GOLPP: Why Laryngeal Paralysis Is a Whole-Body Condition
Claire Greenway
BVM&S MRCVS
A diagnosis of laryngeal paralysis in an older dog usually comes with three things: it's a problem with the voice box, the breathing can be helped, and there's an operation for it. All true. But it's only the first chapter of a longer story, and I'd rather you heard the whole thing from me, gently and plainly, than stumbled on it months from now when the back legs start to go and nobody warned you.
There's a part many owners are never told at the first appointment. In an older dog, what we used to call "idiopathic" laryngeal paralysis is usually not just a larynx problem. It is the first and loudest sign of a slow, generalised nerve condition that, over months to years, also weakens the back legs and the gullet. The veterinary world now has a name for the whole picture: geriatric onset laryngeal paralysis polyneuropathy, or GOLPP (Cornell University, n.d.; Kitshoff et al., 2013). That name was a deliberate change, championed by the Michigan State University group led by Dr Bryden Stanley, because "idiopathic laryngeal paralysis" was steering owners and vets into treating one nerve when the truth was body-wide (Zeltzman, 2016). The recognition, the surgery decision, the feeding and the day-to-day all live in companion guides I'll point you to as we go. My job here is the long view.
Why the larynx goes first
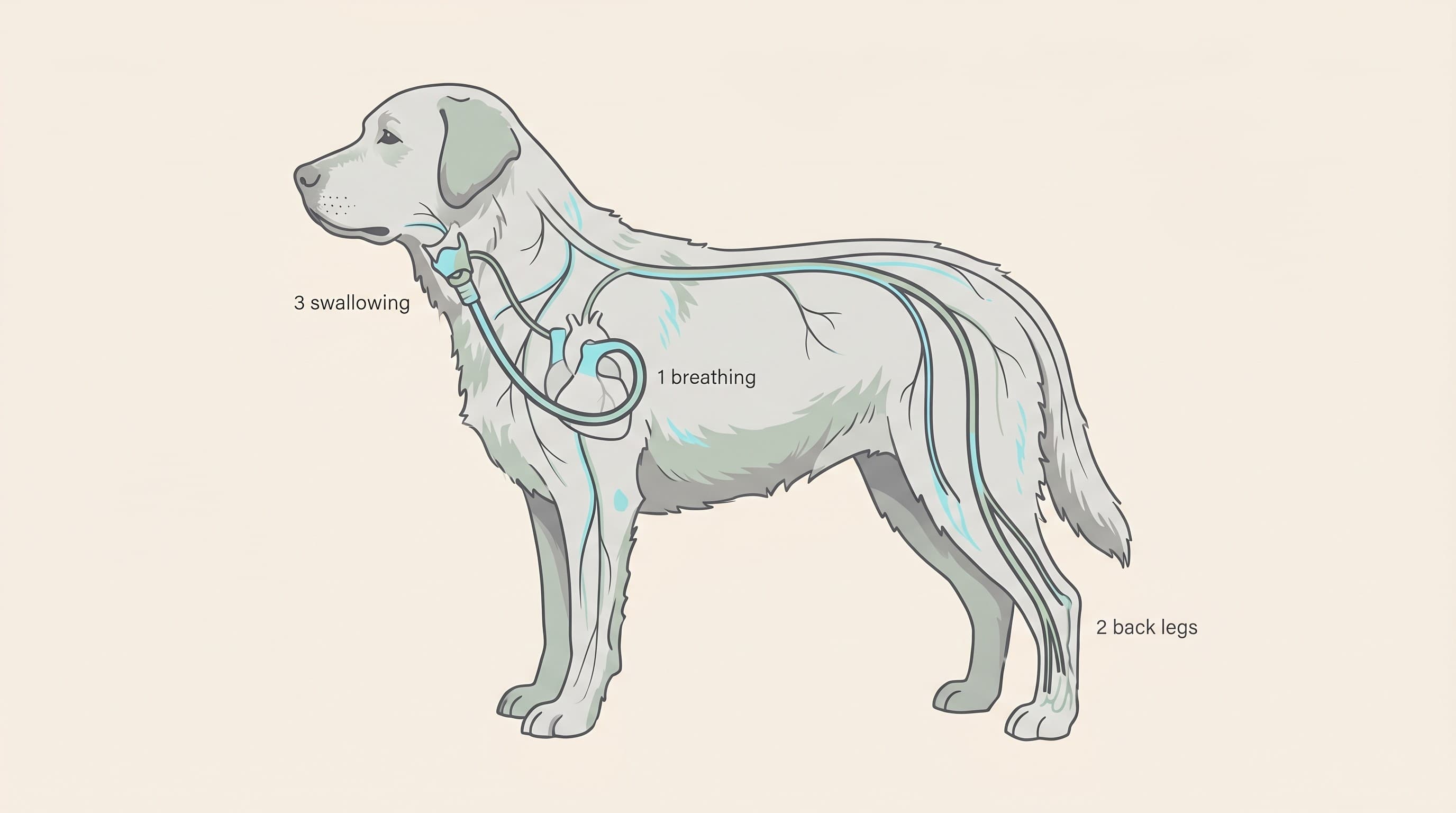
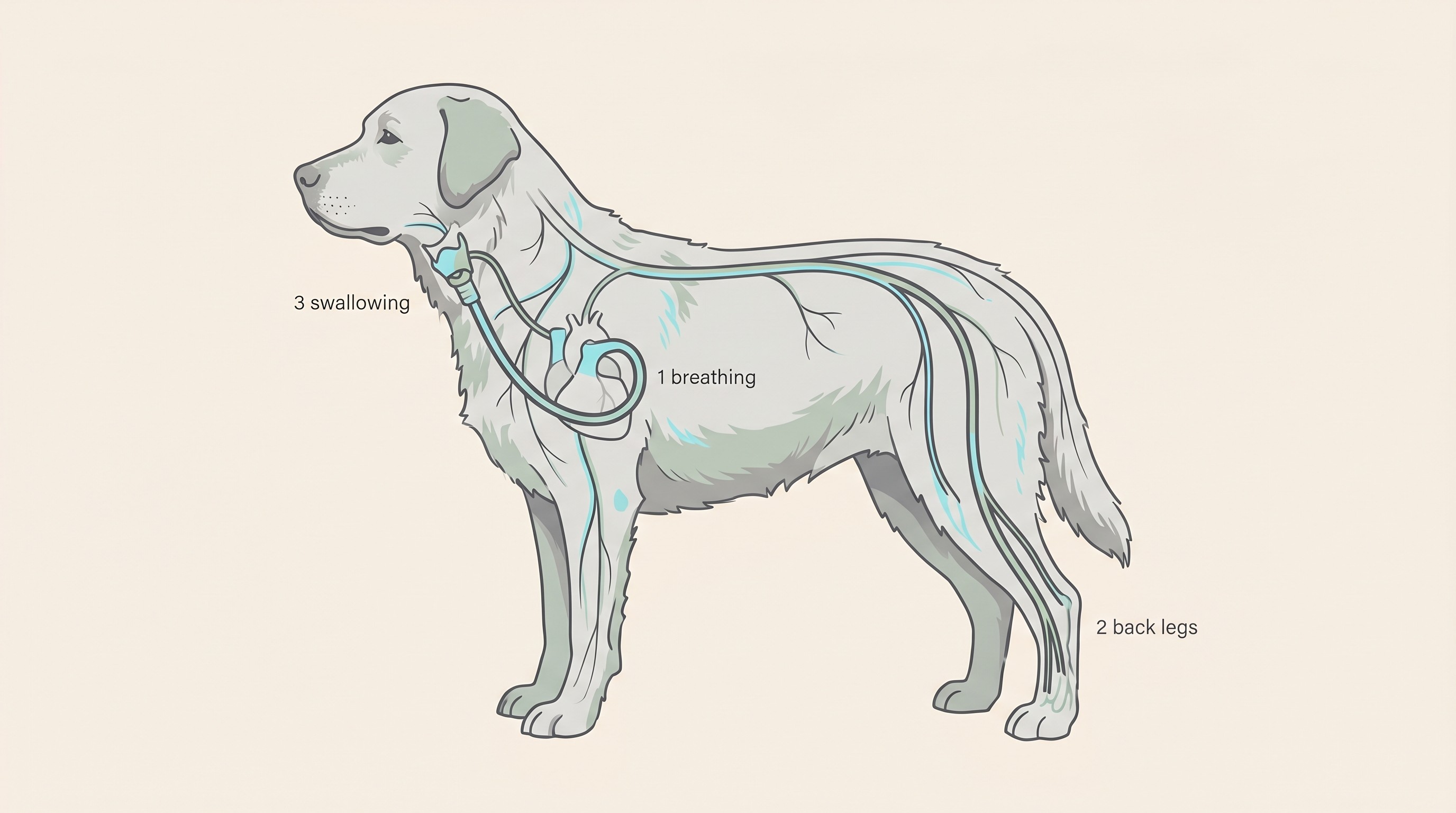
The clue to the whole thing is in which parts fail, and in which order. When researchers studied the nerves of affected Labradors in detail, they found a length-dependent peripheral nerve disease: a precise way of saying the longest nerves in the body wear out earliest and worst, with the damage most marked in the far ends of those nerves (Anderson et al., 2024).
Think about which nerves those are. The recurrent laryngeal nerve, the one that works the voice box, is one of the longest in the entire dog: it runs all the way down into the chest, loops around, and travels back up to the larynx. The sciatic nerve to the back legs is long too, and the same study looked at both the laryngeal and the sciatic nerves and found the same axonal wear (Anderson et al., 2024). So the first to fail are exactly the ones that open the airway and the ones that power the hind end. That is why the picture is so consistent: breathing trouble first, then, later, a wobble behind. It isn't bad luck or two unrelated diseases piling up, it's one disease working through the body longest-nerve-first.
This isn't a theory somebody floated. It rests on three kinds of evidence that line up. In one careful controlled study, around a third of dogs with laryngeal paralysis already had wider neurological signs at diagnosis, every single one had developed generalised neurological signs within a year, and their oesophageal function was measurably poorer than the healthy dogs matched against them (Stanley et al., 2010). Nerve and muscle samples under the microscope showed the loss of large nerve fibres and the muscle wasting of a generalised nerve disease, not a single local lesion at the voice box (Thieman et al., 2010). And an independent Cornell group following ninety dogs found around half of those they could track had wider neurological problems too, such as weak back legs or a poorly working gullet (Bookbinder et al., 2016). Different teams, in different countries, reaching the same conclusion.
How it unfolds in practice
It helps to think of it as an order of trouble over the life of your dog.
Breathing comes first, and it's the urgent part. This is the laryngeal paralysis itself: the change in the bark, the raspy noise on the in-breath, and the real danger of a breathing crisis in heat or with hard exercise. I won't re-tread the recognition here, because the laryngeal paralysis explainer does it properly, and heat and exercise safety covers keeping a dog with laryngeal paralysis safe in warm weather, which genuinely saves lives.
Then, slowly, the back end. Over months to years, you may notice a gradual hind-limb weakness: a sway or a wobble, the back paws scuffing or knuckling over, a struggle to rise, and a visible thinning of the muscle over the hips and thighs (Cornell University, n.d.; VCA Animal Hospitals, n.d.). The key word is gradual. This is a slow drift, not a cliff edge, and many dogs have a long stretch of good, mobile time before it amounts to much.
And the gullet. The same nerves that struggle to swallow well raise a lifelong risk of food, water or even saliva going the wrong way, down into the lungs rather than the stomach. We call that aspiration, and it's why a cough or a gag around mealtimes matters in a GOLPP dog in a way it might not in a healthy one. More on that below.
Naming these in advance steadies owners. When a back paw scuffs on a walk in a year's time, you recognise an old, expected change rather than a fresh catastrophe, and you know it's worth a mention to your vet rather than a sleepless night.
Where the mobility picture overlaps
GOLPP dogs are older, mostly large breeds, the Labradors and the setters and the bigger crossbreeds (Kitshoff et al., 2013). And older large dogs very commonly have arthritis. So when the back legs start to weaken, wobble, knuckle and lose muscle, you are often looking at two things at once: some of it is nerve, the GOLPP, and some of it may well be joints, the osteoarthritis. They pile on top of one another, and from the outside they can look almost identical.
The reality is that you usually can't fully separate them by eye at home, and you don't need to, because much of the same supportive care helps both. Keeping your dog lean takes load off worn joints and weak muscles alike. Traction on slippery floors stops the scrabbling that frightens a wobbly dog. Ramps instead of jumps, a well-fitted support harness to steady the back end on stairs and into the car, and gentle, controlled exercise with physiotherapy or hydrotherapy all spare the joints and the nerves and help hold onto the muscle both conditions are eating away.
This is why I'd want the back end properly assessed rather than written off as "just the dog with laryngeal paralysis getting old". If arthritis is part of the picture, there is specific, effective help for it. I won't explain arthritis here, because it has a whole space of its own: have a look through our Arthritis and Mobility space, and run your dog through the Mobility Check tool, built to score exactly the kind of hind-end change GOLPP throws up. That cross-link is the single most useful practical thing I can hand you here.
Keeping watch on the swallow
The gullet deserves its own moment, because it's the part owners least expect and it carries the quiet risk. The oesophagus, the muscular tube that carries food to the stomach, worked measurably less well in dogs with laryngeal paralysis than in healthy ones, and it was at its worst with liquids (Stanley et al., 2010). At the more severe end, GOLPP dogs are reported to be markedly more likely to develop megaoesophagus, a slack, widened, poorly emptying gullet, with clinical references putting it at around twenty-one times more likely than in dogs without the condition (VCA Animal Hospitals, n.d.). I'd treat that exact number as a clinical-reference estimate rather than a hard law, but the direction is solid and is backed by the controlled study above: GOLPP genuinely loads the dice towards a weak gullet (Stanley et al., 2010).
Why does that matter so much? Because a poorly working gullet, combined with a larynx that no longer closes the airway crisply, is the recipe for aspiration: food, water or saliva slipping into the lungs and seeding pneumonia. This is why a GOLPP dog is worth feeding and watching a little differently. The actual playbook, the raised feeding, the unhurried meals, the texture changes, the no-swimming rule and the warning signs of pneumonia, lives in the aspiration pneumonia guide.
One light habit ties this together: counting your dog's resting breathing rate while they sleep. Under about thirty breaths a minute is normal, thirty or more and climbing over a few days is worth a vet call, and forty or more is urgent. That threshold was validated for monitoring heart disease, where most well-controlled dogs keep their sleeping rate under thirty, so treat it as a general "breathing harder than it should at rest" signal rather than a GOLPP-specific number (Porciello et al., 2016). In a GOLPP dog a rising rate can be an early hint of a brewing aspiration pneumonia, so it's well worth tracking with the breathing rate tool or logging alongside exercise tolerance in the airway diary.
Before you weigh up the surgery
If a tie-back operation, arytenoid lateralisation in full, is on the table or already done, there is one thing I will not soften, because getting it wrong sets owners up for heartbreak.
A tie-back fixes the breathing. It does not fix the nerves.
The operation holds one side of the voice box open so air can get past, and it genuinely works: it relieves the airway obstruction and, in study after study, improves quality of life, with most dogs breathing markedly better afterwards (Kitshoff et al., 2013; Sample et al., 2020). What it cannot do is restore the larynx's normal function or halt the underlying nerve disease (Cornell University, n.d.; VCA Animal Hospitals, n.d.). In Dr Stanley's own account to the profession, surgery improves the breathing but does not arrest the polyneuropathy, which keeps quietly progressing in the background (Zeltzman, 2016). The back legs and the gullet carry on regardless.
There is a sting in the tail, too, and it ties straight back to the gullet. Because a tie-back deliberately props the airway open against a weakening swallow, the risk of aspiration becomes a lifelong watch rather than a one-off worry around the operation. In one large study, aspiration pneumonia affected around nineteen percent of dogs within the first year and rose to roughly a third by three to four years out, with that slack megaoesophagus a key driver (Wilson and Monnet, 2016). I say this not to scare you off surgery, which helps a great many dogs breathe and live better, but so the decision is made with clear eyes. The candidacy, the UK costs and the referral pathway belong in the tie-back surgery decision guide. My single point here: never let anyone, including a hopeful corner of your own mind, frame a tie-back as a cure.
A realistic long view
So where does this leave you? With a progressive condition, yes, but a slow one, and one with a great deal of good time and real things that help inside it.
The best data we have comes from a survey of seventy-six owners of older Labradors with late-onset laryngeal paralysis. Almost all, ninety-four percent, felt the condition affected their dog's quality of life, and just under half, forty-seven percent, felt it was a large contributing factor in how their dog's life ended (Sample et al., 2020). Those are sobering numbers, drawn from one of the most affected breeds, and I won't dress them up. But the same study carried a thread of hope: the dogs that had the tie-back surgery were reported to have better quality of life, and the disease was felt to contribute less to their death, than the dogs that did not have surgery (Sample et al., 2020). Knowing the whole-body picture is what lets you act on that, by treating the dog and not just the larynx.
That is why I wanted you to have the full story rather than the comfortable half. Knowing this is GOLPP, and not merely a voice box that's packed in, changes what you do: you watch the gullet and feed accordingly, you take the breathing crisis seriously in the heat, you get the back end assessed and supported instead of shrugging it off as old age, and you set your expectations clearly so the slow changes ahead feel managed rather than ambushing you. None of that makes the disease disappear, but all of it buys comfort and time, which is the whole point.
For the day-to-day of living well with a dog with laryngeal paralysis, and a warm, established owner community that has walked this exact road, living with laryngeal paralysis is the place to start, and the owner-run resource at larparlife.com is worth knowing about. Knowing the whole dog is how you protect them.
References
- Anderson, R. S., Chu, A. K., Rylander, H., Binversie, E. E., Duncan, I. D., Baker, L., Salamat, S., Patterson, M. M., Gruel, J., Kohler, N. L., Kearney, H. K., Ale, S. M., Momen, M. M., Muir, P., Svaren, J. P., Johnson, R., & Sample, S. J. (2024). Pathologic classification of a late-onset peripheral neuropathy in a spontaneous Labrador retriever dog model. The Journal of Comparative Neurology, 532(3), e25596.
- Bookbinder, L. C., Flanders, J., Bookbinder, P. F., Harvey, H. J., Barry, J. S., & Cheetham, J. (2016). Idiopathic canine laryngeal paralysis as one sign of a diffuse polyneuropathy: An observational study of 90 cases (2007-2013). Veterinary Surgery, 45(2), 254-260.
- Cornell University College of Veterinary Medicine, Riney Canine Health Center. (n.d.). Laryngeal paralysis.
- Kitshoff, A. M., Van Goethem, B., Stegen, L., Vandekerckhove, P., & de Rooster, H. (2013). Laryngeal paralysis in dogs: An update on recent knowledge. Journal of the South African Veterinary Association, 84(1), Art. #909.
- Porciello, F., Rishniw, M., Ljungvall, I., Ferasin, L., Häggström, J., & Ohad, D. G. (2016). Sleeping and resting respiratory rates in dogs and cats with medically-controlled left-sided congestive heart failure. The Veterinary Journal, 207, 164-168.
- Sample, S. J., Stilin, A., Binversie, E. E., Baker, L. A., & Hardie, R. J. (2020). Late-onset laryngeal paralysis: Owner perception of quality of life and cause of death. Veterinary Medicine and Science, 6(3), 306-313.
- Stanley, B. J., Hauptman, J. G., Fritz, M. C., Rosenstein, D. S., & Kinns, J. (2010). Esophageal dysfunction in dogs with idiopathic laryngeal paralysis: A controlled cohort study. Veterinary Surgery, 39(2), 139-149.
- Thieman, K. M., Krahwinkel, D. J., Sims, M. H., & Shelton, G. D. (2010). Histopathological confirmation of polyneuropathy in 11 dogs with laryngeal paralysis. Journal of the American Animal Hospital Association, 46(3), 161-167.
- VCA Animal Hospitals. (n.d.). Laryngeal paralysis in dogs.
- Wilson, D., & Monnet, E. (2016). Risk factors for the development of aspiration pneumonia after unilateral arytenoid lateralization in dogs with laryngeal paralysis: 232 cases (1987-2012). Journal of the American Veterinary Medical Association, 248(2), 188-194.
- Zeltzman, P. (2016, November 14). How "lar par" is multifaceted but treatable. Veterinary Practice News.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing breathing & airways. Free to join.
Join PetsLikeMine