
Getting the Diagnosis: How Vets Confirm Diabetes
Claire Greenway
BVM&S MRCVS
Most owners arrive at the diagnosis the same way. Something had been off for a few weeks: the water bowl emptying too fast, puddles where there had never been puddles, weight sliding off despite a hearty appetite. A sample went off, and now there's a word on the page. Let me walk you through how we confirm it and, above all, why we don't hang a diagnosis this serious on a single high number.
That last point is the heart of this page, and it's the bit the generic websites skip: a diagnosis is not "the glucose was high, therefore diabetes," and in cats especially there is a genuine trap waiting for anyone who reads one number and jumps. If you'd like the underlying biology first, what diabetes actually is is the companion piece.
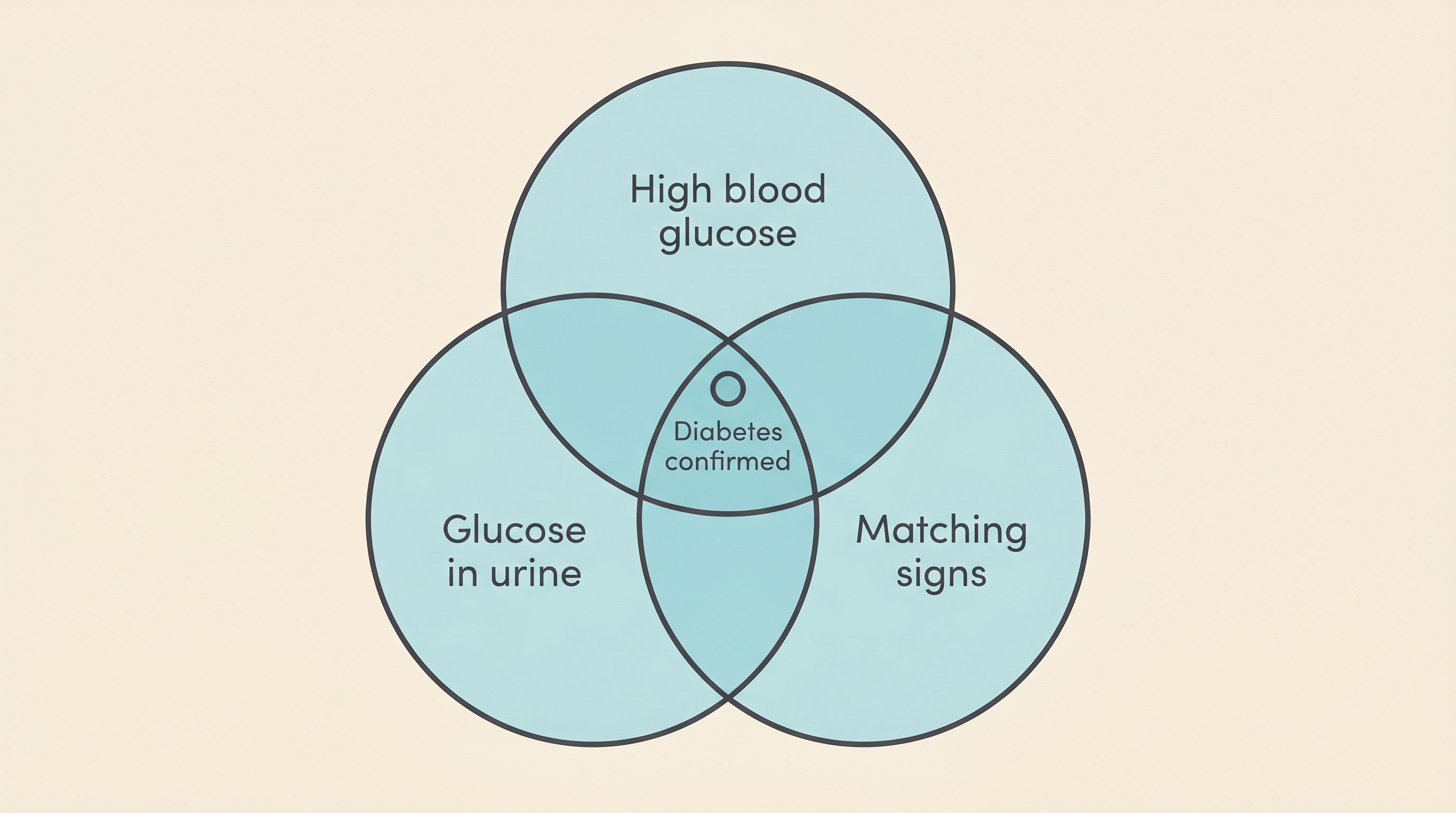
Three things lining up, not one test
A vet doesn't diagnose diabetes on one finding. We diagnose it on three things lining up together: a blood glucose that is persistently high, glucose spilling into the urine, and clinical signs that fit, the classic combination of increased thirst and urination with weight loss despite a good or even ravenous appetite (Behrend et al., 2018; Taylor et al., 2025). Any one alone is a flag, not a diagnosis, because each has innocent explanations: a high glucose can be fleeting and stress-driven, particularly in a cat, and glucose in the urine confirms only that the blood level has been running high at some point. Stack the three together, though, and the diagnosis becomes secure.
Why glucose shows up in the urine at all explains why your vet wants both samples. The kidney reclaims glucose up to a ceiling, the renal threshold: below it the urine stays clean, above it the excess spills over. That ceiling sits at around 10 mmol/L (roughly 180 mg/dL) in dogs and higher in cats, around 15 mmol/L (Taylor et al., 2025; MSD/Merck Veterinary Manual). So glucosuria isn't a measurement, it's a lagging flag that the blood glucose has been running high.
When a single high reading lies, especially in a cat
This is the point I most want to land, and the reason I'd gently push back on any diagnosis made on one in-clinic reading alone. In cats, fear itself can drive the blood glucose up, sometimes dramatically, with nothing to do with diabetes. It's called stress hyperglycaemia, and it is no minor wobble. A cat struggling against restraint can raise its own glucose by as much as 10 mmol/L (around 180 mg/dL) on stress alone, and even a short stressor moves it fast: in one experiment a five-minute spray-bath pushed glucose up by an average of 4.1 mmol/L within ten minutes, and as much as 10.8 mmol/L in some individuals (Rand, WSAVA 2017). So a perfectly non-diabetic cat, frightened by the carrier and the clinic, can walk in with a glucose well up into diabetic territory on stress alone.
This matters enormously, because treating that single high reading as proof would mean starting insulin in a cat that doesn't need it. So here is the guardrail: never let one in-clinic glucose stand alone in a cat. The elevation usually settles within about ninety minutes, but not always; in one study 8 of 20 cats were still above baseline at that point (Rand, WSAVA 2017). If a screening glucose comes back high, the feline guidelines are clear: retest a few hours later from a low-stress sample, or sidestep the problem with glucose measured at home, a continuous sensor, or a home-collected urine sample, since stress hyperglycaemia "can be of any magnitude" (Taylor et al., 2025).
Dogs, I should say, very rarely get clinically meaningful stress hyperglycaemia, so this is overwhelmingly a cat problem (feline diabetes explained covers the wider feline picture). Glucose logged at home is genuinely useful for confirming a borderline cat, and the Glucose Companion gives you somewhere to keep those readings. One small caution if you do measure at home: human glucometers tend to read pet blood low, so a pet-calibrated meter or a continuous sensor gives a truer picture, and the figure still belongs in a conversation with your vet rather than a snap decision.
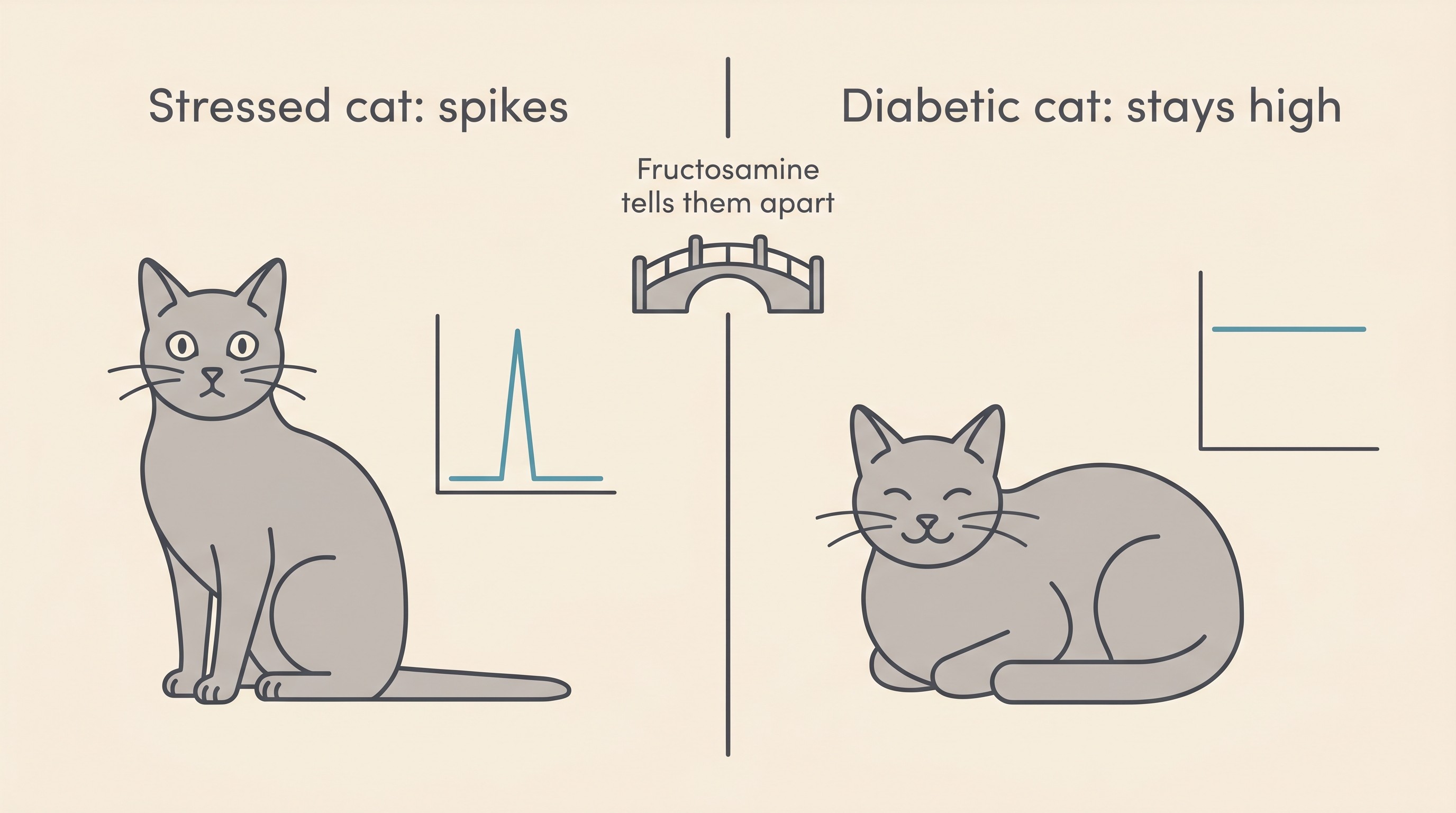
Fructosamine, the test that ignores the last hour
So how do we tell the genuinely diabetic cat from the merely terrified one? With a blood test that doesn't care about the last hour at all: fructosamine, the quiet hero of feline diabetes diagnosis. It is glucose irreversibly bound to the blood proteins, mainly albumin. Because those proteins turn over slowly, it reflects the average blood glucose over roughly the previous one to three weeks, or as the feline guidelines put it, "the preceding 7 to 10 days or so" (Taylor et al., 2025; IDEXX UK). The beautiful part is that a single spike of waiting-room stress is far too brief to move it. The classic study, nearly thirty years ago, found cats with stress hyperglycaemia had a median fructosamine of 269 µmol/L, no different from clinically normal cats at 252, while untreated diabetic cats sat far higher at 624 (Crenshaw & Peterson, 1996). That clean separation is why your vet reaches for it. As a rough UK guide, reference intervals run around 137 to 286 µmol/L in cats and 177 to 314 in dogs, but these are laboratory-specific, so only compare results from the same analyser (IDEXX UK).
Fructosamine has its limits, though. It can read normal in early or mild diabetes, before enough time at high glucose has dragged the average up (Taylor et al., 2025). And anything that speeds up protein turnover pulls it down even in a genuinely diabetic animal: in uncontrolled hyperthyroid diabetic cats the average was 332 µmol/L, inside the normal reference interval, against 527 µmol/L in diabetic cats with normal thyroids (Gal et al., 2017), so a "normal" fructosamine doesn't automatically rule out diabetes in a hyperthyroid cat. It is one piece of the picture, never read alone, and its other job, tracking control over time, belongs to fructosamine and the vet rechecks.
There is now a standardised feline rule that captures all of this (Taylor et al., 2025): the higher and more clear-cut the glucose (at or above about 15 mmol/L, also roughly where it spills into urine), the less corroboration we need, while in the grey zone between roughly 7 and 15 mmol/L you need the classic signs plus a raised fructosamine or repeatable home glucosuria to separate true diabetes from stress. You needn't memorise the cut-offs; the principle is the one I keep returning to: one number is never the diagnosis.
Ketones and the urine: a safety screen, not just confirmation
When that first urine sample is examined, your vet is checking for more than glucose. They are also looking for ketones, often in the blood too. Ketones are what the body produces when, starved of usable glucose, it burns fat for fuel, and they are the warning sign for diabetic ketoacidosis, or DKA, the genuine diabetic emergency. Finding them at diagnosis changes the plan entirely, from "start insulin and manage at home" to "stabilise in hospital first," which is exactly why the screen happens up front. This is no remote possibility: in a 2025 study of 144 newly diagnosed diabetic cats, 44.0% had raised blood ketones and 13.9% had a reported DKA complication, with a third of the most markedly ketotic cats not yet started on insulin (Guse et al., 2025). DKA can be present at the very first visit, before anyone has given a single dose.
DKA has its own full guide, diabetic ketoacidosis, so I'll keep this to the red flag: a diabetic pet who stops eating, vomits, or becomes lethargic and clearly unwell is a same-day emergency, not a wait-and-see.
Running the full bloods, and why
A diabetes work-up is more than a glucose strip and a urine dip. At diagnosis we typically take a full blood count, a biochemistry profile, a complete urinalysis and often a blood pressure (Behrend et al., 2018; Taylor et al., 2025). That database does two jobs beyond confirming the diabetes: it rules out the look-alikes, since thirst, urination and weight loss are not unique to diabetes, and it finds concurrent illness that complicates the picture or fights the insulin once we start it. This is not hypothetical: in that same series of 144 diabetic cats, 63.1% had at least one comorbidity at diagnosis, with pancreatitis the commonest single diagnosis (markers suggestive of it were raised in over half the cats), alongside suspected acromegaly in 17.5% and hyperthyroidism in 5.8% (Guse et al., 2025). So "running the full bloods" isn't padding the bill, it's checking for anything that changes the plan. The closer look at those resistance-causing diseases lives in the concurrent diseases that fight your insulin.
One nuance that surprises owners: diabetics are prone to silent urinary infections, but the modern evidence does not support culturing every diabetic's urine reflexively. In 107 diabetic dogs, only 15 (14%) had a positive culture, and routine culturing wasn't warranted without urinary signs, pus cells or an active sediment (Nelson et al., 2023). So your vet looks closely and cultures when there's a reason to.
What the first numbers do, and don't, tell you
It's tempting to read those first results as a verdict on how bad things are. They aren't, quite. The opening glucose and fructosamine confirm that your pet is diabetic and show roughly how high things have been running, but they don't predict how well your pet will respond, what dose they'll settle on, or, for a cat, whether remission is on the cards. Those answers come from the weeks ahead, from monitoring and gentle adjustment, not from day one. The first figures are a starting point, not a forecast.
The diagnosis also lands differently by species: a diabetic dog is insulin-dependent for life, whereas a diabetic cat may have a window in which good, early management tips them into remission, off insulin altogether, which is part of why we move promptly. Same triad, two diseases, and that contrast gets its own treatment in the same word, two different diseases. For reassurance, this is a condition vets diagnose routinely, roughly one cat in 200 and a quarter of a percent of UK dogs over the age of three (O'Neill et al., 2016; Heeley et al., 2020). You are not in uncharted territory, and while a diabetes diagnosis is a real commitment of time and routine, it is genuinely not a death sentence.
So what now? With the diagnosis confirmed, the ketone screen clear and the baseline database checked, the next step is starting treatment, and that is far less frightening than it feels tonight. The very first insulin injection, the thing looming largest in your mind, is broken down calmly and step by step in your first injection. The work of confirming what you're dealing with is done, and the work of treating it, which most owners find far more manageable than they feared, gets easier from here.
References
- Behrend, E., Holford, A., Lathan, P., Rucinsky, R., & Schulman, R. (2018). 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 54(1), 1-21.
- Crenshaw, K. L., Peterson, M. E., Heeb, L. A., Moroff, S. D., & Nichols, R. (1996). Serum fructosamine concentration as an index of glycemia in cats with diabetes mellitus and stress hyperglycemia. Journal of Veterinary Internal Medicine, 10(6), 360-364.
- Gal, A., Trusiano, B., French, A. F., Lopez-Villalobos, N., & MacNeill, A. L. (2017). Serum fructosamine concentration in uncontrolled hyperthyroid diabetic cats is within the population reference interval. Veterinary Sciences, 4(1), 17.
- Guse, B., Langenstein, J., Bauer, N., & Hazuchova, K. (2025). Signalment, clinicopathological findings, management practices and comorbidities in cats with diabetes mellitus in Germany: cross-sectional study of 144 cases. Journal of Feline Medicine and Surgery, 27(1), 1098612X241303303.
- Heeley, A. M., O'Neill, D. G., Davison, L. J., Church, D. B., Corless, E. K., & Brodbelt, D. C. (2020). Diabetes mellitus in dogs attending UK primary-care practices: frequency, risk factors and survival. Canine Medicine and Genetics, 7, 6.
- IDEXX Reference Laboratories UK. Canine and feline fructosamine reference intervals.
- MSD/Merck Veterinary Manual. Diabetes mellitus in dogs and cats (professional edition).
- Nelson, V., Downey, A., Summers, S., & Shropshire, S. (2023). Prevalence of signs of lower urinary tract disease and positive urine culture in dogs with diabetes mellitus: A retrospective study. Journal of Veterinary Internal Medicine, 37(2), 550-555.
- O'Neill, D. G., Gostelow, R., Orme, C., Church, D. B., Niessen, S. J. M., Verheyen, K., & Brodbelt, D. C. (2016). Epidemiology of diabetes mellitus among 193,435 cats attending primary-care veterinary practices in England. Journal of Veterinary Internal Medicine, 30(4), 964-972.
- Rand, J. (2017). How I avoid stress hyperglycemia confounding glucose measurement in cats. WSAVA World Congress 2017 Proceedings (VIN).
- Taylor, S., Cannon, M., Church, D., Fleeman, L., Fracassi, F., Gilor, C., Mott, J., & Niessen, S. (2025). 2025 iCatCare consensus guidelines on the diagnosis and management of diabetes mellitus in cats. Journal of Feline Medicine and Surgery, 27(11), 1098612X251399103.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing diabetes mellitus. Free to join.
Join PetsLikeMine