabetic cats moved onto a high-protein, low-carbohydrate diet, "exogenous insulin could be reduced by over 50% with no loss in glucose control", the dose fell in eight of nine cats, and three came off injections altogether (Frank et al., 2001). The dose that was correct on the old food can be an overdose on the new one. So the rule is non-negotiable: never change the diet and chase tight control as a solo move. Do it with your vet, with monitoring, and with the insulin coming down as the glucose falls, or the cat goes hypoglycaemic.
Tight control, but always _with monitoring_
This is the heart of the playbook and its sharpest safety line, so I'll hold the hope and the caution together. Good, prompt control is itself a remission lever, but the protocols that produced the best rates did it with intensive home monitoring, not guesswork. The intensive protocol used "ultra-low carbohydrate diets and the insulin analogue glargine" with frequent home blood-glucose measurement and owner dose adjustment on a written plan, and reported that "only one mild clinical hypoglycaemic episode occurred despite tight blood glucose control" precisely because of that monitoring (Roomp & Rand, 2009). Tight control is earned with data, never guessed.
The counterweight is that pushing for low numbers isn't free. In the real-world cohort, 15.5% of cats were hospitalised for clinical hypoglycaemia (Gottlieb et al., 2024), and interstitial readings "<3.6 mmol/l (<65 mg/dl) are common in cats when there is excellent glycaemic control" (Taylor et al., 2025). That's why this step is inseparable from monitoring, and why the lowest possible number is never the goal: a cat sitting a little high but safe beats a "perfect" reading with a crash, every time. If your cat ever goes wobbly, weak, dull or trembling, treat it as a possible hypo, rub sugar or honey on the gums and ring your vet (never pour liquid into a cat that cannot swallow), and read the hypoglycaemia emergency guide before you need it.
What makes tight control safe is the monitoring, ideally from day one. The consensus recommends that "the FreeStyle Libre is applied continuously to facilitate titration of the insulin dose from the time DM is diagnosed until stabilisation or remission is reached" (Taylor et al., 2025). So run your remission attempt with a continuous glucose monitor or home glucometer and your vet's titration plan, so the dose can be pushed down and the lows caught. The how-to lives in the FreeStyle Libre guide. Use the Glucose Companion to keep the diet change, the falling doses and the readings together in one place. One practical point: human glucometers tend to read pet blood low, so use a pet-calibrated meter or a CGM.
On which insulin, the remission protocols were built on glargine (Roomp & Rand, 2009; Marshall et al., 2009), and "there is also some evidence that the longer acting insulin analogues (glargine and detemir) may be less likely to produce clinical hypoglycaemia when aiming for tighter control of [blood glucose]" (Sparkes et al., 2015), so glargine (Lantus) is the typical workhorse for a remission attempt. That said, the current consensus is even-handed, with PZI (ProZinc) and glargine showing "similar remission rates" (Taylor et al., 2025). The choice is your vet's, and the full line-up is in insulin types for dogs and cats.
Get the weight off
If your cat is overweight, losing it is a named, measurable predictor, and an early drop matters: "weight loss (⩾2% body weight) in obese cats in the first month of insulin treatment of DM has been identified as a predictor of remission" (Taylor et al., 2025). Shedding fat reverses the insulin resistance that drives feline diabetes, and that physiology sits in the weight and control guide. The instruction is just to fold it in: an overweight cat's push includes a gentle, vet-supervised weight-loss plan. A cat must never be crash-dieted, but a steady early loss is part of the recipe.
Strip out the glucose-raising drugs
This is a quietly enormous lever, and the easiest to overlook. If your cat is on, or recently came off, steroids, stopping them where it's safe can be transformative. "Cats treated with corticosteroids who develop DM are more likely to enter remission when corticosteroids are discontinued" (Taylor et al., 2025), and the real-world data put a number on it: recent corticosteroid use was associated with a sevenfold greater chance of remission (OR 7.27, P=0.0005) once stopped (Gottlieb et al., 2024). So the action is simple, and you can do it today: tell your vet about every medication your cat is on, especially steroids and any progestogen-type drugs, so anything raising the glucose can be stopped or switched wherever the underlying condition allows. The wider hunt for hidden insulin resistance is the insulin-resistance workup.
Do it WITH your vet, never off a forum
I'll draw one line clearly, because it's where the internet leads cats astray. The remission protocols are owner-led at the sharp end: their whole point is that "insulin adjustments [are made] based on pre-insulin blood glucose concentration measurements made by the owners at home" (Gottlieb et al., 2024). But every one of them runs on a written plan, intensive monitoring and veterinary backup (Roomp & Rand, 2009; Gottlieb et al., 2024). That's the distinction. Structured home tight-regulation, set up and supervised by your vet with a monitor on your cat, is a brilliant tool and may be the thing that earns remission. Copying a stranger's "tight regulation" numbers off a forum and pushing insulin without a monitor is how cats die of hypoglycaemia. Honour the method, never the freelancing. Never adjust on a single reading, never chase one number, and never double-dose. If you're ever unsure whether a dose went in, skip it and wait for the next one rather than re-dose: a missed dose is a minor blip, a double dose can be fatal.
One brief caveat. Oral SGLT2 inhibitors (Senvelgo in the UK and EU, Bexacat in the US) are not a casual shortcut to remission. They're licensed only for clinically well, newly diagnosed cats that have never had insulin, and carry a real risk of euglycaemic diabetic ketoacidosis, meaning a cat can be in a life-threatening crisis with a normal-looking blood glucose. They can even mask whether a cat has remitted, because the "only way to identify such cats is to stop treatment with SGLT2is and monitor BG" (Taylor et al., 2025). If this route is on the table, it's a careful vet-led decision, covered in insulin types for dogs and cats.
Knowing it's working, and roughly when
How do you know it's working? You watch the insulin requirement fall. In cats on insulin, remission "is supported by effective glycaemic control and indicated by a progressive decrease in insulin requirements or evidence of hypoglycaemia" (AAHA, 2026). The dose keeps needing to come down, the glucose sits in or below range, and lows start appearing on the monitor. Those lows aren't a problem to ignore: they're the cue to step the insulin down, and eventually stop it, always on your vet's say-so. The day the cat holds normal glucose with no insulin, that's remission.
Be patient, because most remissions happen within the first few months, not days. The median time to remission in the real-world cohort was 93 days, with 27% of remitting cats doing so within the first two months (Gottlieb et al., 2024). So treat the early weeks as the investment. Pull every lever hard now, and if remission hasn't come within a few months it becomes less likely, but your cat is still well-managed and comfortable, which is a success in its own right.
One last point: remission isn't a cure to bank on. "Although it might last for years, remission is, by definition, a temporary state" (Taylor et al., 2025), and between 13% and 40% of cats relapse (Taylor et al., 2025). That's not a reason to hold back, it's a reason to keep going afterwards. Once your cat is off insulin, the job shifts to protecting that hard-won remission and catching any relapse early, which is the whole next chapter in staying in remission and spotting a relapse early. Keep logging the diet, the doses and the readings in the Glucose Companion throughout, because the clearest sign the playbook is working is a line sloping gently down towards zero, with no dangerous dips along the way. For roughly half of cats, with the right plan started early, that's a picture you'll actually get to see.
References
- AAHA. (2026). 2026 AAHA Diabetes Management Guidelines for Cats, Section 9 (Diabetic Remission) and Section 6 (SGLT2 Inhibitor Treatment and Monitoring). American Animal Hospital Association.
- Bennett, N., Greco, D. S., Peterson, M. E., Kirk, C., Mathes, M., & Fettman, M. J. (2006). Comparison of a low carbohydrate-low fiber diet and a moderate carbohydrate-high fiber diet in the management of feline diabetes mellitus. Journal of Feline Medicine and Surgery, 8(2), 73-84.
- Frank, G., Anderson, W., Pazak, H., Hodgkins, E., Ballam, J., & Laflamme, D. (2001). Use of a high-protein diet in the management of feline diabetes mellitus. Veterinary Therapeutics, 2(3), 238-246.
- Gottlieb, S., Rand, J. S., & Anderson, S. T. (2024). Frequency of diabetic remission, predictors of remission and survival in cats using a low-cost, moderate-intensity, home-monitoring protocol and twice-daily glargine. Journal of Feline Medicine and Surgery, 26, 1098612X241232546.
- Marshall, R. D., Rand, J. S., & Morton, J. M. (2009). Treatment of newly diagnosed diabetic cats with glargine insulin improves glycaemic control and results in higher probability of remission than protamine zinc and lente insulins. Journal of Feline Medicine and Surgery, 11(8), 683-691.
- Roomp, K., & Rand, J. (2009). Intensive blood glucose control is safe and effective in diabetic cats using home monitoring and treatment with glargine. Journal of Feline Medicine and Surgery, 11(8), 668-682.
- Sparkes, A. H., Cannon, M., Church, D., Fleeman, L., Harvey, A., Hoenig, M., Peterson, M. E., Reusch, C. E., Taylor, S., & Rosenberg, D. (2015). ISFM consensus guidelines on the practical management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 17(3), 235-250.
- Taylor, S., Cannon, M., Church, D., Fleeman, L., Fracassi, F., Gilor, C., Mott, J., Niessen, S., et al. (2025). 2025 iCatCare consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine