
Managing EPI for life: enzymes with every meal, B12, and getting the dose right
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
"Exocrine pancreatic insufficiency" is a heavy phrase to be handed, and on diagnosis day it can sound like a life sentence. For most owners it turns out to be something much smaller: a feeding habit, settled into by the end of the first month. Once the enzymes are going in and the B12 is topped up, the great majority of these pets do genuinely well (Batchelor et al., 2007; Cridge, 2025).
I will not re-cover what EPI is, the ravenous-but-thin picture, or the serum TLI blood test that confirmed it; if you want that background, EPI explained is the piece for you. The pancreas is no longer making enough digestive enzymes, so food passes through largely undigested, and replacing those enzymes at every meal does its job for it (Westermarck & Wiberg, 2012). The rest is how to do that well.
Enzymes with every single meal: the cornerstone
The treatment is pancreatic enzyme replacement, given with every meal, for the rest of your pet's life. The active ingredient is pancrelipase, and the practical default is a non-enteric-coated powder mixed through the food (Szkopek et al., 2024; Cridge, 2025). The phrase "every meal" is the bit that matters most: a meal eaten without enzymes mostly passes through undigested, so the snack from a visitor and the bowl from the dog-sitter need the powder too. The results are good. In the long-term study that anchors much of our understanding, signs were almost completely controlled in around half of EPI dogs, whose general health then resembled normal dogs, while about one in five responded poorly (Wiberg et al., 1998).
Is powder really good enough, or should you buy something fancier? Non-enteric-coated powder, and even raw chopped pancreas, were equally effective at controlling signs in that same study (Wiberg et al., 1998), and the single randomised head-to-head between enteric-coated micro-pellets and uncoated powder found no significant difference in faecal fat, though with only eleven dogs completing it that means "no clear advantage shown", not proven equivalence (Parambeth et al., 2018). So the reasonable position is: powder first, with enteric-coated capsules a sound second-line option for a refractory case rather than an upgrade worth paying for routinely (Szkopek et al., 2024). Raw pancreas works and can be cheaper, but it carries food-hygiene and supply caveats and is more likely to irritate the mouth, so I treat it as a fallback (Wiberg et al., 1998; Szkopek et al., 2024).

Getting the dose right: titrate down, not up
This is the part owners worry about most. As a starting point, the convention for dogs is roughly one to two teaspoons of powdered enzyme per 10 kg of body weight at each meal, and for cats about half to one teaspoon per meal (Szkopek et al., 2024); some vets prefer a simpler rule of about a teaspoon per cup of food (Cridge, 2025). Read either as an illustration rather than a prescription: products differ in enzyme strength, and your own vet sets the exact dose.
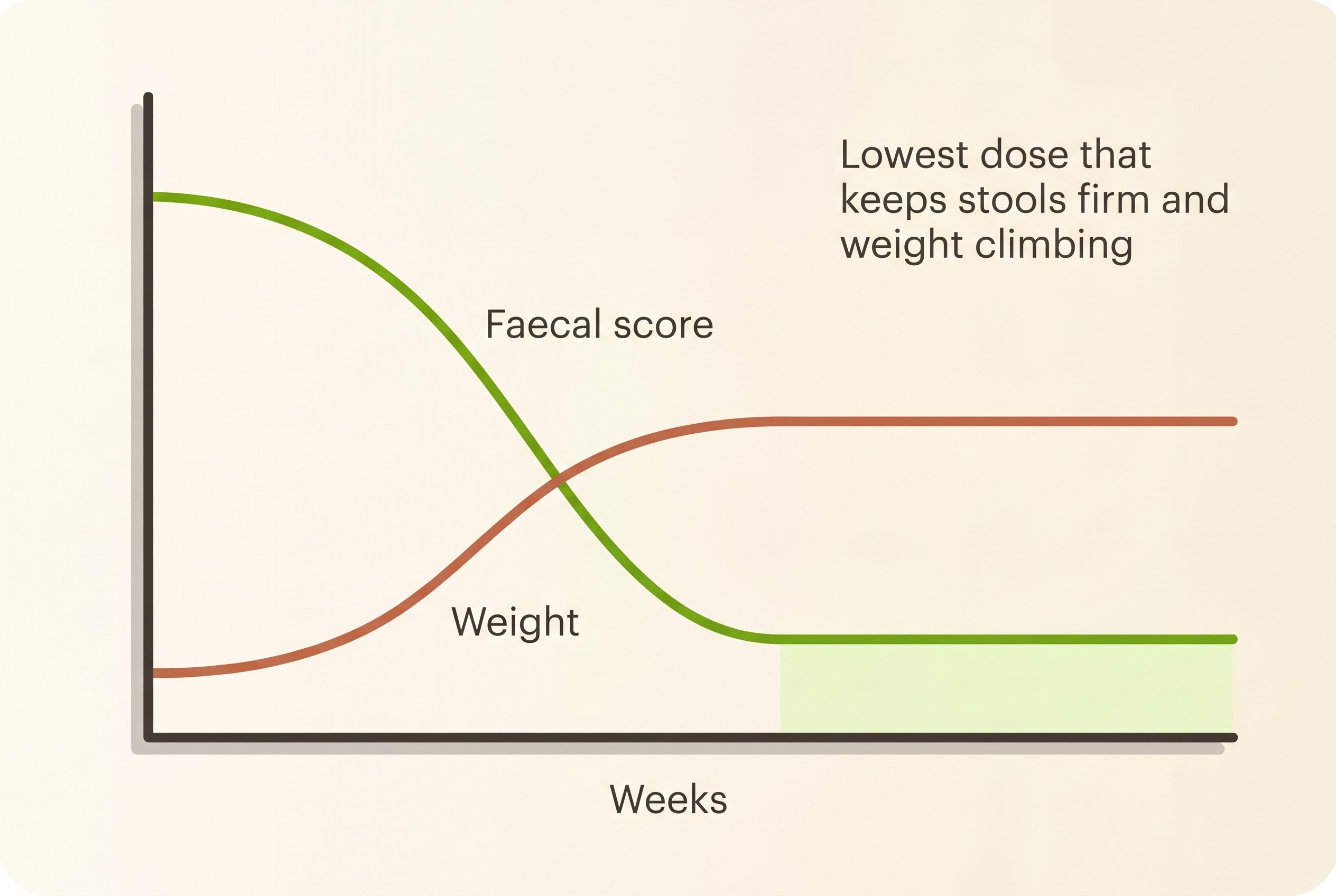
The principle that matters more than any number is this: once signs are under control, you titrate the dose down, not up. Start at the recommended dose, get the stools and weight good, then gradually reduce to the lowest dose that keeps them that way (Szkopek et al., 2024; Westermarck & Wiberg, 2012). That runs against the owner instinct to keep adding powder when progress feels slow, but most dogs do not need large doses, and pushing the dose higher and higher buys very little while costing a great deal and raising the risk of mouth soreness (Szkopek et al., 2024).
So how do you judge the dose? Not by the bag, but by the stool and the weight: the dose is right when the faeces are well-formed and the weight is climbing back to normal (Wiberg et al., 1998; Cridge, 2025). This is exactly where our Faecal Score Tracker earns its place. Think of it as your dosing instrument: you log the stool score and the weight and watch the line settle as the dose finds its level, titrating against a record rather than a vague sense of "a bit better" (the 1-7 chart and how to use it are owned by describing symptoms to your vet). Splitting the day into two or three meals, each with its own enzyme, also helps spread the dose and lets a depleted pet regain condition (Westermarck & Wiberg, 2012).
How to give it, and the folklore to ignore
The method is simple: mix the powder thoroughly through moistened food and feed it (Snead, 2006). Moistening matters mainly because it carries the powder evenly so your pet eats all of it.
Now the folklore, because the internet is full of it. You do not need to pre-incubate the food: letting the enzyme sit on the meal for twenty or thirty minutes before feeding does not improve the response, and neither does adding bile salts, so skip both with a clear conscience (Szkopek et al., 2024; Cridge, 2025). Likewise, you do not routinely need acid-blockers: an H2-blocker or a proton-pump inhibitor such as omeprazole to "protect" the enzymes has not been shown to improve how well they work, so it is usually just extra cost (Szkopek et al., 2024).
The one genuine side effect to know about is mouth soreness. High doses of powdered enzyme, and raw pancreas, can irritate the mouth and occasionally cause ulceration and bleeding, typically blood-tinged saliva or sore gums after meals (Snead, 2006; Szkopek et al., 2024). It is uncommon and clearly dose-related, and the first fix is simple: bring the dose down to the lowest that still controls the signs, mix the powder into moist food rather than offering it dry, and avoid crushing or holding capsules in the mouth (Szkopek et al., 2024). If the gums are already sore, a short course of sucralfate suspension and a chlorhexidine mouth rinse settles things; in the reported case it cleared within a week and had not recurred eight months on (Snead, 2006). It is a fixable nuisance, not a reason to abandon treatment.
Cobalamin (B12) is almost always part of the package
Checking and supplementing B12 is routine, not an extra. The failing pancreas is your pet's main source of intrinsic factor, the molecule needed to absorb cobalamin from the gut, so B12 absorption fails alongside the enzymes. About two-thirds of EPI dogs are deficient, and in cats the figure is higher still, around 77% (Soetart et al., 2019; Xenoulis et al., 2016). It matters: low B12 is one of the fixable reasons a dog will not gain weight despite the enzymes, and marked hypocobalaminaemia at diagnosis is independently associated with shorter survival (Batchelor et al., 2007; Soetart et al., 2019). In cats it is so central that supplementing it made them about three times as likely to respond well (Xenoulis et al., 2016).
One piece of out-of-date advice is worth correcting: B12 does not have to be a monthly injection. Oral cobalamin works at least as well as the injectable form, including in EPI dogs specifically, so a daily tablet is a perfectly good and cheaper route for most pets (Chang et al., 2022; Toresson et al., 2016, 2018). It is usually started when serum cobalamin is low or low-normal, a common threshold being around 400 ng/L (Cridge, 2025). The dosing schedule, and when to re-check and taper, belongs with living with chronic enteropathy, so I will hand you there for the regimen.
The diet that partners the enzymes, and the pancreatitis trap
The standard dietary partner to the enzymes is a highly digestible, low-residue diet, the type your vet may call a gastrointestinal or "GI" diet (Cridge, 2025; Szkopek et al., 2024). The logic is simple: high digestibility means more of the now enzyme-treated food is absorbed.
The correction I most often have to make is this: EPI is not pancreatitis. Because pancreatitis gets all the dietary press, owners very reasonably assume their EPI pet should go on a low-fat diet. In fact, with adequate enzymes, fat does not need to be restricted in most EPI dogs, and it should not be restricted in cats; over-restricting it simply strips calories from an animal that is often thin and badly needs them (Cridge, 2025; Szkopek et al., 2024). A minority of dogs with stubborn, greasy stools despite optimised enzymes do settle better with some fat moderation, so the better framing is "led by your pet's response, not a blanket low-fat rule" (Cridge, 2025). Low-fat feeding is its own topic, owned by low-fat feeding for pancreatitis; I flag it only so the two do not get muddled. High-fibre diets are best avoided too: excess fibre can interfere with enzyme activity, and high-fibre foods tend to be lower in calories than a thin pet can afford (Cridge, 2025; Szkopek et al., 2024). The default, then, is highly digestible, calorie-dense, and not high in fibre.
What good control looks like, and how long it takes
Set your expectations realistically and you will not panic in week one. Stool quality usually improves over up to about four weeks on enzymes and the right diet, while body condition can take several months to recover fully, so your pet will not transform overnight (Cridge, 2025). Well-controlled looks like well-formed faeces that are no longer greasy, bulky or pale, a steady climb back to a healthy weight, the ravenous edge settling, and energy and coat returning (Wiberg et al., 1998; Cridge, 2025). Your tracker line is the proof.
The prognosis to hold onto is a good one. Treated dogs that get through the early period have a median survival of around 1,919 days, comfortably over five years, and prolonged survival is likely once remission is achieved (Batchelor et al., 2007). The sobering other side of that figure is that roughly one in five dogs are lost or euthanised in the first year, very often the ones who do not respond well early (Batchelor et al., 2007), which is exactly why getting the dose, the B12 and the diet right from the start matters so much. If your pet eats enzymes faithfully and still will not gain weight, do not give up and do not just pile on more powder: there are fixable reasons, and why the weight still will not come walks through every one of them.
Keeping it affordable, and the daily rhythm
There is no pretending the cost away: lifelong enzyme replacement is the main ongoing expense, and a genuine worry. Helpfully, the biggest saving is also the clinically correct move, titrating to the lowest effective dose rather than over-supplementing (Szkopek et al., 2024). Buying powder in bulk helps too, raw pancreas is cheaper where it can be sourced and handled safely, and oral B12 spares the running cost of repeat injections (Chang et al., 2022).
Once your routine is settled, the whole thing comes down to a small daily rhythm: powder in every bowl, B12 on board, a digestible diet, and the Faecal Score Tracker and the scales telling you the dose is right. If your EPI pet ever becomes acutely unwell, treat them like any sick pet and use the Vomiting & Diarrhoea Triage to judge whether it needs a same-day call. But for most owners, most of the time, the story from here is a quietly good one: a normal-looking dog or cat, and many good years ahead.
References
- Wiberg ME, Lautala H-M, Westermarck E. (1998) Response to long-term enzyme replacement treatment in dogs with exocrine pancreatic insufficiency. Journal of the American Veterinary Medical Association 213(1):86-90.
- Westermarck E, Wiberg ME. (2012) Exocrine pancreatic insufficiency in the dog: historical background, diagnosis, and treatment. Topics in Companion Animal Medicine 27(3):96-103.
- Batchelor DJ, Noble P-JM, Taylor RH, Cripps PJ, German AJ. (2007) Prognostic factors in canine exocrine pancreatic insufficiency: prolonged survival is likely if clinical remission is achieved. Journal of Veterinary Internal Medicine 21(1):54-60.
- Szkopek D, Pierzynowski SG, Pierzynowska K, et al. (2024) A review: pancreatic enzymes in the treatment of chronic pancreatic insufficiency in companion animals. Journal of Veterinary Internal Medicine 38(4):2026-2033.
- Cridge H. (2025) Canine and Feline Exocrine Pancreatic Insufficiency. Today's Veterinary Practice (July/August 2025)
- Parambeth JC, Fosgate GT, Suchodolski JS, Lidbury JA, Steiner JM. (2018) Randomized placebo controlled clinical trial of an enteric coated micro-pelleted formulation of a pancreatic enzyme supplement in dogs with exocrine pancreatic insufficiency. Journal of Veterinary Internal Medicine 32(5):1591-1599.
- Snead E. (2006) Oral ulceration and bleeding associated with pancreatic enzyme supplementation in a German shepherd with pancreatic acinar atrophy. Canadian Veterinary Journal 47(6):579-582.
- Chang C-H, Lidbury JA, Suchodolski JS, Steiner JM. (2022) Effect of oral or injectable supplementation with cobalamin in dogs with hypocobalaminemia caused by chronic enteropathy or exocrine pancreatic insufficiency. Journal of Veterinary Internal Medicine 36(5):1607-1621.
- Toresson L, Steiner JM, Suchodolski JS, Spillmann T. (2016) Oral cobalamin supplementation in dogs with chronic enteropathies and hypocobalaminemia. Journal of Veterinary Internal Medicine 30(1):101-107. AND Toresson L, Steiner JM, Olmedal G, et al. (2018) Comparison of efficacy of oral and parenteral cobalamin supplementation in normalising low cobalamin concentrations in dogs: a randomised controlled study. The Veterinary Journal 232:27-32.
- Xenoulis PG, Zoran DL, Fosgate GT, Suchodolski JS, Steiner JM. (2016) Feline exocrine pancreatic insufficiency: a retrospective study of 150 cases. Journal of Veterinary Internal Medicine 30(6):1790-1797.
- Soetart N, Rochel D, Drut A, Jaillardon L. (2019) Serum cobalamin and folate as prognostic factors in canine exocrine pancreatic insufficiency: an observational cohort study of 299 dogs. The Veterinary Journal 243:15-20.
- Exocrine Pancreatic Insufficiency in Dogs and Cats. MSD/Merck Veterinary Manual (current online edition; H. Cridge, author/reviewer)
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine