
Mites and mange: demodex, sarcoptic scabies and the itch that is not an allergy
Dr. Alastair Greenway
MRCVS
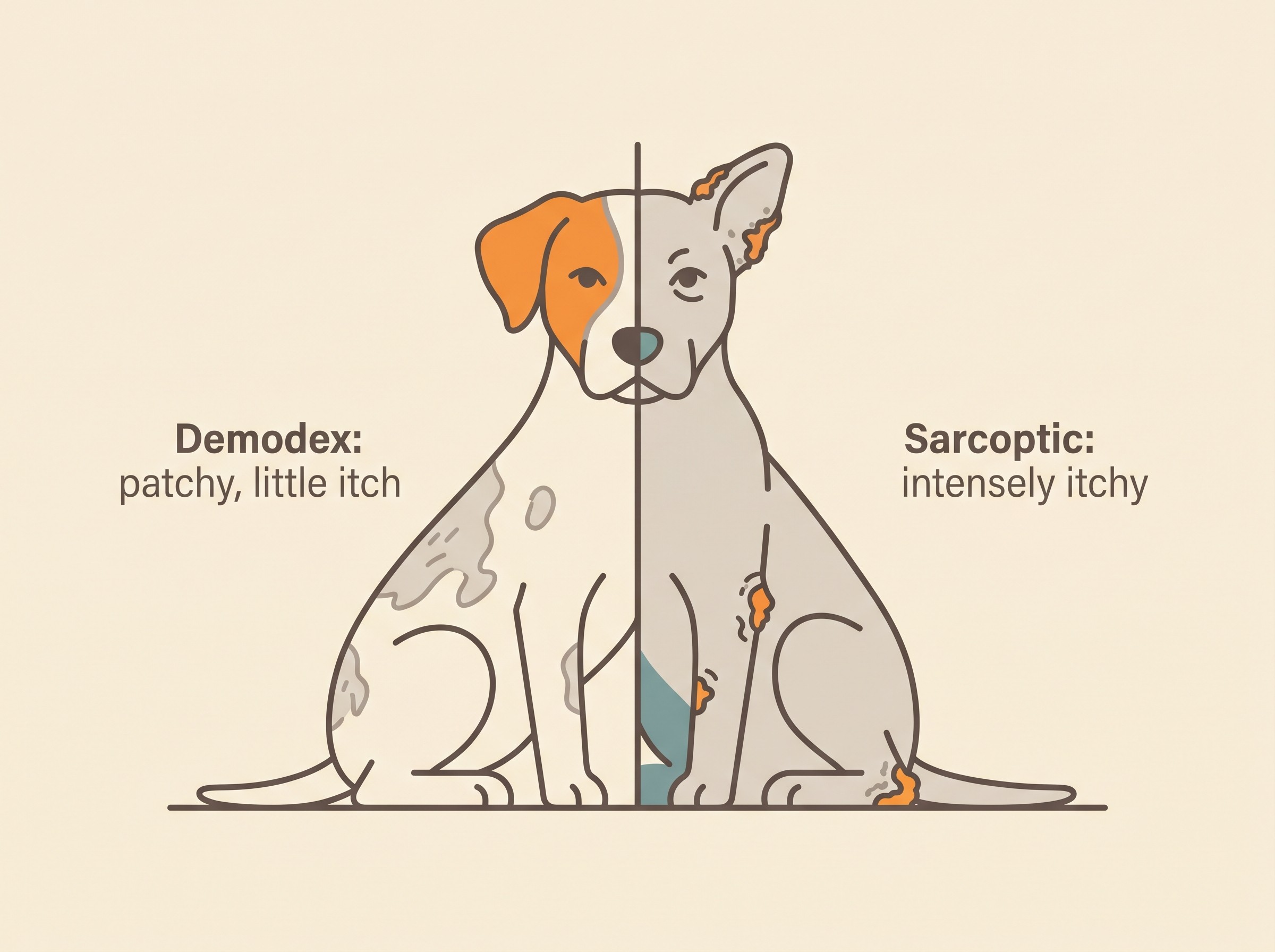
Two mange mites belong at the start of any allergy work-up, taken off the table before anyone spends a penny chasing an allergy. Both can imitate allergy or stack on top of it, and one of them you really cannot afford to miss. The five-cause differential and the order it runs in belong to the funnel article (why is my pet so itchy), so we will not re-list all five here. The reason mites go first is practical: a parasite is cheap to rule out and treatable when found, so it gets checked before money goes on long-term allergy management (Mueller et al., 2020). And the two mites behave almost as opposites. Demodex is usually itch-free; sarcoptic mange is about as itchy as dermatology gets. Hold that contrast and the rest of this falls into place.
Demodex: the mite your dog already had
The first thing that catches owners out is that this mite is not caught from anywhere. Demodex canis lives in the hair follicles of healthy dogs in small numbers as a normal commensal, and disease is the overgrowth of that resident mite rather than the arrival of a new one (Mueller et al., 2020; CAPC, 2023). Pups pick it up from their mother by direct skin contact in the first days of life, which is why puppies delivered by caesarean and reared away from the dam never acquire it (Mueller et al., 2012; CAPC, 2023). So demodicosis is not contagious from another dog, the park or the bedding, and in-contact animals do not need treating (CAPC, 2023).
The second thing that surprises people is that uncomplicated demodex usually does not itch much (Mueller et al., 2020). When a "mangey" dog is also frantically scratching, the itch is almost always coming from a secondary bacterial infection in the damaged skin rather than the mite, and it settles once that infection is treated (Mueller et al., 2020). Demodex plus heavy itch usually means a layer of pyoderma sitting on top, the detail of which belongs to skin and ear infections.
Demodicosis comes in two sizes. Localised disease is a few patches of hair loss, commonly fewer than about six, usually on the face or a leg, mostly in young dogs, and it often clears on its own (Mueller et al., 2020). Generalised disease is more extensive, a whole body region or two or more feet involved, and does need treating (Mueller et al., 2020). Age is a genuine clue here. Juvenile-onset generalised demodicosis, typically under a year old, reflects an immature or inherited immune predisposition, which is why affected dogs should not be bred from (Mueller et al., 2020; Mueller et al., 2012).
It is adult-onset generalised demodicosis that should make a vet's ears prick up. In an older dog with no history of it, the overgrowth points to something suppressing the immune system, so it earns a hunt for an underlying problem (hyperadrenocorticism, hypothyroidism, neoplasia, leishmaniosis) or a drug cause such as corticosteroids or chemotherapy, worked up with clinical exam, bloods and hormonal testing as indicated (Mueller et al., 2020). A nuance the pharma-adjacent pages skip: a substantial proportion of adult-onset cases still have no identifiable cause even after a thorough search (Mueller et al., 2020). If the trail leads to a hormonal disease, the endocrine side is picked up onward from hair loss without itching.
One warning, because owners get caught by it. Steroids are the wrong drug for a demodex dog. Glucocorticoids suppress immunity and let the mites proliferate, so they can tip localised disease into generalised and are contraindicated in demodicosis (Mueller et al., 2020; Mueller et al., 2012).
Treatment is far easier than it used to be. The isoxazoline parasiticides (fluralaner, afoxolaner, sarolaner, lotilaner) are now a recommended first-line option and have largely replaced the old amitraz dips and daily off-licence wormers (Mueller et al., 2020). In a European field trial a single dose of oral or spot-on fluralaner cleared mites from 98 to 100% of dogs by day 56 to 84, with 92% mite-free by day 28 (Petersen et al., 2020), and monthly afoxolaner performed similarly (NexGard demodicosis field study, 2018). NexGard (afoxolaner) carries a UK licensed indication for treating demodicosis in dogs (NexGard SPC, NOAH).
That is a real advance, but it is not "one tablet and done". Cure is defined by the mites, not the coat: treatment continues, monitored with repeat deep skin scrapings, until two consecutive scrapings about a month apart come back negative. Stopping when the fur looks better but mites remain is a common cause of relapse (Mueller et al., 2020; Mueller et al., 2012). Photographing the same patches at each recheck in the Skin and Itch Tracker gives you a record to bring to the scraping appointment.
Cats have demodex too. Demodex cati is a follicular commensal whose generalised disease is rare and usually flags an underlying illness, but the exception to almost every demodex rule is the surface-dwelling Demodex gatoi, which is itchy and contagious between cats, so it behaves far more like an allergy mimic (Saari et al., 2009; Mueller et al., 2020). The wider feline allergy picture belongs to feline atopic syndrome.
Sarcoptic mange: itch that runs ahead of the rash
Sarcoptic mange is the opposite animal, and the reason this article sits in an allergy space at all. Sarcoptes scabiei var. canis burrows into the skin and provokes an intense hypersensitivity reaction to the mite and its products, producing itch that is severe, often relentless, and characteristically out of proportion to how little the skin actually shows (Cornell Riney Canine Health Center; Mueller et al., 2020). That feature, an itch far worse than the lesions would explain, is the most useful thing separating it from atopy.
The distribution is the next clue, and a different map from allergy. Scabies favours the sparsely haired sites: the margins of the ear flaps, the elbows, the hocks and the underside of the chest and abdomen, with crusting and self-trauma (Cornell Riney Canine Health Center; Pin et al., 2006). That looks nothing like the face, paw, armpit and groin pattern of atopic dermatitis, owned by atopic dermatitis explained.
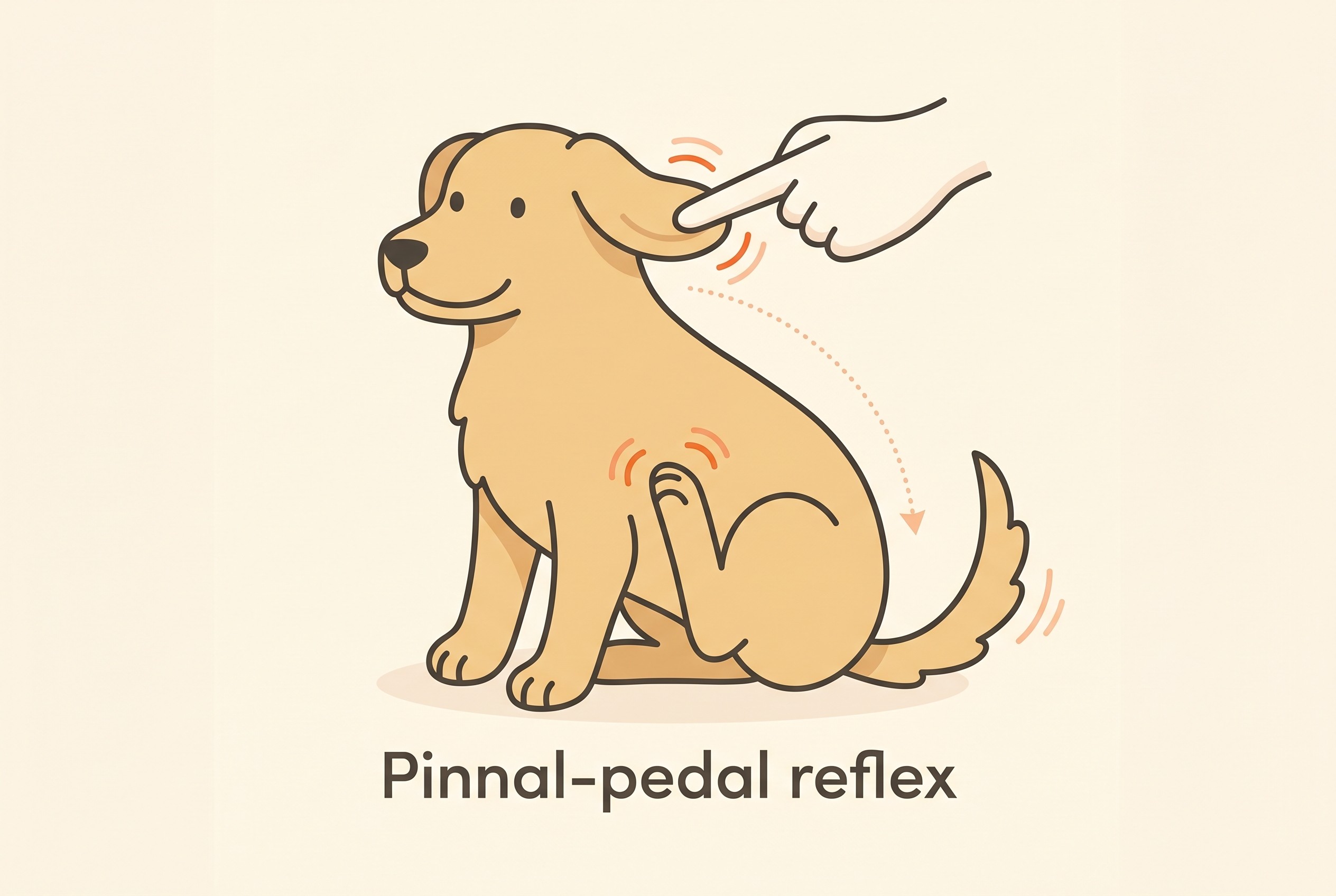
There is a neat bedside test, the pinnal-pedal reflex: firmly rubbing the edge of the ear flap provokes a reflex hind-leg scratch on the same side in most scabies cases. In a study of 588 dogs with skin disease it was positive in about 82% of confirmed scabies cases but in only 6.2% of dogs with other skin disease (a sensitivity of roughly 82%, a specificity of about 94%) (Mueller et al., 2001). It is a strong pointer when positive but no way to clear scabies when negative: with roughly 18% false negatives, a negative reflex does not let you off the hook.
Two more things set scabies apart. It is contagious, spreading between dogs by direct contact and through shared spaces like kennels, grooming parlours and parks, with foxes a wildlife reservoir (Cornell Riney Canine Health Center). And it is zoonotic: people in contact can develop an itchy, spotty rash, though infestation from a dog is usually self-limiting once the dog and household are treated, because the canine mite cannot complete its life cycle on human skin (Cornell Riney Canine Health Center; Moroni et al., 2022). A reason to act, not to panic, and why a vet may treat the household. Cats can be transiently affected but do not sustain infestation; their own intensely itchy, head-and-ear equivalent is notoedric mange (Notoedres cati), rare but highly contagious between cats (Merck Veterinary Manual).
Why a scrape can say "no" when the answer is "yes"
A content mill implies a skin scrape is the final word. It is not: Sarcoptes mites are notoriously hard to find, and a superficial scrape is positive in only a minority of confirmed cases, so a negative scrape does not rule scabies out (Merck Veterinary Manual; Mueller et al., 2020). A blood test exists, an anti-Sarcoptes IgG ELISA, more sensitive at around 84% sensitivity and 90% specificity, but the antibodies take several weeks to appear, so it too can be falsely negative early (Lower et al., 2001).
So when the history and the pattern fit, a therapeutic trial with an effective acaricide is a legitimate, often-preferred diagnostic step in its own right, with a clear response usually within a few weeks (Cornell Riney Canine Health Center; Mueller et al., 2020). A trial only tells you anything if you can see the response. Scoring the itch and photographing the ear margins and elbows in the Skin and Itch Tracker turns a vague "she seems a bit better" into a measurable fall in the score: a true scabies response shows as that line dropping, where an allergy that was never going to respond holds flat.
Treatment itself is highly effective. A single dose of oral or topical fluralaner produced a 100% reduction in mite counts by four weeks (Taenzler et al., 2016), oral afoxolaner gave 100% efficacy at days 28 and 56 with resolution of the itch and crusting (Beugnet et al., 2016), and sarolaner reached 100% reduction after two monthly doses (Becskei et al., 2016). On licensing, be precise rather than sweeping: Simparica and Simparica Trio (sarolaner) carry a UK licensed indication for treating sarcoptic mange in dogs, whereas some highly effective, well-evidenced products such as fluralaner are used off-licence under the prescribing cascade (Simparica SPC, NOAH). Not every product is licensed for every mite, even when the evidence is excellent.
When to suspect mites over allergy
Pull the discriminators into something you can act on. Push scabies up the list with sudden-onset severe itch, especially non-seasonal and rapidly worsening; itch out of proportion to how the skin looks; an ear-margin, elbow and hock distribution; a positive pinnal-pedal reflex; in-contact animals or people also itching; a history of kennels, shelter or stray contact; or itch that is not responding to allergy treatment (Cornell Riney Canine Health Center; Mueller et al., 2020). Any one of those justifies either a scrape or, given how often the scrape misses, a treatment trial. For demodex, the clue is patchy hair loss in a young dog, or new generalised hair loss in an older one that earns the underlying-disease search (Mueller et al., 2020). If you are weighing up whether this warrants a vet visit now, the itchy pet triage check will point you.
This article covers only the two mange mites. The smaller culprits, ear mites, harvest mites and walking dandruff, live in the smaller culprits, and the other big parasitic mimic in flea allergy dermatitis. And unlike a mite, ruled out fast and cheaply, a suspected food cause needs a proper diet trial run through the Elimination-Diet Companion, so do not let "we checked for mites" stand in for that.
So if the itch came on fast, sits on the edges of the ears and the elbows, or is being shared around the household, the next step is concrete: flea-treat everything, log the itch score, photograph the pattern, and book a vet review. You will have handed over the pattern and trend a vet needs, and a treatment trial that works shows its hand within weeks.
References
- Mueller RS, Rosenkrantz W, Bensignor E, Karas-Tecza J, Paterson T, Shipstone MA. (2020). Diagnosis and treatment of demodicosis in dogs and cats: Clinical consensus guidelines of the World Association for Veterinary Dermatology. Veterinary Dermatology, 31(1), 5-27.
- Companion Animal Parasite Council. Demodex spp. CAPC Guidelines. Companion Animal Parasite Council. Accessed 2023.
- Mueller RS, Bensignor E, Ferrer L, Holm B, Lemarie S, Paradis M, Shipstone MA. (2012). Treatment of demodicosis in dogs: 2011 clinical practice guidelines. Veterinary Dermatology, 23(2), 86-96.
- Petersen I, Chiummo R, Zschiesche E, Karas-Tecza J, Rapti D, Roepke R, Thomas E. (2020). A European field assessment of the efficacy of fluralaner (Bravecto) chewable and spot-on formulations for treatment of dogs with generalized demodicosis. Parasites & Vectors, 13, 304.
- Saari SAM, Juuti KH, Palojarvi JH, Vaisanen KM, Rajaniemi RL, Saijonmaa-Koulumies LE. (2009). Demodex gatoi-associated contagious pruritic dermatosis in cats: a report from six households in Finland. Acta Veterinaria Scandinavica, 51(1), 40.
- Mueller RS, Bettenay SV, Shipstone M. (2001). Value of the pinnal-pedal reflex in the diagnosis of canine scabies. Veterinary Record, 148(20), 621-623.
- Moroni B, Rossi L, Bernigaud C, Guillot J. (2022). Zoonotic Episodes of Scabies: A Global Overview. Pathogens, 11(2), 213.
- Lower KS, Medleau LM, Hnilica K, Bigler B. (2001). Evaluation of an enzyme-linked immunosorbent assay (ELISA) for the serological diagnosis of sarcoptic mange in dogs. Veterinary Dermatology, 12(6), 315-320.
- Taenzler J, Liebenberg J, Roepke RKA, Frenais R, Heckeroth AR. (2016). Efficacy of fluralaner administered either orally or topically for the treatment of naturally acquired Sarcoptes scabiei var. canis infestation in dogs. Parasites & Vectors, 9, 392.
- Beugnet F, de Vos C, Liebenberg J, Halos L, Larsen D, Fourie J. (2016). Efficacy of afoxolaner in a clinical field study in dogs naturally infested with Sarcoptes scabiei. Parasite, 23, 26.
- Becskei C, De Bock F, Illambas J, Cherni JA, Fourie JJ, Lane M, Mahabir SP, Six RH. (2016). Efficacy and safety of a novel oral isoxazoline, sarolaner (Simparica), for the treatment of sarcoptic mange in dogs. Veterinary Parasitology, 222, 56-61.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing allergies & skin. Free to join.
Join PetsLikeMine