
Why the weight still will not come: cobalamin, dysbiosis and the slow responders
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
The enzymes go on every meal. The food has been switched. You have been patient, and the pet in front of you is still too thin. At that point a quiet worry tends to set in: what if this just does not work?
Let me lift the worst version of that worry off the table. Most dogs and cats with exocrine pancreatic insufficiency (EPI) do well on pancreatic enzyme replacement therapy (PERT), and once they are through the first stretch the outlook is genuinely good (Batchelor et al., 2007; Cridge et al., 2024). But a real minority do not bounce straight back, and when that happens the answer is almost never "the diagnosis was wrong" or "just pile on more enzymes". A poor response is usually a fixable problem, and the reasons are findable if you work through them in order. This article is that ordered list. It assumes EPI was confirmed on a serum TLI blood test, owned by what EPI is, and that you already have the day-to-day enzyme routine in place.
First, are you actually a non-responder, or just early?
Before chasing anything exotic, rule out the commonest "failure" of all, which is impatience, and I mean that with no blame attached. Recovery from EPI is slow: stool quality usually takes around four weeks of enzymes and the right diet to improve, and body condition can take several months to come back fully, so an owner expecting a transformation in a week may abandon a plan that is working exactly as it should (Cridge, 2025). The first question is therefore not "why has this failed", but "how long has it been, and is the line moving at all". This is where logging the numbers earns its keep: tracking the stool and the weight week by week on the Faecal Score Tracker shows you whether the four-week timeline is on track or genuinely stalled, rather than relying on a vague sense of "a bit better". A pet slowly improving needs time, not a new plan.
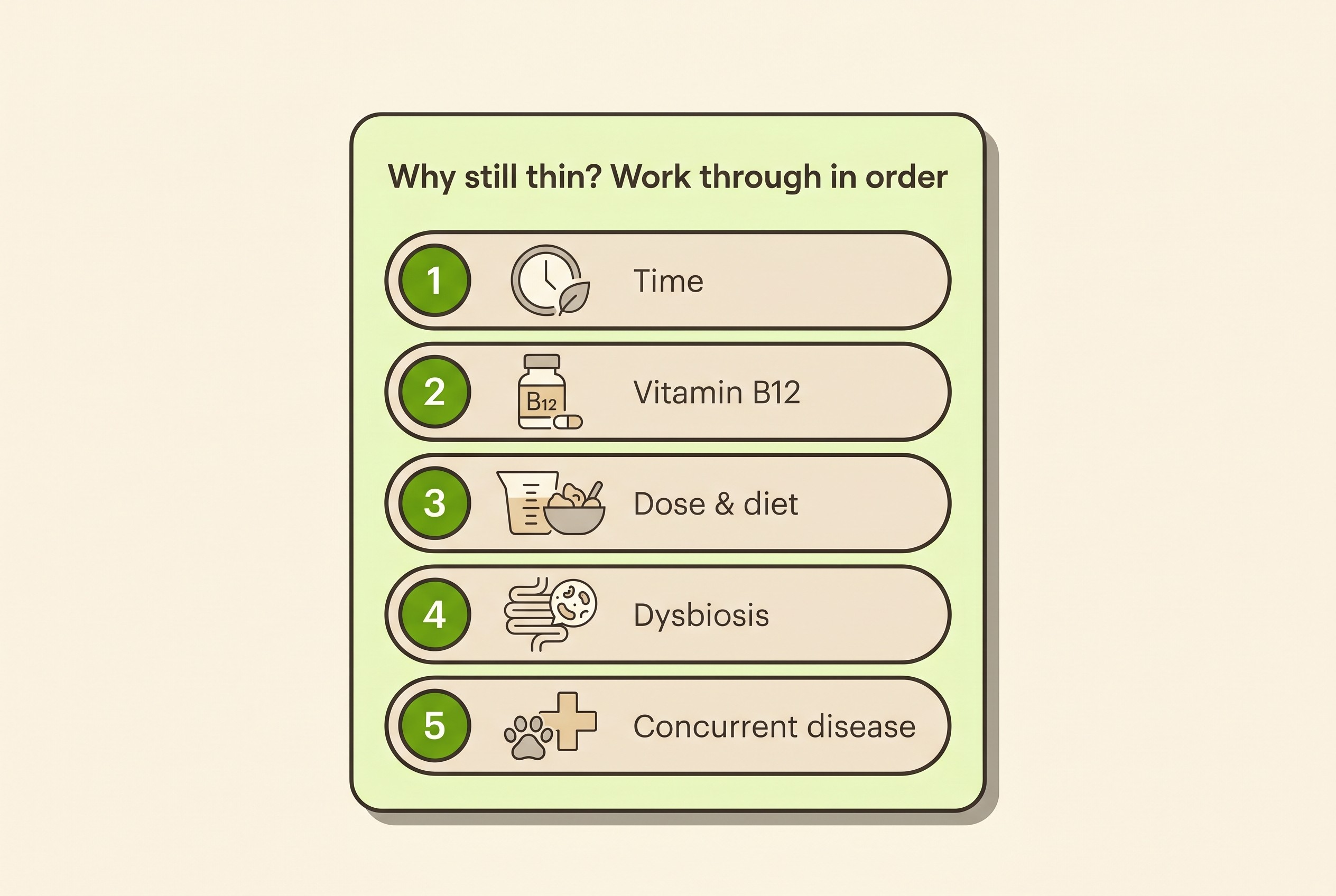
When the line really has flattened despite a fair trial, the modern way to think about it is a short list of fixable reasons rather than a verdict of "refractory": an inadequate timeline, an enzyme dose or formulation issue, an inappropriate diet, persistent small-intestinal dysbiosis, and concurrent disease such as a chronic enteropathy (Cridge, 2025; Cridge et al., 2024). One thread, cobalamin, runs through several of these, so it goes first.
Vitamin B12: the commonest correctable reason, and check it first
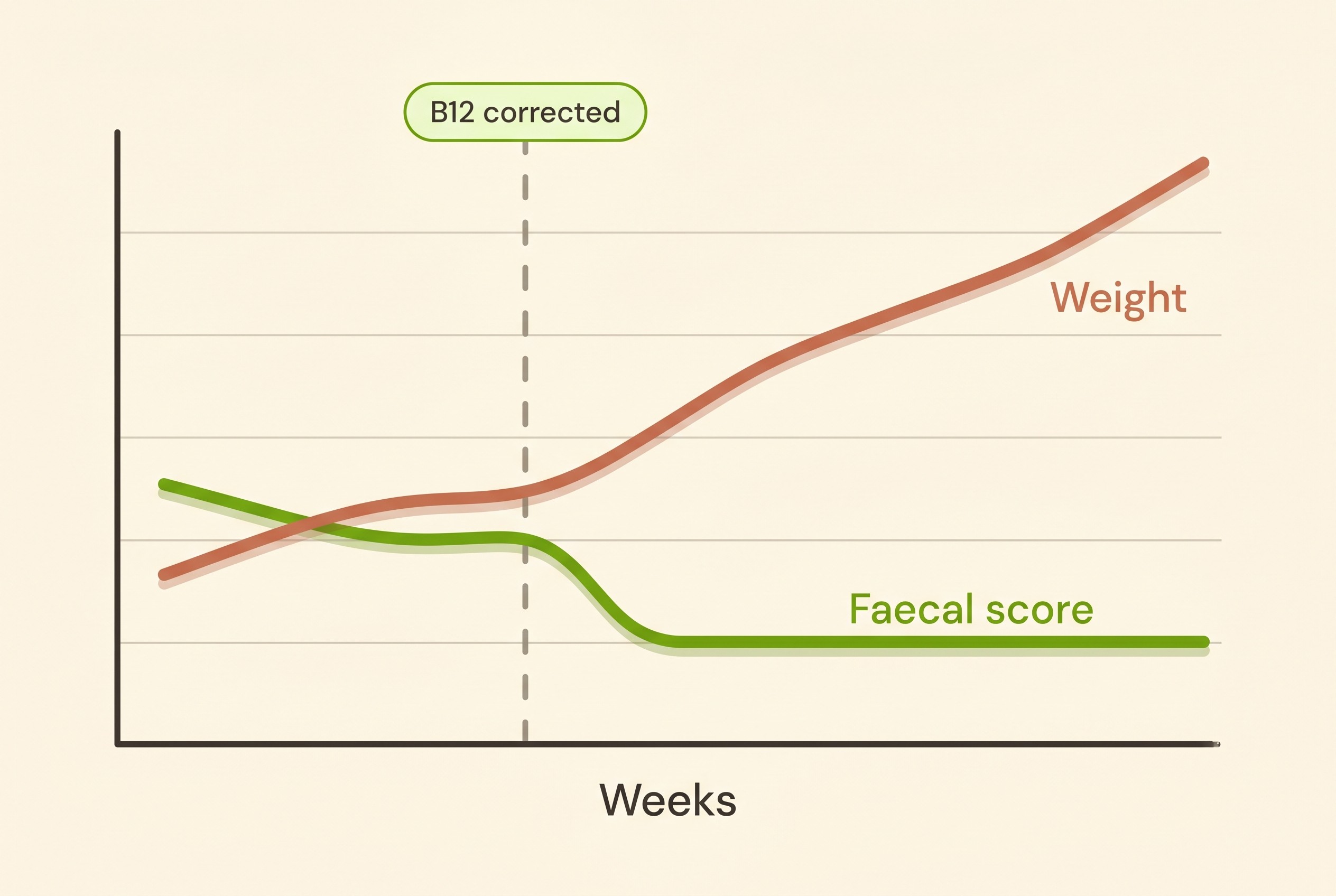
Enzyme supplementation alone may not resolve the signs, and a deficiency of cobalamin (vitamin B12) is the first thing to consider when it does not (MSD Veterinary Manual). The reason is built into the disease: in dogs and cats the pancreas is the main source of the carrier protein needed to absorb B12 from the gut, so when the exocrine pancreas fails, B12 absorption fails alongside it (Batchelor et al., 2007; Cridge, 2025). The full explanation belongs to what EPI is; the point here is that the deficiency is intrinsic to EPI, not an unlucky coincidence.
Checking it is routine, not a niche add-on. Around two-thirds of dogs with EPI have low cobalamin at diagnosis, and roughly three-quarters of cats are deficient (Soetart et al., 2019; Xenoulis et al., 2016). And this is not just about stool. In a large canine cohort, low cobalamin at diagnosis was an independent risk factor for shorter survival (Soetart et al., 2019), an earlier study linked marked deficiency in particular to a worse outcome, and the MSD Veterinary Manual singles out cobalamin deficiency as an independent risk factor for poor outcome in EPI dogs (Batchelor et al., 2007; MSD Veterinary Manual). So a thin EPI pet who will not gain needs its B12 measured and corrected before anything cleverer is tried.
Correcting it is easy and cheap, and one out-of-date assumption is worth retiring on the spot: B12 does not have to be a lifelong weekly injection. Oral cobalamin normalises low levels just as effectively as the injectable form, including in EPI dogs specifically (Chang et al., 2022; Toresson et al., 2016, 2018). The dosing schedule sits with living with chronic enteropathy, so I will hand you there. If your pet's B12 was low and has now been replaced, the Faecal Score Tracker is how you will see whether that correction moved the needle, often the single change that finally lets the weight come. (Your vet may measure folate in the same draw; do not read too much into a high folate alone, as in one large cohort it was linked to a better prognosis, not a worse one (Soetart et al., 2019).)
Dose, compliance and the diet that catches people out
Once B12 is sorted, the next reasons are unglamorous, and very often the real answer.
Start with the dose, which may simply need adjusting. Enzyme requirements vary between individuals, and a dose that is a little too low, or a formulation that is not working for this particular pet, is a common cause of an incomplete response (Cridge, 2025; Szkopek et al., 2024). Raising the dose or changing formulation is a vet-led change; the titration method belongs to managing EPI for life.
Compliance matters just as much, and I raise it without a hint of blame because it is so easy to slip. Enzymes have to go with every meal to work: the treat from a visitor, the snack on a walk, the bowl left by the dog-sitter, every one needs the powder too, or that food largely passes through undigested. A few missed meals a week, or a dose that has quietly crept down because progress felt slow, shows up as a stalled recovery, so it is worth running carefully through a typical week first.
Then there is the diet error I correct more than any other. Owners, and sometimes practices, reach for a very low-fat diet by analogy with pancreatitis, on the mistaken assumption that a sick pancreas means fat must be the enemy. In EPI that backfires: a very low-fat diet can further reduce fat assimilation and is not recommended (MSD Veterinary Manual; Cridge, 2025). The diet that partners the enzymes is a highly digestible one, low in insoluble, non-fermentable fibre, with a moderate amount of fermentable fibre acceptable; high insoluble fibre is the thing to avoid, because it can interfere with enzyme activity and nutrient absorption (Cridge et al., 2024; MSD Veterinary Manual). The low-fat-for-pancreatitis argument lives in low-fat feeding for pancreatitis; I flag it only so the two do not get muddled, because that keeps a lot of EPI pets needlessly thin.
Persistent dysbiosis, and the one place a short antibiotic course earns its keep
This needs care, because it runs against a message you will have read elsewhere on this site. EPI changes the bacterial balance of the small intestine. The extra undigested food in the gut, the loss of the pancreatic juice's antibacterial factors, and altered motility all predispose to a small-intestinal dysbiosis (the term that has largely replaced the older "small intestinal bacterial overgrowth", or SIBO) (MSD Veterinary Manual; Isaiah et al., 2017). This is not hand-waving: the faecal microbiome of EPI dogs is measurably abnormal, with characteristic shifts in bacterial families and a raised dysbiosis index, present in both treated and untreated dogs, so enzymes alone do not fully fix it (Isaiah et al., 2017; Blake et al., 2019).
Now the contrast. For an ordinary, self-limiting tummy upset, antibiotics are usually unnecessary, and metronidazole in particular is now actively discouraged because of that same microbiome cost. That argument is owned by antibiotics for diarrhoea, and I will not re-run it. But a confirmed EPI non-responder with a dysbiotic, antibiotic-responsive component is one of the few places where the opposite holds, and a short, vet-directed course can genuinely help. EPI pets commonly have concurrent dysbiosis and may benefit from antimicrobial therapy, with tylosin the drug carrying the most veterinary support; oxytetracycline has been used historically too (MSD Veterinary Manual; Westermarck & Wiberg, 2012).
Let me be candid about the strength of that evidence, because this is where the field is thin. The controlled evidence for antibiotics as a routine EPI adjunct is limited, which is why they belong to the genuine non-responder and not to every newly diagnosed pet. The supporting biology is real: a chronic, antibiotic-responsive diarrhoea can resolve strikingly on tylosin, though it commonly relapses when the drug stops (Westermarck et al., 2005). But that is a related condition, not proof of automatic benefit in EPI, so the right framing is a defined, time-limited course for a defined problem, decided with your vet. Faecal microbiota transplantation is sometimes raised for refractory cases; treat it as an emerging, specialist frontier rather than a recommendation (MSD Veterinary Manual).
When it is concurrent disease, and when to ask for help
If B12 is corrected, the dose, compliance and diet are all sound, and the pet still will not gain, it is time to ask whether EPI is the whole story. TLI is robust and is not altered by enzyme supplements, so it can be repeated if there is genuine doubt, but more often the diagnosis is right and a second problem is sitting on top of it (Cridge, 2025).
The big one is a concurrent chronic enteropathy (CE). EPI and CE can coexist, and persistent signs despite good enzyme and B12 therapy point towards additional small-intestinal disease, for which abdominal ultrasound and intestinal biopsy may be indicated (MSD Veterinary Manual; Cridge, 2025). If that is the answer, the pet may need the CE step-up, a structured diet trial and, where justified, immunomodulation, on top of EPI management; that pathway is owned by chronic enteropathy treatment, and the food-trial mechanics by the Diet-Trial Companion. In dogs that are not German Shepherds, and in cats, ongoing chronic pancreatitis is often the underlying cause and can keep grumbling beneath the EPI, its own subject in chronic grumbling pancreatitis.
One more vet-directed option is worth knowing for the true non-responder: a trial of a proton pump inhibitor such as omeprazole, on the rationale that excess stomach acid may be inactivating the supplemented enzymes before they can work (MSD Veterinary Manual). It is a reasonable step for a persistent case, not a routine first move.
The order is the point: time, then B12, then dose and compliance and diet, then dysbiosis, then concurrent disease. Work down that list with your vet and the great majority of "stuck" EPI pets turn out not to be stuck at all, just waiting for the one missing piece. If you reach the end of it with the basics sound and the weight still not coming, that is the moment for an internal medicine referral: escalating sensibly, not giving up. Keep the stool and the weight going onto the Faecal Score Tracker as you go, because when the right change finally lands, that slow climb back to a healthy weight is exactly how you will know you have found it.
References
- Batchelor, D. J., Noble, P.-J. M., Taylor, R. H., Cripps, P. J., & German, A. J. (2007). Prognostic factors in canine exocrine pancreatic insufficiency: prolonged survival is likely if clinical remission is achieved. Journal of Veterinary Internal Medicine, 21(1), 54-60.
- Blake, A. B., Guard, B. C., Honneffer, J. B., Lidbury, J. A., Steiner, J. M., & Suchodolski, J. S. (2019). Altered microbiota, fecal lactate, and fecal bile acids in dogs with gastrointestinal disease. PLOS ONE, 14(10), e0224454.
- Chang, C.-H., Lidbury, J. A., Suchodolski, J. S., & Steiner, J. M. (2022). Effect of oral or injectable supplementation with cobalamin in dogs with hypocobalaminemia caused by chronic enteropathy or exocrine pancreatic insufficiency. Journal of Veterinary Internal Medicine, 36(5), 1607-1621.
- Cridge, H. (2025). Canine and feline exocrine pancreatic insufficiency. Today's Veterinary Practice, June 2025.
- Cridge, H., Williams, D. A., & Barko, P. C. (2024). Exocrine pancreatic insufficiency in dogs and cats. Journal of the American Veterinary Medical Association, 262(2), 246-255.
- Isaiah, A., Parambeth, J. C., Steiner, J. M., Lidbury, J. A., & Suchodolski, J. S. (2017). The fecal microbiome of dogs with exocrine pancreatic insufficiency. Anaerobe, 45, 50-58.
- MSD Veterinary Manual. Exocrine pancreatic insufficiency in dogs and cats (current online edition; H. Cridge, reviewer).
- Soetart, N., Rochel, D., Drut, A., & Jaillardon, L. (2019). Serum cobalamin and folate as prognostic factors in canine exocrine pancreatic insufficiency: an observational cohort study of 299 dogs. The Veterinary Journal, 243, 15-20.
- Szkopek, D., Pierzynowski, S. G., Pierzynowska, K., et al. (2024). A review: pancreatic enzymes in the treatment of chronic pancreatic insufficiency in companion animals. Journal of Veterinary Internal Medicine, 38(4), 2026-2033.
- Toresson, L., Steiner, J. M., Suchodolski, J. S., & Spillmann, T. (2016). Oral cobalamin supplementation in dogs with chronic enteropathies and hypocobalaminemia. Journal of Veterinary Internal Medicine, 30(1), 101-107.
- Toresson, L., Steiner, J. M., Razdan, P., Spodsberg, E., Olmedal, G., Suchodolski, J. S., & Spillmann, T. (2018). Comparison of efficacy of oral and parenteral cobalamin supplementation in normalising low cobalamin concentrations in dogs: a randomised controlled study. The Veterinary Journal, 232, 27-32.
- Westermarck, E., Skrzypczak, T., Harmoinen, J., et al. (2005). Tylosin-responsive chronic diarrhea in dogs. Journal of Veterinary Internal Medicine, 19(2), 177-186.
- Westermarck, E., & Wiberg, M. E. (2012). Exocrine pancreatic insufficiency in the dog: historical background, diagnosis, and treatment. Topics in Companion Animal Medicine, 27(3), 96-103.
- Xenoulis, P. G., Zoran, D. L., Fosgate, G. T., Suchodolski, J. S., & Steiner, J. M. (2016). Feline exocrine pancreatic insufficiency: a retrospective study of 150 cases. Journal of Veterinary Internal Medicine, 30(6), 1790-1797.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine