Feline Diabetes Explained: Why a Cat's Diabetes Is Its Own Disease
Dr. Alastair Greenway
MRCVS
Most of what gets written about pet diabetes carries, quietly, a canine accent. So if you've just been told your cat is diabetic, here is the thing worth knowing first: your cat's diabetes is not a smaller version of a dog's. It looks far more like human type 2 diabetes, and because the insulin-making cells are damaged rather than entirely gone, a cat caught early has something most diabetic dogs never get: a real chance of coming off insulin altogether. That through-line, resistance plus beta-cell strain but partly reversible, is the key to everything below.
How a cat's diabetes mirrors human type 2
In a cat, two things go wrong together: the tissues become resistant, so insulin does less work, and the beta cells that make insulin start to fail and die off. The current feline consensus puts it plainly, that the disease "is currently assumed to have a similar aetiology to human type 2 DM in 75% to 80% of cases," characterised by "a combination of partial beta cell dysfunction, beta cell loss and insulin resistance" (Taylor et al., 2025). And the resistance is real, with diabetic cats roughly six times less sensitive to insulin than normal cats (Rand, 1999), which is why simply topping up the insulin they can no longer make is only half the job.
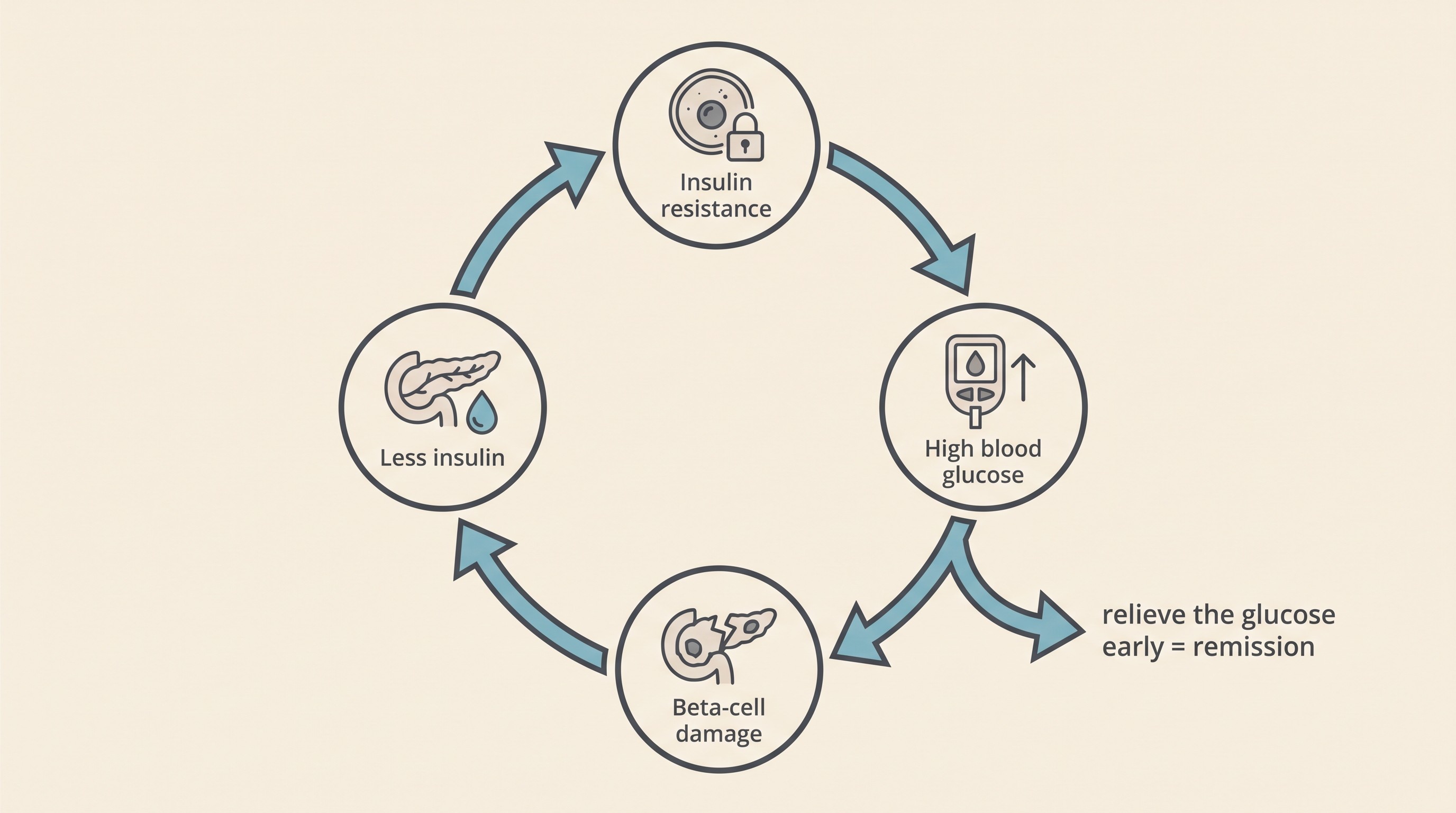
Now the part that drives everything else. High glucose is not just a symptom, it is itself toxic to the beta cells meant to control it, so you get a vicious cycle: resistance pushes the glucose up, the high glucose injures more beta cells, those cells make even less insulin, and the glucose climbs higher still (Taylor et al., 2025; Rand, 1999). We call this glucotoxicity. The hopeful wrinkle is the timing: early on this glucose-driven shutdown of insulin is functional and reversible, and only sustained, untreated high glucose turns it into permanent loss (Rand, 1999). And it isn't armchair theory: holding healthy cats at a high glucose for a sustained period, with a fat infusion as the comparison, showed it was the glucose, not the fat, that caused beta-cell dysfunction and loss (Zini et al., 2009). High sugar damages the very cells that fix high sugar, which is why a new feline diagnosis is never something to simply "keep an eye on." The clock is doing damage.
One more cat signature is worth a line: diabetic cats characteristically lay down a toxic protein called islet amyloid in the pancreas, one of the closest parallels there is to human type 2 disease and another reason the beta cells are slowly lost (Rand, 1999; Clark & Hoenig, 2021). And this is where dogs and cats part company. A diabetic dog has lost almost all beta-cell function and needs insulin for life, with no realistic remission; a diabetic cat has resistance plus partial, declining function, which is why a cat can sometimes come off insulin and a dog essentially never can (Taylor et al., 2025; Behrend et al., 2018). The full head-to-head lives in diabetes in dogs and cats: two different diseases. The line to take is that your cat is not on the dog's track.
Which cats get it
If you're wondering why your cat, the freshest UK picture helps. In more than 1.2 million cats in UK primary-care practice, the annual prevalence of diabetes was about 0.39%, roughly one cat in 256, with an average age at diagnosis of 11.8 years; the odds rose steeply with age, and males were affected substantially more often than females (Waite et al., 2025). So this is mostly a disease of middle-aged and older male cats, none of which is anything you did. The one factor you can change is weight, the most consistently recognised risk factor, working through that same insulin resistance: each extra kilogram is thought to cost a cat in the order of 30% of its insulin sensitivity, so an overweight cat loses well over half of it before ever becoming diabetic (Clark & Hoenig, 2021; Rand, 1999). In an older UK cohort, overweight cats had around three times the odds and inactive cats roughly twice (McCann et al., 2007), and indoor, sedentary, neutered cats are over-represented too (O'Neill et al., 2016). Keeping a cat in is a reasonable safety choice, not a moral failing, but activity and weight are the levers you can pull.

Two more feline notes. The Burmese is a genuine genetic quirk, roughly three to four times more likely to develop diabetes in Australia, Britain and Europe but not in the distinct North American line (Waite et al., 2025; Samaha et al., 2020): feline diabetes has its own genetics, not borrowed from the dog. And steroids and certain hormone treatments cause insulin resistance and can tip a susceptible cat over (Taylor et al., 2025; McCann et al., 2007). That's often reversible, and where another disease is fighting your insulin, concurrent diseases and insulin resistance takes it on.
That partial, declining beta-cell function is also where the hope lives. Because the cells are damaged but not all gone, relieving the high glucose early can let some cats come off insulin entirely: reported remission rates run from around 11% to more than 60%, best with early diagnosis, a low-carbohydrate diet, weight loss and dropping steroids (Taylor et al., 2025; Gottlieb et al., 2024). The caveats are that it isn't every cat, and remission is not a cure, because relapse is possible and monitoring continues (Taylor et al., 2025). I'll keep it to that, because feline diabetic remission and the remission playbook cover it properly.
Monitoring a cat takes a different eye
Here is a feline-specific trap that catches owners, and sometimes vets too. A single high blood-glucose reading at the vet does not, on its own, prove a cat is diabetic or badly controlled, because cats produce stress hyperglycaemia: the simple stress of being grabbed, restrained or frightened can drive a perfectly normal cat's glucose right up, and the consensus is blunt that this response "can be of any magnitude" (Taylor et al., 2025). The mechanism is the struggle itself; a frightened, fighting cat releases noradrenaline and lactate, and the harder it struggles the higher its glucose climbs (Rand et al., 2002). At its worst, stress alone can push a normal cat into the 300 to 400 mg/dL range, roughly 17 to 22 mmol/L, squarely where people expect to see diabetes, from nothing more than a bad five minutes on the table. So we never diagnose, and never adjust an insulin dose, off one frightened-cat reading.
We see through it two ways. The first is a blood test called fructosamine, which reflects average glucose over roughly the preceding one to three weeks and is not moved by a single stress spike (Taylor et al., 2025). In the classic study, merely stressed cats had a median fructosamine of 269 µmol/L, barely above the normal of around 252, while genuinely diabetic cats sat far higher at 624 (Crenshaw et al., 1996), a clean separation a one-off glucose can't give you. The second is to move the measurement out of the clinic to where your cat is relaxed: home blood-glucose testing and, increasingly, a small wearable continuous glucose monitor, both of which the consensus recommends when the two are hard to tell apart (Taylor et al., 2025). The mechanics belong to Stage 3, in home blood glucose monitoring and continuous glucose monitors on pets, but the principle should land: the cat benefits more than any patient from calm data gathered at home, and holding that history in one place is exactly what the Glucose Companion is there for. One note for when you start, human glucose meters read a cat's blood low, so a pet-calibrated meter or a sensor is the better tool, and either way you react to the trend, not to one alarming number.
Oral SGLT2 drugs, and their hard safety line
For decades, treating feline diabetes meant insulin injections, full stop. That's no longer the only option, and the change is a distinctly feline story with one serious warning attached. A class of once-daily oral drugs called SGLT2 inhibitors works differently from insulin, making the kidneys dump excess glucose out in the urine, independently of the cat's own insulin. In the UK and Europe the product is velagliflozin (Senvelgo); the US has a tablet, bexagliflozin (Bexacat), the first oral feline diabetes drug approved there (EMA/CVMP, Senvelgo; FDA/Elanco, Bexacat label). In the right cat they work genuinely well, with bexagliflozin achieving treatment success in around 84% of newly diagnosed cats and velagliflozin shown non-inferior to insulin (Hadd et al., 2023; SGLT2 systematic review, 2025).
But read this next part twice. An SGLT2 inhibitor is not a casual pill you swap in for injections. It is a specific decision for a specific cat, with a real and potentially fatal risk, and it is only for clinically well, newly diagnosed cats with no significant underlying conditions that have never been on insulin (Taylor et al., 2025; FDA/Elanco, Bexacat label). The danger is euglycaemic diabetic ketoacidosis: because the drug constantly strips glucose out through the urine, a cat that runs short of insulin can tip into life-threatening ketoacidosis with a normal, or even low, blood glucose, so the usual high-sugar warning never comes (FDA/Elanco, Bexacat label). And it isn't theoretical: it occurred in roughly one in 15 newly diagnosed cats started on these drugs, rising to about one in 10 if they had previously been on insulin, and cats have died, with the European regulator flagging deaths where unsuitable cats were switched off insulin onto Senvelgo (Taylor et al., 2025; Hadd et al., 2023; EMA/CVMP, Senvelgo). So the rules are firm: never in a cat currently or previously on insulin, never started in one that is unwell at diagnosis, and always a vet's decision, not a way to dodge needles. The fuller comparison lives in the insulin types and oral options for cats.
A last word across the table
There's a small, specific kindness in the feline version worth ending on. Diabetic dogs very commonly go blind from cataracts, around 80% within the first year or so, because of how a dog's lens handles sugar; cats almost never do, because the older feline lens has very little of the enzyme that drives that process, and feline diabetes is a disease of older cats (Beam et al., 1999; Richter et al., 2002). One more way your cat's diabetes is its own disease, and on balance the more forgiving of the two.
None of which makes it nothing: it is a real condition that asks for real commitment. But it is treatable, often very successfully, sometimes reversibly, and your cat is not on a path you should fear. Because it is partly reversible if caught early, the best thing you can do is start gathering calm data at home: set up the Glucose Companion, and read feline diabetic remission when you're ready to reach for the best outcome. The window for that is now, which is the best reason I know to feel purposeful tonight rather than afraid.
References
- Beam, S., Correa, M. T., & Davidson, M. G. (1999). A retrospective-cohort study on the development of cataracts in dogs with diabetes mellitus: 200 cases. Veterinary Ophthalmology, 2(3), 169-172.
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Clark, M., & Hoenig, M. (2021). Feline comorbidities: pathophysiology and management of the obese diabetic cat. Journal of Feline Medicine and Surgery, 23(7), 639-648.
- Crenshaw, K. L., Peterson, M. E., Heeb, L. A., Moroff, S. D., & Nichols, R. (1996). Serum fructosamine concentration as an index of glycemia in cats with diabetes mellitus and stress hyperglycemia. Journal of Veterinary Internal Medicine, 10(6), 360-364.
- EMA/CVMP. (2023). Senvelgo 15 mg/ml oral solution for cats (velagliflozin): European public assessment report and direct healthcare professional communication. European Medicines Agency.
- FDA/Elanco. (2022). BEXACAT (bexagliflozin tablets) prescribing information. NADA 141-557, US Food and Drug Administration.
- Gottlieb, S., Rand, J. S., Anderson, S. T., et al. (2024). Frequency of diabetic remission, predictors of remission and survival in cats using a low-cost, moderate-intensity, home-monitoring protocol and twice-daily glargine. Journal of Feline Medicine and Surgery, 26(4), 1098612X241232546.
- Hadd, M. J., Bienhoff, S. E., Little, S. E., et al. (2023). Safety and effectiveness of the sodium-glucose cotransporter inhibitor bexagliflozin in cats newly diagnosed with diabetes mellitus. Journal of Veterinary Internal Medicine, 37(3), 915-924.
- McCann, T. M., Simpson, K. E., Shaw, D. J., Butt, J. A., & Gunn-Moore, D. A. (2007). Feline diabetes mellitus in the UK: the prevalence within an insured cat population and a questionnaire-based putative risk factor analysis. Journal of Feline Medicine and Surgery, 9(4), 289-299.
- O'Neill, D. G., Gostelow, R., Orme, C., Church, D. B., Niessen, S. J. M., Verheyen, K., & Brodbelt, D. C. (2016). Epidemiology of diabetes mellitus among 193,435 cats attending primary-care veterinary practices in England. Journal of Veterinary Internal Medicine, 30(4), 964-972.
- Rand, J. S. (1999). Current understanding of feline diabetes: part 1, pathogenesis. Journal of Feline Medicine and Surgery, 1(3), 143-153.
- Rand, J. S., Kinnaird, E., Baglioni, A., Blackshaw, J., & Priest, J. (2002). Acute stress hyperglycemia in cats is associated with struggling and increased concentrations of lactate and norepinephrine. Journal of Veterinary Internal Medicine, 16(2), 123-132.
- Richter, M., Guscetti, F., & Spiess, B. (2002). Aldose reductase activity and glucose-related opacities in incubated lenses from dogs and cats. American Journal of Veterinary Research, 63(11), 1591-1597.
- Samaha, G., Wade, C. M., Beatty, J., Lyons, L. A., Fleeman, L. M., & Haase, B. (2020). Mapping the genetic basis of diabetes mellitus in the Australian Burmese cat. Scientific Reports, 10, 19194.
- SGLT2 systematic review. (2025). Efficacy and safety of non-insulin antidiabetic drugs in cats: a systematic review. PMC12427183.
- Taylor, S., et al. (2025). iCatCare 2025 consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
- Waite, O., Gostelow, R., Wright, E., et al. (2025). Frequency, risk factors, and mortality for diabetes mellitus in 1,225,130 cats under primary veterinary care in the United Kingdom in 2019. Journal of Veterinary Internal Medicine, 39(4), e70161.
- Zini, E., Osto, M., Franchini, M., et al. (2009). Hyperglycaemia but not hyperlipidaemia causes beta cell dysfunction and beta cell loss in the domestic cat. Diabetologia, 52(2), 336-346.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine