
Is Cataract Surgery Right for My Pet? A Decision Guide
Claire Greenway
BVM&S MRCVS
Your vet has said the word cataract, and now you're trying to work out whether to operate. The search results don't help much. On one side sit the websites with a stock photo of a bright-eyed dog and a headline promising to restore your pet's sight, with a price quietly bolted on. On the other are the forums, where for every "best money I ever spent" there's a "wish we'd never bothered". What you want is a straight answer from someone who isn't selling you anything, so let me try to give you one.
Three things are true at once. Surgery is the only way to give a pet back the sight a cataract has taken, and it works well, around 90 to 95% of eyes regain useful vision in the early days afterwards (MSPCA-Angell, n.d.; Cornell Riney, n.d.). It's also a specialist, costly procedure with a real after-care commitment, and it isn't right for every pet. And choosing not to operate is a legitimate, kind decision that a great many pets live well with. None of those three cancels out the others, and holding all of them at once is exactly what the cost-bait and the forum despair both fail to do. What the operation involves and the weeks of recovery are owned by cataract surgery recovery; this piece is the operate-or-not decision itself.
How well does it actually work?
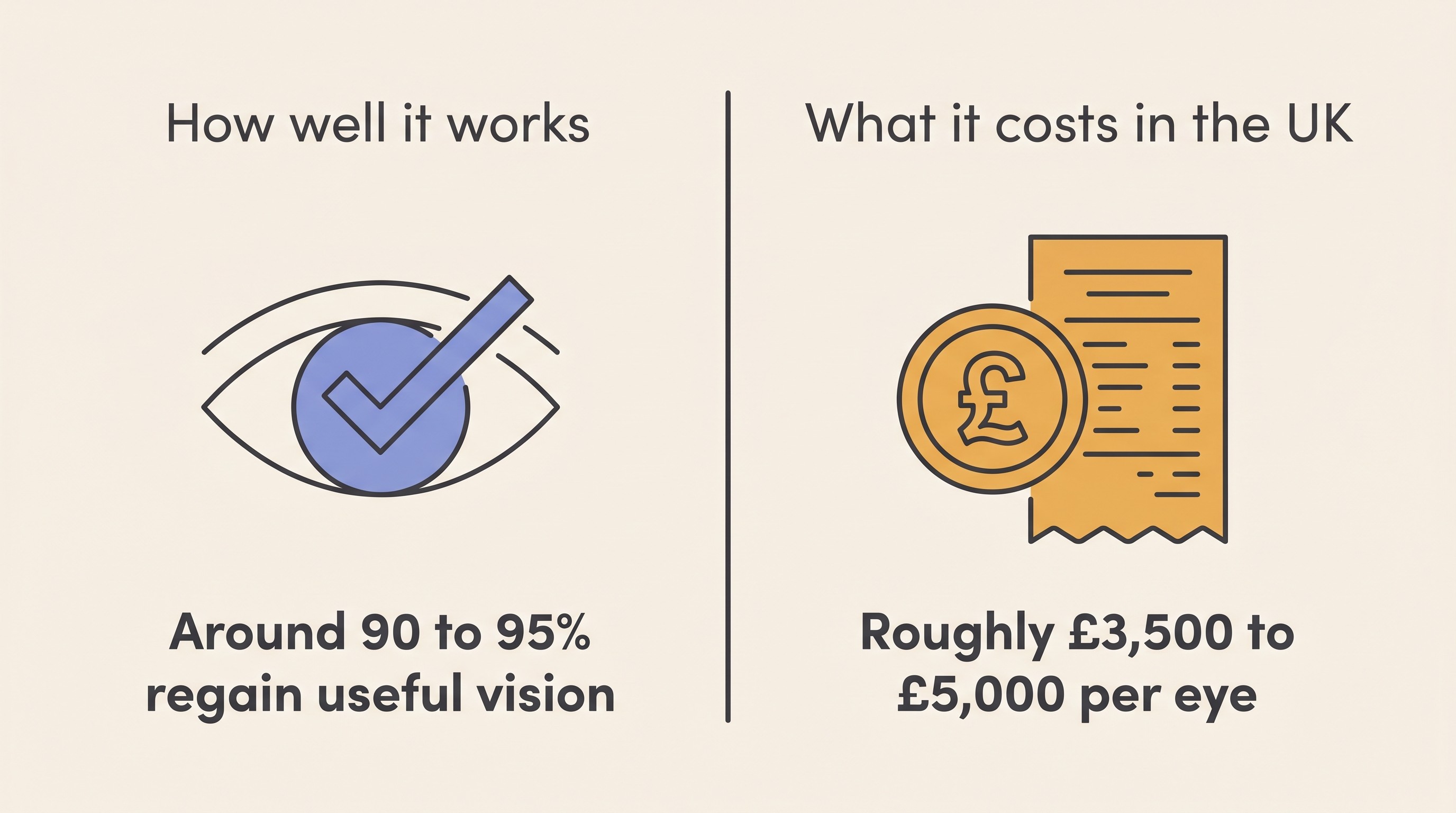
Let me start with the genuine good news, because it gets buried under hedging elsewhere. In a pet that's a good candidate, modern cataract surgery is one of the more reliable procedures in veterinary ophthalmology. The standard operation is phacoemulsification, "phaco" for short: an ultrasonic probe breaks up and removes the cloudy lens through a small incision, and an artificial lens is usually implanted in its place (MSPCA-Angell, n.d.; Cornell Riney, n.d.). Across the major studies, roughly 90 to 95% of eyes regain useful vision in the immediate post-operative period, and a meta-analysis pooling nine studies put the weighted vision-restoration rate at about 86% (MSPCA-Angell, n.d.). Cornell quotes an 80 to 90% success rate for ideal candidates, with better outcomes the sooner surgery is done (Cornell Riney, n.d.).
The word "initially" carries weight, though. That high rate is the early picture, and vision does tail off over the years, maintained in roughly 90% of eyes at one year and around 80% at two (synthesised from Sigle & Nasisse, 2006). That's still a very good result, and the truthful version of it is this: surgery very often gives sight back, in most eyes it lasts for years, but it isn't a permanent guarantee.
Will it work for _my_ pet? The candidacy gate
Here is the clinical heart of the whole decision, and the part the affiliate pages skate over, because it's where some pets get a no.
A cataract is a cloudy lens, and that cloudiness sits right in the surgeon's line of sight to the back of the eye. So before anyone operates, they have to answer something they can't see for themselves by looking in: is the retina behind that cataract actually healthy? If it isn't, removing the cataract just gives you a clear window onto an eye that still can't see. The retina is the film at the back of the camera, and a clean lens in front of a dead film produces no picture.
Two tests do this job. An electroretinogram (ERG) measures whether the retina still responds electrically to flashes of light, and an ocular ultrasound checks it hasn't detached and the eye is structurally sound (Cornell Riney, n.d.; MSPCA-Angell, n.d.). Enough light gets through even a dense cataract to trigger a response from a retina that's still working, which is what makes the ERG possible at all (LKC Technologies, n.d.).
Why does this matter so much? It has a name: progressive retinal atrophy (PRA), an inherited degeneration of the retina, and here lies the cruel overlap. PRA and cataracts can coexist, and a late PRA can itself trigger a cataract that hides the dying retina behind it (ACVO, n.d.; LKC Technologies, n.d.). Operate on that eye and the dog stays blind, because the problem was never really the lens. So when there's PRA, cataract removal isn't recommended, vision won't improve and may even deteriorate (ACVO, n.d.). That's why the retinal work-up comes first, and it's the single biggest thing standing between a pet and the operating table. The disease itself lives in progressive retinal atrophy; here, it's the reason for the tests.
There's one nuance, because I don't want you treating the ERG as a simple pass or fail. A lower-than-ideal reading can come from ageing or from a dense cataract itself, not only from genuine retinal disease (Wegg et al., 2023). So the specialist reads it in the context of the ultrasound and the exam, rather than as one number that decides everything. It's judgement, not a turnstile.
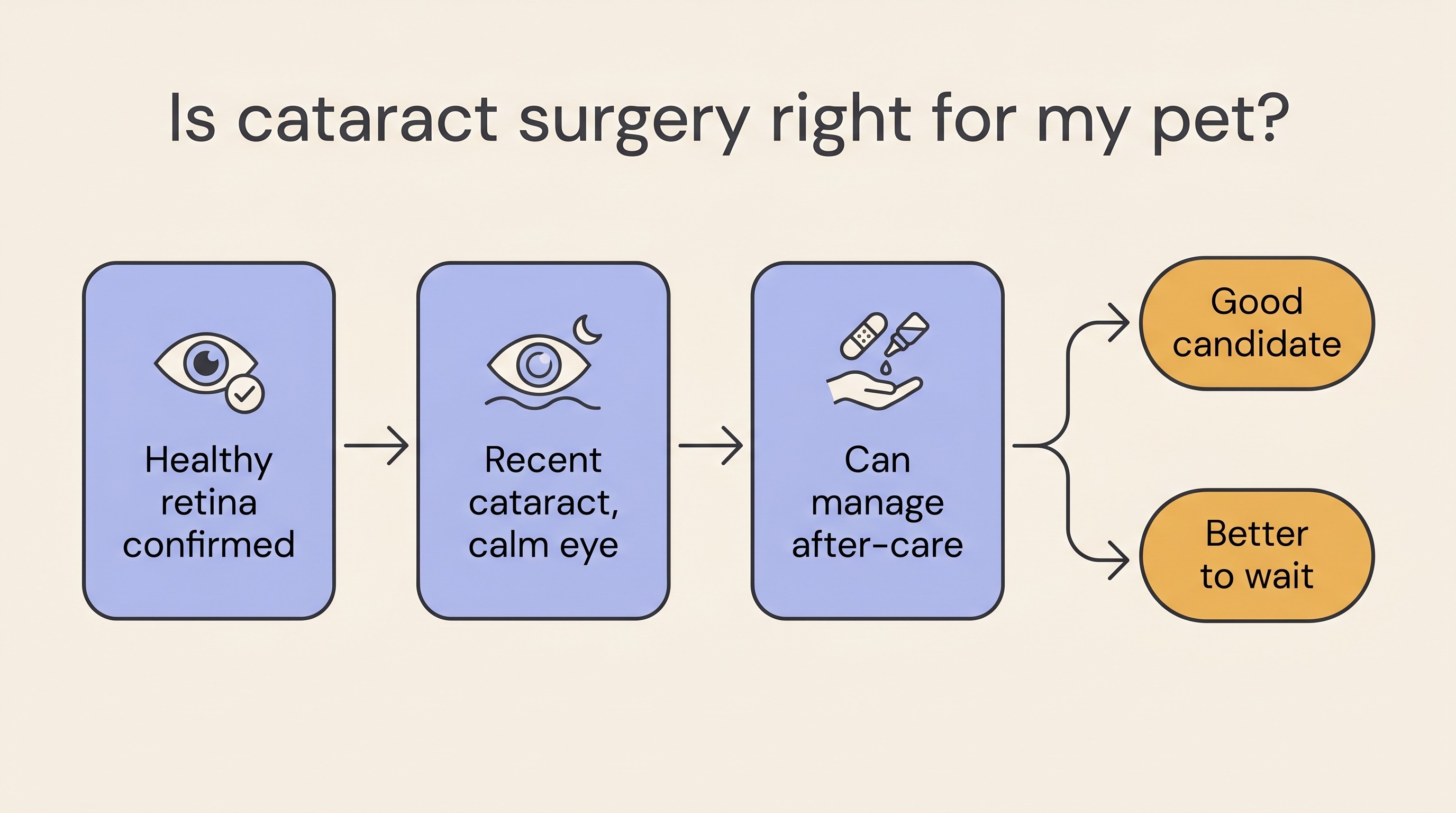
A few other things tip an eye towards being a harder candidate. Best results come from a recent, still-immature cataract in an otherwise healthy eye, when the lens is softer and easier to remove, rather than a long-standing one (Cornell Riney, n.d.; MSPCA-Angell, n.d.). Uncontrolled inflammation inside the eye (lens-induced uveitis) or glaucoma at the time of surgery worsens the odds and usually needs settling first. And very advanced (hypermature) cataracts, along with certain breeds (Boston Terriers, Cocker Spaniels, Cocker-Poodle crosses and Shih Tzus), carry a higher risk of post-operative glaucoma (Sigle & Nasisse, 2006). Then there's the practical question that has nothing to do with the eye: can your pet cope with weeks of frequent drops, a cone and enforced rest, and if it's diabetic, is the diabetes stable? The final yes or no is the specialist's, made on the day from the exam, ERG, ultrasound and a look at the drainage angle (Cornell Riney, n.d.; MSPCA-Angell, n.d.).
The complication picture, in full
If I tell you it works well, I owe you the other side, otherwise "works well" is just marketing. The two serious complications to know are post-operative glaucoma and retinal detachment. The most common one, posterior capsular opacification (a clouding of the capsule the lens sat in), is usually mild and often doesn't limit vision at all.
In the landmark long-term series of 172 dogs, glaucoma became more common with time but stayed under 10% until after the first year, retinal detachment was uncommon at 1 to 2% across all time periods, and outright failure (a blind or lost eye) stayed under 10% until after three years (Sigle & Nasisse, 2006). Pooled estimates land in the same place: glaucoma around 11%, retinal detachment around 4%, most of the capsular clouding mild (MSPCA-Angell, n.d.). The summary I'd give across the consulting-room table is this: roughly one eye in ten runs into a significant complication over time, and the serious ones are glaucoma and detachment. The full watch-list belongs to cataract surgery recovery; the point here is just that the risk is real, modest, and part of the decision.
What it asks of you afterwards, and what it costs
Two practical realities decide this as much as any clinical fact: the after-care and the money.
The after-care is genuine work, and part of what you're signing up for. After day-case surgery there are several eye drops several times a day tapering over weeks, a cone worn at all times, rest with no rough play, and a recheck the day after followed by a schedule of follow-ups, with healing over roughly six to eight weeks and some eyes staying on a drop long term (Cornell Riney, n.d.). The week-by-week belongs to cataract surgery recovery, but I'll be plain: if a heavy drop schedule on a wriggling pet sounds impossible for your household, that's a real factor, not a small one, and the Eye-Drop & IOP tracker exists to make it manageable.
Now the cost, said straight. As a practical UK estimate, cataract surgery runs roughly £3,500 to £5,000 per eye, varying by centre and by the individual eye. Published referral fixed prices show the spread: Paragon Referrals quote £4,750 for one eye and £6,300 for both, while North Downs quote around £6,200 for one and £7,900 for both (Paragon Referrals, n.d.; NDSR, n.d.). Many centres bundle the consultation, the pre-operative ERG and ultrasound, the anaesthetic, the surgery, a night or two of hospitalisation and a post-op check into that package (Paragon Referrals, n.d.). Two footnotes worth keeping in mind: both eyes and the work-up add to the figure, and while insurance often contributes, owners without cover are usually asked to pay in full on admission (Paragon Referrals, n.d.). This is the most expensive eye procedure there is, so it's almost always done at a referral centre, not your local practice.
Choosing not to operate is a real choice, not a failure
Here is the beat I most want you to take away, because it's where the kindest medicine and the actual evidence happen to agree. If you decide against surgery, on cost, on candidacy, on your pet's age or health, or simply because it isn't the right call for your household, you have not let your pet down.
The evidence backs that up, not just my reassurance. In a direct comparison, the overall complication rate in cataract eyes managed without surgery (20.8%) was not significantly different from the operated eyes (18.3%), and the eyes that did worst weren't the ones owners chose to manage without surgery, they were the ones an ophthalmologist had judged poor surgical candidates in the first place (Krishnan et al., 2020). Add the thing I see every week in practice: sight loss from a cataract is rarely painful in itself, and pets adapt remarkably well to losing their vision, especially when it comes on gradually. A pet living with cataracts can have a genuinely good life.
I'll keep one counterpoint in view, because pretending otherwise would mislead you. Without surgery the eye does not get its sight back: in diabetic eyes managed on medication alone, only about 7.6% recovered any vision, and that was through the cataract slowly resorbing rather than anything we did (Lee et al., 2023). And an unoperated cataract still needs watching, because it can cause the painful complications (inflammation, glaucoma) described above. So "not operating" isn't "do nothing and forget it". The day-to-day of doing it well, the routine checks, the red flags, supporting a low-vision pet, is owned by living with cataracts without surgery, and the door stays open: if vision loss accelerates and the eye is otherwise healthy, surgery can be revisited.
Two pets the decision looks different for
A couple of situations change the calculus enough to call out.
The diabetic dog: don't wait. If your dog is diabetic, the case for surgery, and for getting referred early, is at its strongest. Most diabetic dogs develop cataracts, around 80% within the first year or so of diagnosis, whatever the glucose control, because it's the sugar in the lens and not anything you did wrong (Beam et al., 1999; Cornell Riney, n.d.). They form fast, often clouding over in weeks, and surgery is best done on a recent cataract in a healthy eye, so the sooner you get seen the better the odds (Cornell Riney, n.d.). And operating works: in one study of diabetic eyes, surgery restored vision in 94.8% of those operated against only 7.6% on medication alone (Lee et al., 2023). The eye angle and the guilt-relief belong to diabetic cataracts, and the glucose-control side sits in our Diabetes space; the only line that matters here is, don't sit on a clouding eye in a diabetic dog, ask about referral promptly.
Cats: a different story. Almost everything above, the success rates, the work-up, the cost, comes from the canine literature, because in dogs this is a common decision. In cats it isn't. Feline cataracts are uncommon and usually secondary to long-standing inflammation inside the eye, so the priority is finding and treating the underlying cause, and surgery is reserved for selected cases. Diabetic cataracts are rare in cats too, so the "operate early" urgency is essentially a dog story. If you've got a cat, cataracts in cats is the piece written for you.
Where this leaves you
What most determines whether surgery is even on the table isn't the price or your nerve, it's the health of the retina hiding behind that cataract, and only an ophthalmologist's exam, ERG and ultrasound can tell you where your pet actually stands. So the genuinely useful next step isn't "think harder about it at midnight", it's a referral consult to find out. Go to it knowing what you want answered: questions to ask about cataract surgery and the matching cataract surgery questions checklist lay out exactly what to bring, so you leave with a real answer about your pet rather than a stock photo and a number. And if you'd like to track your pet's sight before and after that decision, the At-Home Vision Check gives you a repeatable way to see how they're actually doing.
References
- American College of Veterinary Ophthalmologists (ACVO). (n.d.). PRA (Progressive Retinal Atrophy). ACVO Common Conditions.
- Beam, S., Correa, M. T., & Davidson, M. G. (1999). A retrospective-cohort study on the development of cataracts in dogs with diabetes mellitus: 200 cases. Veterinary Ophthalmology, 2(3), 169-172.
- Cornell University College of Veterinary Medicine, Riney Canine Health Center. (n.d.). Canine cataracts.
- Krishnan, H., Hetzel, S., McLellan, G. J., & Bentley, E. (2020). Comparison of outcomes in cataractous eyes of dogs undergoing phacoemulsification versus eyes not undergoing surgery. Veterinary Ophthalmology, 23(2), 286-291.
- Lee, E., Kang, S., Jeong, D., & Seo, K. (2023). Comparison of the outcomes of phacoemulsification versus topical medication alone in canine diabetic cataracts: a retrospective study. Journal of Veterinary Science, 24(6), e86.
- LKC Technologies. (n.d.). Animal Clinical Applications of Electroretinography (ERG).
- MSPCA-Angell (Angell Animal Medical Center). (n.d.). Lifting the Veil: Canine Cataracts & Cataract Surgery.
- North Downs Specialist Referrals (NDSR). (n.d.). Ophthalmology Fixed Prices.
- Paragon Veterinary Referrals. (n.d.). Fixed Pricing: Ophthalmology.
- Sigle, K. J., & Nasisse, M. P. (2006). Long-term complications after phacoemulsification for cataract removal in dogs: 172 cases (1995-2002). Journal of the American Veterinary Medical Association, 228(1), 74-79.
- Wegg, M. L., Pollard, D., & Ofri, R. (2023). Retrospective evaluation of pre-surgical electroretinography results in a mixed-breed canine population presented for cataract removal surgery. Veterinary Ophthalmology, 26(2), 145-154.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing vision & eye health. Free to join.
Join PetsLikeMine