
Getting the diagnosis: why atopy is what is left when everything else is ruled out
Dr. Alastair Greenway
MRCVS
Atopic dermatitis is the one allergy diagnosis that no single test can confirm. There is nothing to find on a slide or in a blood tube. Instead, a vet arrives at it by carefully subtracting everything else that itches the same way, until what is left, matching the right pattern, is atopy. So when you are told your pet "probably has atopy" and nobody has run a test that proves it, you have not been fobbed off. You have been told the honest truth about how this diagnosis works. This article is about that logic, because once you see it, the slow work-up stops feeling like nothing is happening and starts looking like exactly what it is: the diagnosis being made step by step.
We assume here that you already know roughly what atopy is, an inherited overreaction to everyday environmental things like pollens and house-dust mites, and that itch is a symptom with a short list of causes this whole space walks you through. This piece owns the next question: how do you actually pin it down?
No single test, and that is not a gap in the science
Most owners are never told this part plainly, so here it is. There is no confirmatory test for canine atopic dermatitis. The diagnosis is clinical: it rests on a compatible history and a recognisable clinical pattern, plus the deliberate exclusion of the other diseases that mimic it (Hensel et al., 2015; Banovic, 2018). The international consensus guideline puts it in almost exactly those words, that the diagnosis "is based on meeting clinical criteria and ruling out other possible causes with similar clinical signs" (Hensel et al., 2015). A widely used practitioner review is blunter still: atopic dermatitis "should never be diagnosed until diseases that resemble it ... have been ruled out" (Banovic, 2018).
That is why a quick "allergy test" cannot short-circuit the process, and we will come back to where those tests genuinely earn their keep. For now, hold the central idea: a diagnosis of exclusion is not a weaker diagnosis. It is the right one for a disease with no fingerprint of its own.
Favrot's criteria: a pattern-recognition aid, not a scorecard
Vets do not work entirely from instinct. There is a recognised set of clinical features that, taken together, make atopy more or less likely. The most-used version comes from a large prospective study by Favrot and colleagues, who looked at a geographically widespread population of itchy dogs and worked out which features best separated the atopic ones from the rest (Favrot et al., 2010). The criteria they derived reach a sensitivity and specificity in the region of 80 to 85% and 79 to 85% respectively, out-performing the older criteria that came before them (Favrot et al., 2010).
The commonly reproduced checklist has eight features, and a dog meeting at least five of them is, on the balance of probability, atopic, at roughly 80% sensitivity and specificity (Banovic, 2018). Presented as the guide they are and not the test they are not, those eight features are (Banovic, 2018; Favrot et al., 2010):
- Onset of signs before three years of age
- A dog that lives mostly indoors
- Itch that responds to steroids (glucocorticoid-responsive pruritus)
- Itch with no visible lesions to start with (the scratching comes before the rash)
- Affected front feet
- Affected ear flaps (pinnae)
- Ear margins that are not affected
- The rump and lower back (dorsolumbar area) not affected
Now for the bit that competitor pages quietly drop. No cut-off on this list is perfect, and the trade-off proves it. Tighten the threshold to six criteria met instead of five and you make a positive result more trustworthy (specificity rises to around 94%), but you miss far more atopic dogs (sensitivity falls to roughly 42%) (Favrot et al., 2010). There is no setting that catches every atopic pet without also flagging some that are not. That is precisely why these criteria support a diagnosis but never replace the ruling-out. Resist any page, or any product, that presents "five of eight equals atopy" as a verdict. It is a starting point for suspicion, not a finish line.
Notice too that several criteria are defined by what is not affected, and those absences are doing real diagnostic work. Itchy ear margins point instead towards sarcoptic mange; an itchy rump and tail base points towards flea allergy (Hensel et al., 2015; Banovic, 2018). The checklist is, in part, a built-in differential: it is quietly steering you away from the conditions that copy atopy. The detail of those rivals belongs to their own articles, but the logic of why their absence matters lives right here.
One caveat worth naming. Favrot's criteria were derived and validated in dogs (Favrot et al., 2010). They are a canine tool. Cats reach the same destination by the same principle of exclusion, but not by this list, so we hand the feline specifics to feline atopic syndrome (Santoro et al., 2021) rather than pretend the checklist applies to a cat.
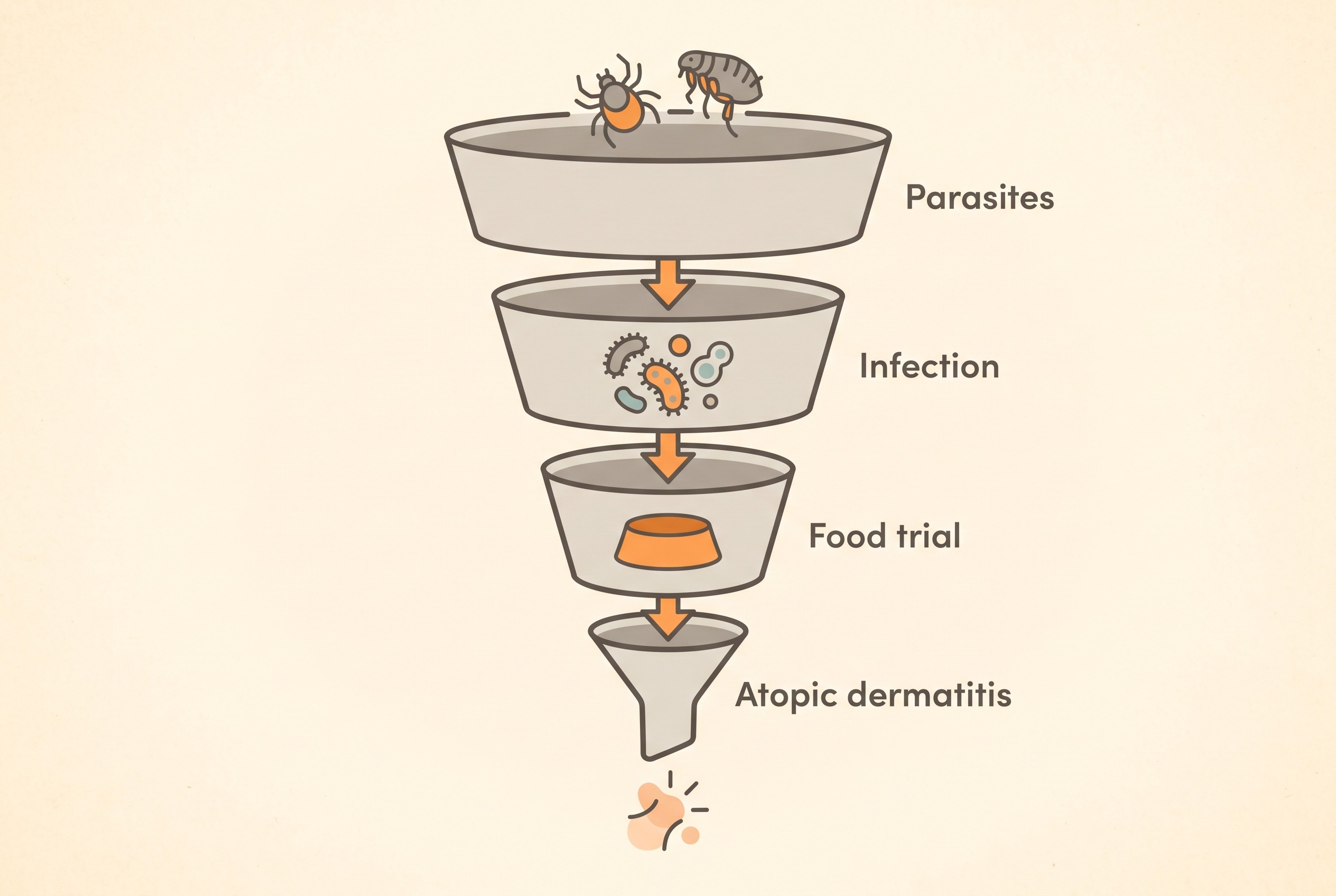
The exclusion steps, in the order they actually happen
What follows is the subtraction, in the sequence a careful vet tends to follow. Each step is brief on purpose, because each one is owned in full by a sibling article.
One: rule out parasites, especially fleas. Rigorous, complete flea control on every pet in the household and in the environment, plus skin scrapes or a treatment trial where the pattern fits mites (Hensel et al., 2015). Flea allergy is the cheapest mimic to treat and the most often missed, which is exactly why it goes first. The mechanism, the "one bite is enough" story, is handled in flea allergy dermatitis.
Two: find and treat any secondary infection. Bacterial infection (mostly Staphylococcus pseudintermedius) and Malassezia yeast ride on top of allergic skin and inflate the itch, and simple cytology finds them (Hensel et al., 2015). Clearing them is part of the work-up for two reasons: they confound the picture, and an untreated infection is a classic reason a diagnosis or a treatment later looks like it "failed" when it did no such thing. The detail sits in skin and ear infections.
Three: exclude a food driver with a strict elimination diet. This step matters especially for year-round signs, or where there are tummy upsets alongside the skin (Hensel et al., 2015). The only reliable way to do it is a strict elimination diet of adequate length: a minimum of about six weeks, with some dogs still improving out to eight or ten weeks (Banovic, 2018). We will not teach the diet mechanics here; the how-to lives in the elimination diet done properly, and the Elimination-Diet Companion is built to run the strict trial without the slip-ups that quietly invalidate it.
Four: what is left, with a compatible pattern, is atopic dermatitis. With parasites out, infection cleared and a food driver excluded, a pet still itching in the classic pattern is atopic. There is a subtlety worth knowing here: food-induced and non-food-induced atopic dermatitis look clinically identical (Favrot et al., 2010). That is exactly why the diet trial is part of the atopy work-up rather than a separate errand, and why a fair number of atopic pets turn out to have a food component tucked inside the same picture.
A practical aside ties the steps together. Tracking an itch score through each stage is how you actually see whether flea control, infection treatment or the diet trial moved the needle, and that trend is the data the diagnosis is built on. The Skin & Itch Tracker plots it for you, so "is she any better?" becomes a line on a chart rather than a guess. It also speaks to the steroid criterion: a clear before-and-after dip when steroids are trialled is "glucocorticoid-responsive pruritus" made visible.
Where allergy testing actually fits (and where it does not)
This is the single most common point of confusion, so let us clear it up. A blood (serum IgE) test or an intradermal skin test does not diagnose atopic dermatitis. Their job comes after a clinical diagnosis is made: to work out which specific allergens a confirmed-atopic pet reacts to, so an immunotherapy formula can be tailored to them (Hensel et al., 2015; Banovic, 2018). A positive blood result in a pet that has not been worked up means very little on its own, because perfectly healthy, non-allergic dogs carry circulating allergen-specific IgE too (Hensel et al., 2015). The full argument about what each test is for, and which kits are worthless, belongs to allergy tests that work and the ones that waste your money. One sentence on the worst of them: an independent study submitted fake fur and plain water to a direct-to-consumer hair and saliva kit and still got "positive" allergen results back, with reproducibility no better than chance, so it cannot diagnose anything (Coyner and Schick, 2019).
A negative test does not clear allergy
There is a second, independent reason the diagnosis stays clinical. A meaningful minority of dogs, commonly cited as around 10%, have disease that is identical to atopic dermatitis in every clinical respect, yet show no demonstrable IgE response to environmental allergens on testing. This is recognised in its own right and called "atopic-like dermatitis" (Halliwell, 2006). It happens because the pet may react to allergens not on the test panel, or by routes that do not produce detectable IgE. The upshot for an owner is simple and important: your pet can be genuinely, classically atopic and still test negative. Most pharma-adjacent pages skip this because it complicates the tidy "test equals answer" pitch.
What a confident diagnosis actually unlocks
Reaching a clear clinical diagnosis is not a dead end, it is a gate. It rules the dangerous and the curable mimics in or out, it tells you whether a food trigger is in the mix, and it is the thing that opens the door to immunotherapy, the only treatment that targets the underlying disease, because the allergen testing that guides it only makes sense once atopy is confirmed (Hensel et al., 2015). The patience the work-up demands is what buys you a real plan, and for many pets a route to needing less firefighting as the months go on.
So the slow exclusion was never the vet stalling. It was the diagnosis being earned. With it in hand, the question changes from "what is wrong?" to "what do we do about it?", and building the treatment toolkit is where that plan begins.
References
- Favrot C, Steffan J, Seewald W, Picco F. A prospective study on the clinical features of chronic canine atopic dermatitis and its diagnosis. Veterinary Dermatology. 2010 Feb;21(1):23-31.
- Hensel P, Santoro D, Favrot C, Hill P, Griffin C. Canine atopic dermatitis: detailed guidelines for diagnosis and allergen identification. BMC Veterinary Research. 2015;11:196. (ICADA guideline.)
- Halliwell R. Revised nomenclature for veterinary allergy. Veterinary Immunology and Immunopathology. 2006 Dec;114(3-4):207-208.
- Coyner K, Schick A. Hair and saliva test fails to identify allergies in dogs. Journal of Small Animal Practice. 2019 Feb;60(2):121-125..)
- Banovic F. Canine atopic dermatitis: updates on diagnosis and treatment. Today's Veterinary Practice. 2018 Jan/Feb. (Practitioner review, peer-edited.)
- Santoro D, Pucheu-Haston CM, Prost C, Mueller RS, Jackson H. Clinical signs and diagnosis of feline atopic syndrome: detailed guidelines for a correct diagnosis. Veterinary Dermatology. 2021;32(1):26-e6. AND Halliwell R, Banovic F, Mueller RS, Olivry T. Feline allergic diseases: introduction and proposed nomenclature. Veterinary Dermatology. 2021;32(1):8-e2.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing allergies & skin. Free to join.
Join PetsLikeMine