Tie-Back Surgery for Laryngeal Paralysis: How to Decide
Dr. Alastair Greenway
MRCVS
A specialist has mentioned a "tie-back", quoted a number that made you blink, and somewhere in the small print was the word aspiration. The dog in question is usually older, often a Labrador or another big breed, with breathing that has turned noisy and laboured, and perhaps a frightening episode already behind you on a warm day. That is the moment most owners reach this page: trying to work out whether the operation is the right move or the wrong one.
Let me take some of the heat out of it. There's a clear, well-evidenced way through this, covering who the operation genuinely suits, what it can and cannot do, the real UK cost and pathway, and the questions to take to the surgeon. I can't put my hands on your dog, so I won't tell you what to do, but I can give you a clear way to decide. I'll take it as read that you know what laryngeal paralysis is and how to spot it; if not, the laryngeal paralysis explainer does that, and this piece stays on the decision.
What a tie-back actually is
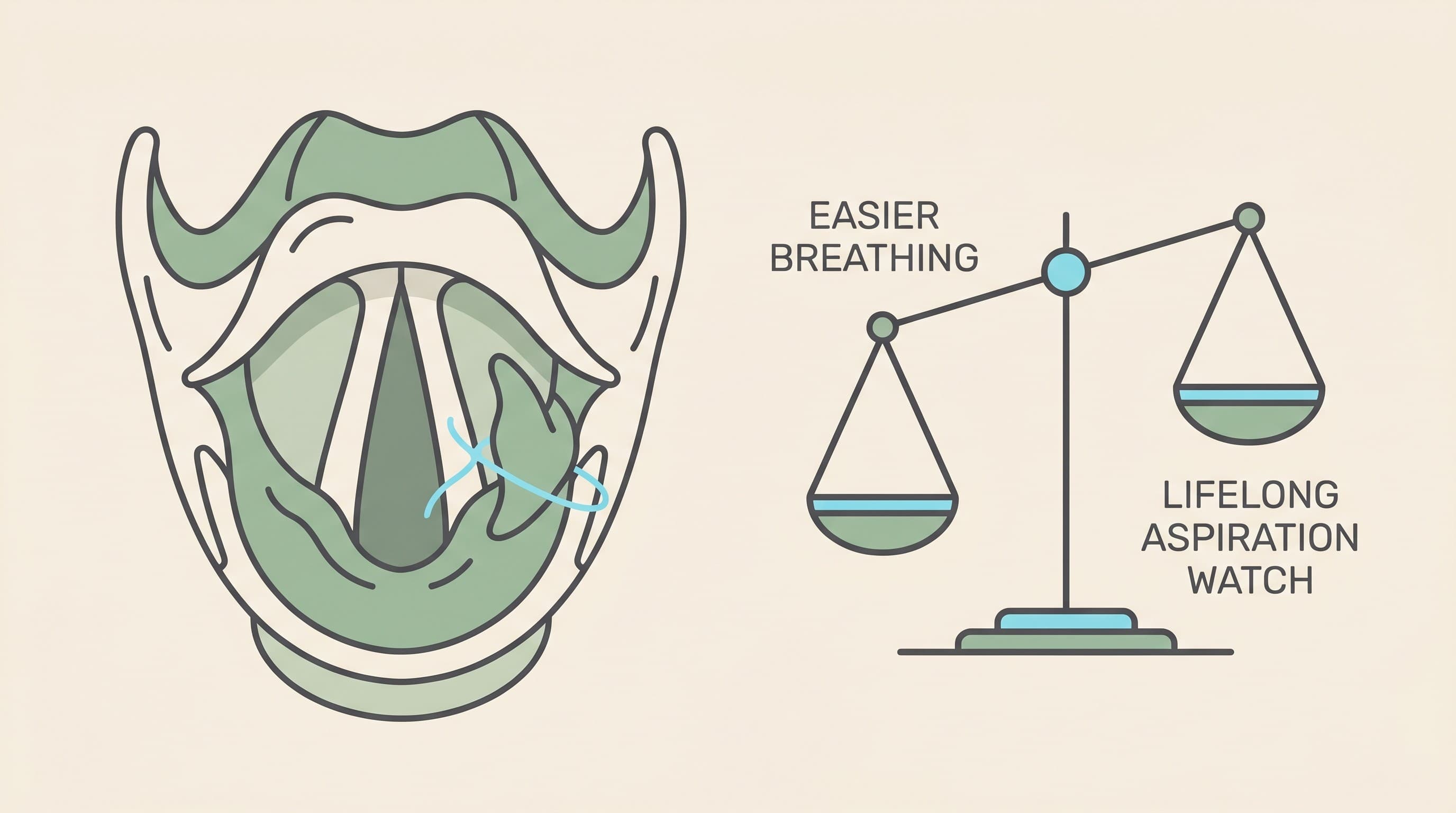
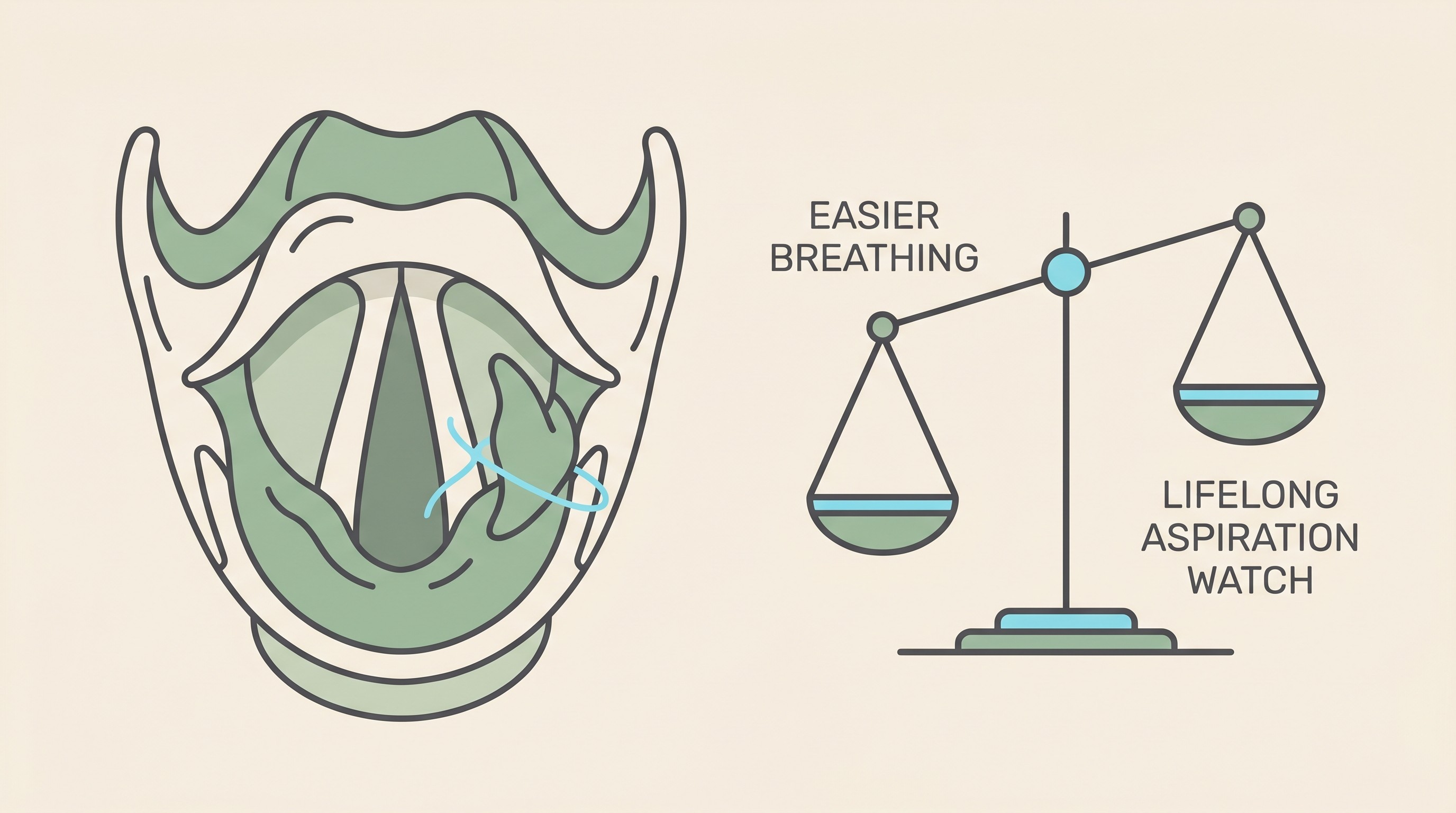
"Tie-back" is the everyday name for unilateral arytenoid lateralisation. Stripped of the Latin: the surgeon places a permanent stitch that pulls one side of the voice box out and holds it open, so the airway no longer collapses shut on the in-breath and air can get past (American College of Veterinary Surgeons, n.d.; Willows Veterinary Centre and Referral Service, n.d.). It's a fairly straightforward operation through a small neck incision, and it has sat for years "at the top of the list of procedures with good success and few complications" for this condition (American College of Veterinary Surgeons, n.d.).
Two things are worth fixing in your mind first. One is that only one side is deliberately tied back, never both. That isn't a half-measure: opening both sides strips the airway of its ability to protect the lungs, and the landmark series found dogs that had both sides done were significantly more likely to suffer complications and less likely to survive than those that had one (MacPhail and Monnet, 2001).
The other is the heart of the decision. A tie-back is palliative, not curative. It relieves the airway obstruction, but it does not restore the larynx's normal function, and it does nothing to slow the underlying nerve disease behind most older dogs' laryngeal paralysis (American College of Veterinary Surgeons, n.d.; Southfields Veterinary Specialists, n.d.). The way I put it to owners is simple: a tie-back fixes the breathing, not the nerves. Hold on to that line, because every other part of this decision hangs off it. (If the whole-body picture behind it is new to you, GOLPP as a whole-body condition tells it properly.)
Who it's for, and when
The decision is driven by the breathing, not the diagnosis label. A dog can have laryngeal paralysis on a scope and barely a symptom in daily life, and that dog does not need an operation today.
Surgery is for dogs with moderate to severe clinical signs: the noisy, laboured breathing, the exercise intolerance, and above all the dog who has had one or more genuine breathing crises in heat or with exertion (Southfields Veterinary Specialists, n.d.; American College of Veterinary Surgeons, n.d.). UK referral centres are clear it is "usually only performed on patients suffering clinical signs" (Willows Veterinary Centre and Referral Service, n.d.). The crisis-prone dog is the clearest candidate of all, for a blunt reason: once a dog has reached the point of respiratory crisis, those episodes tend to keep coming, because the airway simply cannot do its job (American College of Veterinary Surgeons, n.d.). Waiting, in that dog, is its own danger.
There's no fixed age at which a dog is "too old". These are typically older patients, so the team weighs anaesthetic fitness and looks hard at the chest first, but age by itself is not the deciding factor: the danger of not operating on a crisis-prone dog sits on the scales too. The flip side is just as real: a dog with only mild signs can reasonably be managed without surgery for now.
What it fixes well, and what it can't
The encouraging half is genuinely encouraging. Around 90 to 95% of dogs that have a tie-back end up with a significantly improved airway and a better quality of life (Willows Veterinary Centre and Referral Service, n.d.; Southfields Veterinary Specialists, n.d.), and the classic peer-reviewed series put hard numbers on it: 35 of 39 dogs, about 90%, had an improved quality-of-life score afterwards (Hammel et al., 2006). Many owners describe the dog seeming years younger, breathing quietly again, able to enjoy a walk without that desperate, sawing noise.
Now the half the cheaper write-ups skate over. An airway held permanently open cannot close fully to guard the lungs during a swallow, and a tie-back dog can't cough as effectively to clear what slips past, so food, water or even saliva can go the wrong way into the lungs and seed pneumonia. The trade-off is precise: surgery does not remove the aspiration risk, it changes its nature, swapping a partly-shut, dangerous airway for a permanently open one that needs lifelong care around mealtimes (American College of Veterinary Surgeons, n.d.; MacPhail and Monnet, 2001).
So how big is that risk? Across the studies, aspiration pneumonia affects roughly 8 to 25% of tie-back dogs over their lifetime, with UK centres quoting 8 to 21% (Southfields Veterinary Specialists, n.d.). The crucial nuance is that it rises the longer the dog lives, rather than being a single hurdle cleared in the recovery weeks: the largest series found it in about 18.6% of dogs by one year, climbing to around 31.8% by three to four years out (Wilson and Monnet, 2016). So I'll say it plainly: a tie-back does not end the aspiration story, it begins a managed one. The day-to-day discipline that keeps that risk low is straightforward and has its own home, so I won't teach it here: the aspiration pneumonia guide covers how to feed, water and watch a tie-back dog, and the tie-back aspiration watch is an at-a-glance reference worth printing for the fridge.
Weighing the wider risks
Beyond aspiration, it's fair to ask about complications in general. As context, not a scare: somewhere between 10 and 58% of dogs develop some complication at some stage, a wide range because it sweeps up everything from a brief cough or gag to a seroma over the wound (Southfields Veterinary Specialists, n.d.). The landmark series recorded an overall complication rate around 34%, a related-cause mortality around 14%, and aspiration pneumonia as the commonest single complication at about 24% (MacPhail and Monnet, 2001). Minor niggles were common, 56% of dogs in one series had one such as ongoing coughing, gagging, continued exercise intolerance or a seroma, but crucially most of those did not dent the owner-rated quality of life (Hammel et al., 2006).
In modern hands the picture looks better. A recent series put the overall complication rate at about 23%, with an overall mortality of under 7%, and showed the operation can now be done safely as a day case, with no worse complication or death rate than an overnight stay (Shubert and Ganjei, 2023). It's worth knowing the tie-back earned its place at the front of the queue: against an alternative procedure (bilateral ventriculocordectomy), the alternative needed more revision surgery and was more prone to chronic breathing problems and aspiration, which is part of why unilateral tie-back is the standard rather than the fallback (Bahr et al., 2014). Read all of that as "real but mostly manageable risks, in experienced hands", not "a coin toss".
Managing without surgery, for the right dog
If your dog's signs are mild, or an anaesthetic is genuinely risky for other reasons, or surgery simply isn't the right call for your circumstances, managing conservatively is a legitimate plan, not a failure to act.
The levers are practical. Keeping the dog lean is the single biggest one you control, because every extra kilo asks more of a compromised airway. Beyond that: avoid heat, hard exertion and the over-excitement that tips a borderline airway into a crisis, and use a harness rather than a collar so there's no pressure on the windpipe. During a flare, your vet can buy time with sedation and a short course of corticosteroids, which the professional references describe as effective temporarily in mild cases (Kemp, 2022). The heat-and-exercise side of prevention is enough of a life-saver to deserve its own guide, laryngeal paralysis heat and exercise safety.
Two limits, so nobody is lulled. Conservative care manages signs, it does not fix the obstruction or halt progression, so a dog on this path needs close monitoring for deterioration and must avoid heat stress (Willows Veterinary Centre and Referral Service, n.d.). And on tablets: doxepin is sometimes tried, but the only randomised, placebo-controlled trial, in 22 Labradors, found it did not improve any measure of owner-assessed quality of life over placebo, and the placebo dogs actually edged ahead on overall health (Rishniw et al., 2021). It's reasonable to try in a mild dog, but it is not a reliable substitute for surgery in a dog who is already having breathing crises, and I'd be wary of anyone who sells it as one.
Does operating actually beat not operating?
This is the question that turns the decision from a gamble into a judgement, and there is real evidence to answer it. In an owner-perception study of 76 dogs with late-onset laryngeal paralysis, 94% of owners felt the disease affected their dog's quality of life, and among those whose dog had since died, 47% felt it was a large contributing factor in that death (Sample et al., 2020). Sobering figures. But the same study held the answer that matters here: the dogs that had the tie-back surgery were reported to have a better quality of life, and a smaller contribution of the disease to their death, than the dogs that did not (Sample et al., 2020).
Pair that with a word about the main complication. Aspiration pneumonia, the thing that frightens owners most, is becoming less and less commonly fatal, and dogs can recover fully even from severe episodes with prompt treatment (American College of Veterinary Surgeons, n.d.); in that classic series, six of the seven dogs that developed post-operative pneumonia recovered (Hammel et al., 2006). So the balanced bottom line: for a symptomatic, crisis-prone dog, surgery carries real risk, but the weight of evidence is that it improves life and is often the kinder choice. For a mildly affected dog, it's entirely reasonable to wait, manage and keep a close eye, holding surgery in reserve for if and when the breathing demands it.
What it costs in the UK, and how the pathway runs
This is the part that's hard to pin down online, especially from the big US resources, so let me be concrete and UK-specific, while flagging that every figure here is a practical estimate that varies by centre and by what's included.
The pathway runs through your own vet, who refers you to a soft-tissue surgery specialist at a referral hospital. The work-up there usually includes a consultation, an airway assessment under a light plane of anaesthesia to confirm the larynx genuinely isn't moving, chest X-rays to check for any pre-existing pneumonia or a slack gullet (megaoesophagus), the tie-back itself, and a short hospital stay, often one to two nights, though more centres now offer it as a day case (North Downs Specialist Referrals, n.d.; North West Veterinary Specialists, n.d.).
On cost, UK referral fixed-price packages currently run from around £3,300 at the lower end to around £5,000 to £5,300 at the higher end. As real published examples, one centre lists £3,300, including bloods, the anaesthetic, surgery, IV medication, a chest radiograph, a day's hospitalisation and post-op medicines (North West Veterinary Specialists, n.d.), and another lists £5,275, including the consultation, radiography, the airway assessment, the surgery and up to two nights in hospital (North Downs Specialist Referrals, n.d.). Two things to note. First, this is materially dearer than the flat-faced (BOAS) surgery figure you'll see elsewhere on this site, around £2,000 to £3,000, so don't anchor on the BOAS number. Second, these packages typically do not cover the cost of treating a complication, and a CT scan, if needed, adds roughly £1,300 to £1,400 (North Downs Specialist Referrals, n.d.; North West Veterinary Specialists, n.d.). Prices change, so treat it as a ballpark, not a quote. (For orientation only: the US community larparlife.com quotes roughly $4,500 in the US and about €2,000 in Europe with diagnostics on top, which mainly tells you there's no single global price (larparlife.com, n.d.).)
How to decide, and what to ask
So here's how I'd arrive at an answer with confidence rather than dread.
Start by being clear-eyed about where your dog sits on the breathing scale. A dog who is genuinely struggling, who has had a crisis, or who is one warm walk away from one, is the dog the evidence supports operating on. A dog who snores a bit and tires sooner than he used to, but is otherwise managing, is a dog you can reasonably keep lean, keep cool and watch, with surgery held in reserve.
Then, when you meet the surgeon, take real questions. How many of these do you do? Day case or overnight, and why for my dog? What is your own aspiration-pneumonia rate, and how do you reduce it? What's the feeding and water plan afterwards? What is, and isn't, in the fixed price? And will my insurance cover it? A good surgeon will welcome every one. While you're deciding or recovering, it's genuinely useful to log exercise tolerance and any coughing fits in the airway diary, so the pattern, rather than your memory at 11pm, guides the next conversation.
References
- American College of Veterinary Surgeons. (n.d.). Laryngeal paralysis. Retrieved from
- Bahr, K. L., Howe, L., Jessen, C., & Goodrich, Z. (2014). Outcome of 45 dogs with laryngeal paralysis treated by unilateral arytenoid lateralization or bilateral ventriculocordectomy. Journal of the American Animal Hospital Association, 50(4), 264-272.
- Hammel, S. P., Hottinger, H. A., & Novo, R. E. (2006). Postoperative results of unilateral arytenoid lateralization for treatment of idiopathic laryngeal paralysis in dogs: 39 cases (1996-2002). Journal of the American Veterinary Medical Association, 228(8), 1215-1220.
- Kemp, M. H. (2022). Laryngeal paralysis in dogs and cats. MSD Veterinary Manual. Retrieved from
- larparlife.com. (n.d.). The cost of laryngeal paralysis. Retrieved from
- MacPhail, C. M., & Monnet, E. (2001). Outcome of and postoperative complications in dogs undergoing surgical treatment of laryngeal paralysis: 140 cases (1985-1998). Journal of the American Veterinary Medical Association, 218(12), 1949-1956.
- North Downs Specialist Referrals. (n.d.). Ear, nose and throat surgery fixed prices. Retrieved from
- North West Veterinary Specialists. (n.d.). Soft tissue fixed prices. Retrieved from
- Rishniw, M., Sammarco, J., Glass, E. N., & Cerroni, B. (2021). Effect of doxepin on quality of life in Labradors with laryngeal paralysis: A double-blinded, randomized, placebo-controlled trial. Journal of Veterinary Internal Medicine, 35(4), 1943-1949.
- Sample, S. J., Stilin, A., Binversie, E. E., Baker, L. A., & Hardie, R. J. (2020). Late-onset laryngeal paralysis: Owner perception of quality of life and cause of death. Veterinary Medicine and Science, 6(3), 306-313.
- Shubert, M. P., & Ganjei, J. B. (2023). Outcome following elective unilateral arytenoid lateralization performed in an outpatient manner is comparable to hospitalization for dogs with laryngeal paralysis. Journal of the American Veterinary Medical Association, 261(9), 1-6.
- Southfields Veterinary Specialists. (n.d.). Laryngeal paralysis. Retrieved from
- Willows Veterinary Centre and Referral Service. (n.d.). Laryngeal paralysis. Retrieved from
- Wilson, D., & Monnet, E. (2016). Risk factors for the development of aspiration pneumonia after unilateral arytenoid lateralization in dogs with laryngeal paralysis: 232 cases (1987-2012). Journal of the American Veterinary Medical Association, 248(2), 188-194.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing breathing & airways. Free to join.
Join PetsLikeMine