Weight, Muscle and the Long Game
Claire Greenway
BVM&S MRCVS
Two of the most powerful tools in orthopaedic medicine sit in your hands at home, and neither needs a prescription or a referral. By the point most owners reach this article the big decisions are already behind them. The surgery is done, or the conservative plan is underway, and the worst of the worry about whether you chose well has passed. What's left is a quieter, longer question: from here on, what can you actually do to give this dog the best possible decade? That's the question I love being asked, because the honest answer is so encouraging.
Those two tools are weight and muscle. Between them they do more for both of your dog's knees, and for the arthritis the affected joint will carry for life, than almost anything else once the surgical decision is made. They're not glamorous. Nobody writes a dramatic forum post about keeping their Labrador lean. But the evidence behind them is some of the strongest in canine medicine, and once you see the size of the effect you'll never look at the food bowl or the daily walk the same way again.
A quick word on where this piece sits. If you want the actual odds that the other knee will go too, that's the job of Will the Other Leg Go Too?, and I won't re-tread the numbers here. What I'll say plainly is this: cruciate disease in dogs is a degeneration of the whole dog, not bad luck in one joint, which is exactly why weight and muscle protect both stifles at once. The same lever that looks after the operated knee lowers the load on the other one.
Weight: the biggest lever
I'll start with the most under-appreciated fact in this whole space. Carrying extra weight is not just more kilos pressing through a sore joint, though it is certainly that. Fat is not inert padding. Adipose tissue is an active endocrine organ that secretes pro-inflammatory signalling molecules called adipokines, which means an overweight dog is running a low-grade inflammatory state throughout the body, on top of the purely mechanical extra load (German et al., 2018). So excess weight loads the joint and stokes the very inflammation that drives arthritis. It works on two fronts at once, and that's why getting it right matters so much in a knee that's already on the back foot.
It also genuinely raises the risk of cruciate trouble in the first place. In a database of more than 1.2 million dogs, body weight was an established risk factor for cranial cruciate ligament deficiency, with heavier dogs and dogs over about four years of age carrying higher odds (Witsberger et al., 2008). Breed, conformation and neuter timing matter too, and the full risk-factor story is laid out in Which Dogs Get It?. But of everything on that list, weight is the one you can actually change, which is what makes it the lever rather than the verdict.
Weight loss on its own, with nothing else added, measurably reduces lameness. In a controlled trial of obese dogs with osteoarthritis, lameness scores fell significantly once the dogs had lost around 6.1% of their body weight, and objective gait analysis confirmed the improvement from about 8.85% (Marshall et al., 2010). An earlier study in dogs with hip arthritis found the same: a body-weight loss of 11 to 18% produced a significant improvement in lameness from weight reduction alone (Impellizeri et al., 2000). A single-figure percentage of body weight, turning a limp into a better walk, with no new drug and no second operation. Nothing but a lighter dog.
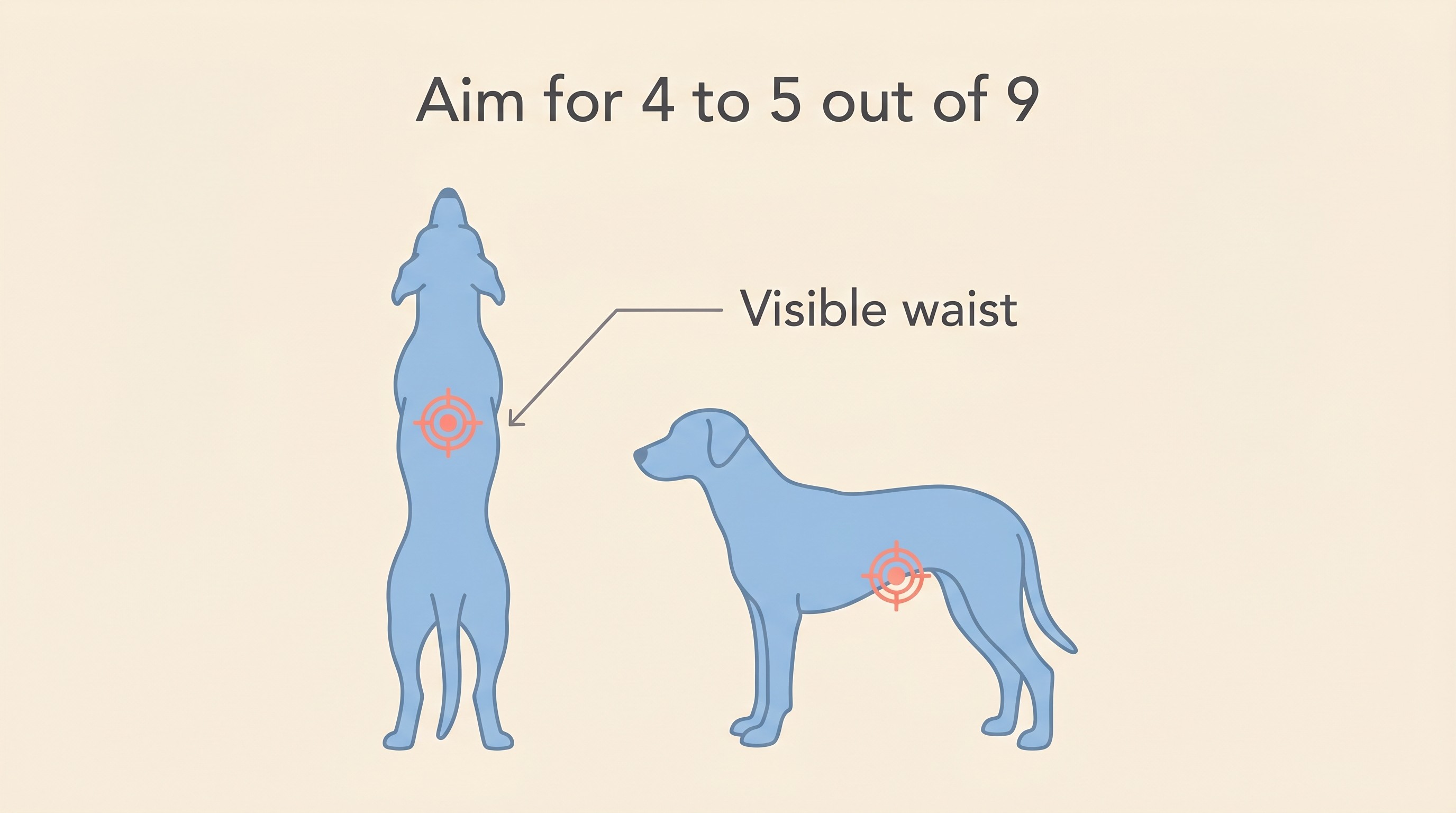
If that has you reaching for the scales, put them down. The scales give a number that means little without context, because the right weight for an individual dog depends on its frame, not its breed average. The tool I'd give you instead is body condition score, a nine-point scale where you're aiming for a 4 to 5 out of 9. You're looking for three things you can check at home: feel the ribs easily without pressing through a layer of fat, see a waist when you look down from above, and see the belly tuck up from the side. Learn those three checks and you can monitor your dog's condition every week. The 2-Minute Mobility Check at /tools/mobility-check is a good companion, giving you a way to baseline how the leg is functioning so you can see the long game moving in the right direction.
I also want to take the guilt out of this, because guilt helps nobody. If your dog is carrying a little too much, you are emphatically not a bad owner: in UK first-opinion practice, roughly 59% of dogs were overweight or obese, made up of 38.9% overweight and 20.4% obese (Courcier et al., 2010). Overweight is the norm in this country, not the exception. None of that is a reason to shrug; it's a reason to act without shame, because the fix is in your hands.
And the long-view evidence is genuinely landmark. In a lifelong study, Labradors fed 25% less than their littermates from puppyhood, and kept lean for their whole lives, developed less osteoarthritis and developed it later (Kealy et al., 2006). The same cohort lived a median of around 1.8 years longer, with the onset of chronic disease pushed further down the road (Kealy et al., 2002). Leanness, then, is not a cosmetic preference. It buys comfort and it buys time. For a dog whose knee is already going to carry arthritis, that is about the most valuable thing you can give.
Weight management does sometimes mean a prescription weight-loss diet, which can run somewhere around 60 to 90 pounds a month for a medium-sized dog in the UK: a rough practical estimate, not a peer-reviewed figure. The deep mechanics of diet choice, calorie maths and feeding plans are exactly what the Arthritis and Mobility hub is built for, and I'll point you there at the end.
Muscle matters
If weight is about taking load off the joint, muscle is about giving the joint its own support. The thigh muscles, the quadriceps in particular, are the knee's live stabilisers. They hold and steady that joint through every step, and here's the catch: they waste fast. Thigh muscle atrophy is a recognised, measurable feature of cruciate disease itself and of the enforced rest that follows surgery. Thigh circumference falls within a few weeks of a limb being used less, which is why "thigh circumference" or "muscle atrophy" is a standard scored item on the instruments vets use to grade stifle function.
You'll see eye-watering percentages thrown around online for how much muscle a dog loses and how fast. I'm not going to give you a number, because the dramatic figures trace back to supplement marketing rather than primary research, and I'd rather tell you the true direction than a tidy fabrication. Use the leg less and the muscle melts away quicker than most owners expect, and that lost muscle was helping to hold the joint together. Rebuilding it, and then keeping it, supports the operated knee and protects the other leg that's now quietly taking on more of the work.
Muscle is built and held through consistent, controlled movement, not through rest. The detailed rebuilding work belongs to other articles: the structured physiotherapy and hydrotherapy that rebuild a post-op leg are covered in Physiotherapy and Hydrotherapy After Cruciate Surgery, and the phase-by-phase home exercises live in Home Exercises by Recovery Phase. What this article owns is the lifelong habit those programmes hand you on to: once your dog is through formal rehab, the muscle is yours to maintain, and you maintain it by keeping the leg working steadily for the rest of the dog's life.
There's good evidence that pairing the two levers beats either alone. In overweight arthritic dogs, caloric restriction combined with a structured physiotherapy programme improved mobility and ground-reaction-force symmetry on force-plate testing, and it actually helped the dogs lose weight more effectively than dieting on its own (Mlacnik et al., 2006). So the message is not to wrap the dog in cotton wool and starve it thin. Feed it lean and keep it moving, because the two reinforce each other.
Sensible activity, not cotton wool
This is where owners most often go wrong, in two opposite directions. One group, frightened of doing damage, retires the dog to the sofa, and the muscle wastes and the joint stiffens. The other, relieved the dog is feeling better, lets it return to weekend-warrior bursts of ball-chasing and hard turns, which spike the load on a degenerating joint exactly when it's least able to cope. Both extremes do harm. The target sits squarely in the middle.
The right kind of exercise is regular, controlled and low-impact: steady lead walks that gradually build in length, gentle conditioning, and hydrotherapy where your vet or physio thinks it's appropriate. What you're avoiding is the explosive, twisting, stop-start activity, the fetch sessions and sudden sprints after a squirrel, that send a shock load through the knee. Consistency is the whole game: a dog walked sensibly every day is being protected, and a dog that does nothing all week and then runs flat out on Sunday is being set up for trouble.
I'd be doing you a disservice if I pretended this work makes the leg perfect, so let me be straight about the ceiling. Even after good surgery, objective force-plate testing has shown that only a minority of dogs end up truly indistinguishable from a normal dog: around 11% after TPLO and 15% after lateral suture in one careful study (Conzemius et al., 2005). The great majority do very well functionally and live happy, active lives, but "back to factory perfect" is not what we're promising. None of that calls for gloom. It's precisely why the lifelong weight and muscle work matters so much: the joint isn't flawless, so we give it every other advantage we can, and a lean, well-muscled dog has those advantages in spades. The same logic runs through the conservative-management evidence in cruciate dogs, where weight loss and controlled exercise form the shared backbone of care whatever route was chosen (Wucherer et al., 2013).
While you're keeping the operated leg in good shape, keep half an eye on the other one. The early signs in the second knee, the subtle sit-test and the intermittent limp, are exactly what Spotting Early Signs in the Other Knee teaches you to catch. Proactive watching and proactive weight and muscle work are two halves of the same sensible habit.
One last reassurance: this whole long-game framing is a dog story. Cats do occasionally rupture a cruciate, but it's uncommon and usually the result of genuine trauma, so the slow degenerative picture and the lifelong levers I've described really belong to dogs.
So here's where the long game leads. A dog kept lean and well-muscled protects both knees, carries its inevitable stifle arthritis more comfortably, and on the best evidence we have, simply ages better. You don't need to do anything heroic, just be quietly, consistently good at two things for years. When you're ready to go deeper on the how, on weight-loss programmes, diet choice, body-condition coaching and conditioning plans, the Arthritis and Mobility hub is your ongoing home for all of it, and the natural next step is the lifelong arthritis picture your work here is feeding into. You've already made the big decisions. This is the part where steady beats dramatic, and you're in full control of it.
References
- Conzemius, M. G., Evans, R. B., Besancon, M. F., et al. (2005). Effect of surgical technique on limb function after surgery for rupture of the cranial cruciate ligament in dogs. Journal of the American Veterinary Medical Association, 226(2), 232–236.
- Courcier, E. A., Thomson, R. M., Mellor, D. J., & Yam, P. S. (2010). An epidemiological study of environmental factors associated with canine obesity. Journal of Small Animal Practice, 51(7), 362–367. PMID 20402841.
- German, A. J., et al. (2018). Dangerous trends in pet obesity. Veterinary Record, 182(1), 25. (Summarising Loftus, J. P., & Wakshlag, J. J. (2014). Canine and feline obesity: a review of pathophysiology, epidemiology, and clinical management. Veterinary Medicine: Research and Reports, 6, 49–60.)
- Impellizeri, J. A., Tetrick, M. A., & Muir, P. (2000). Effect of weight reduction on clinical signs of lameness in dogs with hip osteoarthritis. Journal of the American Veterinary Medical Association, 216(7), 1089–1091. PMID 10754668.
- Kealy, R. D., Lawler, D. F., Ballam, J. M., et al. (2002). Effects of diet restriction on life span and age-related changes in dogs. Journal of the American Veterinary Medical Association, 220(9), 1315–1320. PMID 11991408.
- Kealy, R. D., Lawler, D. F., Ballam, J. M., et al. (2006). Lifelong diet restriction and radiographic evidence of osteoarthritis of the hip joint in dogs. Journal of the American Veterinary Medical Association, 229(5), 690–693. PMID 16948575.
- Marshall, W. G., Hazewinkel, H. A. W., Mullen, D., et al. (2010). The effect of weight loss on lameness in obese dogs with osteoarthritis. Veterinary Research Communications, 34(3), 241–253. PMID 20237844. DOI 10.1007/s11259-010-9348-7.
- Mlacnik, E., Bockstahler, B. A., Müller, M., et al. (2006). Effects of caloric restriction and a moderate or intense physiotherapy program for treatment of lameness in overweight dogs with osteoarthritis. Journal of the American Veterinary Medical Association, 229(11), 1756–1760. PMID 17144822.
- Witsberger, T. H., Villamil, J. A., Schultz, L. G., et al. (2008). Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. Journal of the American Veterinary Medical Association, 232(12), 1818–1824.
- Wucherer, K. L., Conzemius, M. G., Evans, R., & Wilke, V. L. (2013). Short-term and long-term outcomes for overweight dogs with cranial cruciate ligament rupture treated surgically or nonsurgically. Journal of the American Veterinary Medical Association, 242(10), 1364–1372. DOI 10.2460/javma.242.10.1364.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentKeep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing cruciate ligament disease. Free to join.
Join PetsLikeMine