
Vomiting or regurgitation? Why the difference matters
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
"He's been sick." It is one of the most common sentences I hear across the consulting table, and it sounds perfectly clear. But it carries at least three quite different things tucked inside it, and which one your pet is actually doing tells me more, before I have laid a hand on them, than almost anything else you can say. Vomiting and regurgitation look alike but point at completely different parts of the body, and the work-up goes down a different road for each.
It is a distinction owners cannot easily see but can learn to spot. The aim here is simple: to let you tell the two apart, describe what you saw, and film it usefully, so your vet starts from what actually happened.
When "he was sick" hides three different things
Owners use "sick", "vomiting", "bringing it up" and "gagging" more or less interchangeably, because in everyday life they all amount to the same thing: stuff that should have stayed inside has ended up on the floor. Clinically, though, they are not the same event. Vomiting and regurgitation are two distinct presenting problems with two distinct sets of causes, and the standard texts treat them as separate complaints with separate diagnostic approaches (Washabau & Day, 2013; Hall et al., 2019).
This is not pedantry; it is localisation. Getting the word right changes which tests your vet reaches for first. Vomiting opens a wide field, regurgitation narrows it sharply to one organ, and mislabelling one as the other sends everyone looking in the wrong place, which can delay the right diagnosis (Washabau & Day, 2013; Gallagher, 2012).
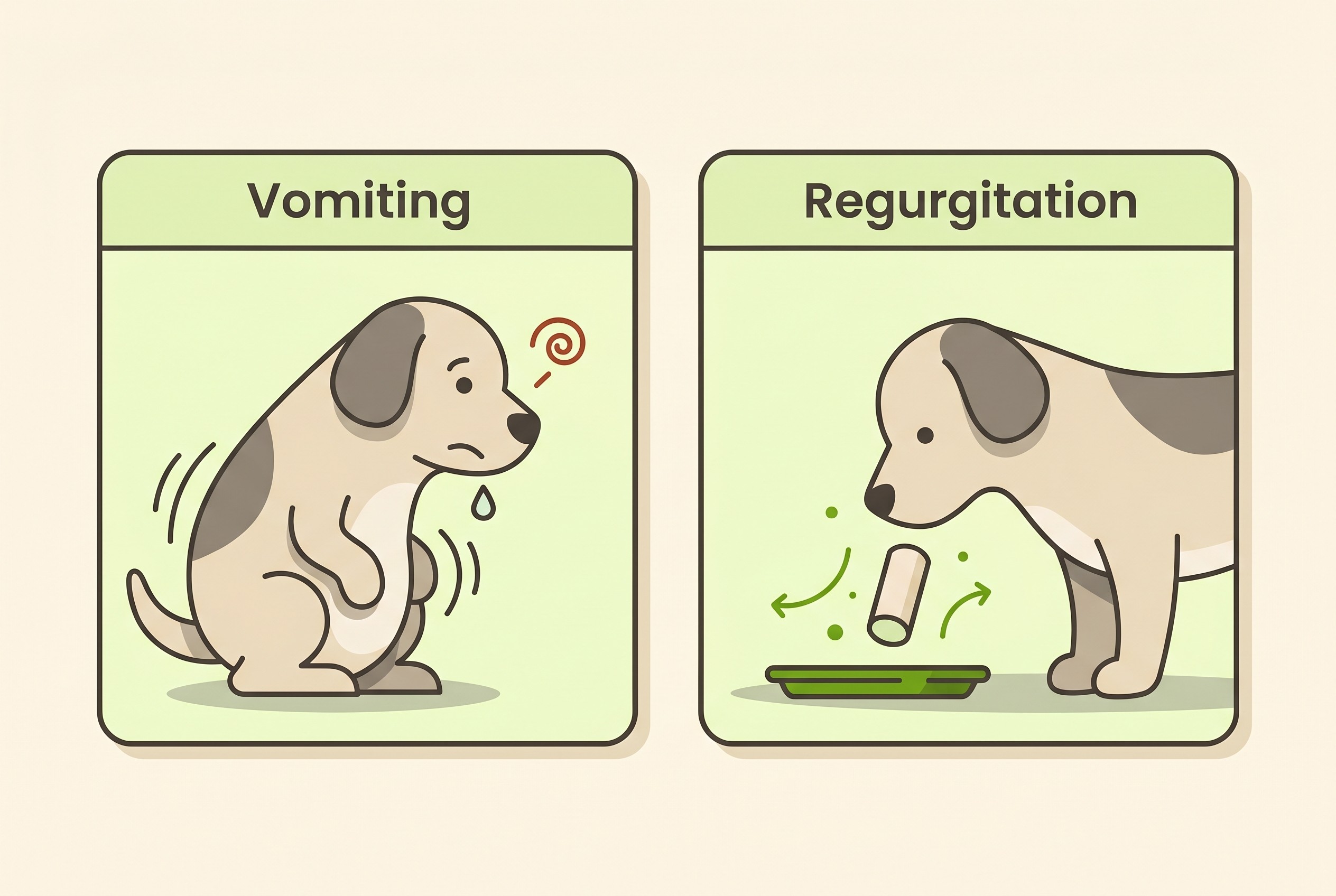
Vomiting: the active heave
Vomiting is something the body actively does. It is a centrally controlled reflex that forcibly expels the contents of the stomach (and sometimes the upper small intestine), in a recognisable sequence (Washabau & Day, 2013; Gallagher, 2012).
First there is a prodrome of nausea. You will often see drooling, repeated lip-smacking or swallowing, restlessness, and that unmistakable apprehensive, hangdog look. Then comes the retching: rhythmic, forceful contractions of the abdominal muscles and diaphragm, the belly visibly bracing and heaving against a closed throat. Then the expulsion, with the airway reflexively protected throughout (Gallagher, 2012). The whole thing has effort and warning written all over it.
So what does it point to? A great deal. Vomiting has a long list of causes, many of them outside the gut altogether, in the kidneys, the hormone system and other organs, which is why your vet screens for organ and hormone disease on bloods rather than only looking at the stomach (Washabau & Day, 2013). I will not list those causes here: the whole differential and the acute-versus-chronic split are covered in my pet is being sick or has diarrhoea, the article that anchors this space. Vomiting widens the picture, it does not narrow it.
Regurgitation: the effortless bring-up
Regurgitation is the opposite: passive and effortless. Material is simply brought back up from the gullet (the oesophagus) or the throat without any abdominal effort, without a nausea prodrome, and usually without any warning at all (Washabau & Day, 2013; Gallagher, 2012). The pet often just lowers its head and the contents fall out, more like an overflow than a heave.
There is one genuinely useful clue in what appears. Because regurgitated material has only ever reached the oesophagus and never the stomach, it contains no bile. It is typically undigested and frequently comes up as a cylindrical, tube-shaped plug coated in clear or frothy mucus and saliva (Washabau & Day, 2013; Gallagher, 2012). Yellow or green bile, by contrast, points towards vomiting. But there is a trap the texts flag explicitly: do not mistake the white froth and saliva of oesophageal disease for bile (Gallagher, 2012). The clean way to hold all this in your head is that vomiting is something the body actively does to itself, while regurgitation is something that just happens.
Clues that fool people
Most of the "is my dog vomiting or regurgitating?" pages online lean on three shortcuts: the timing relative to meals, how digested the material looks, and even the pH of what comes up. The good textbooks and specialists are clear that these are suggestive at best and unreliable at worst.
Timing is not reliable. The folklore says regurgitation happens soon after eating and vomiting comes later. It is only a tendency. A regurgitating animal can passively bring food back up hours after a meal, because food can sit in a poorly-emptying oesophagus, and some dogs vomit very soon after eating. You cannot diagnose on the clock (Armstrong, n.d.).
Degree of digestion is suggestive, not diagnostic. Regurgitated material is usually undigested and vomited material is more often partly digested, but these are tendencies, not proof (Washabau & Day, 2013; Gallagher, 2012).
pH testing is unreliable, and not something to ask owners to do at all. The specialist sources list it among the features that do not reliably tell the two apart (Gallagher, 2012). Do not let anyone convince you that regurgitated material is "always alkaline, never acidic" as a home test, because it simply is not dependable.
So what does hold up? Active abdominal effort. Forceful, repeated contractions of the belly, the heave, are the single most reliable confirmation that you are watching vomiting (Armstrong, n.d.; Gallagher, 2012). If your pet braced and heaved, that is vomiting; if the material just appeared with no effort, that is regurgitation. After effort, the next most useful clue is bile: present points to vomiting, absent (or only white froth) towards regurgitation.
One more bucket deserves a mention, because owners conflate it with both. Dysphagia, meaning difficulty swallowing, points at the mouth, throat or the very top of the oesophagus. It shows as exaggerated or repeated swallowing efforts, dropping food, food or water coming back down the nose, and gagging or coughing when trying to swallow (Gallagher, 2012; Hall et al., 2019). Gagging and coughing in particular are easily mistaken for being sick, when they may actually be a throat or breathing sign. So there is a third possibility, and one more reason to film rather than guess.
The reason regurgitation worries me more
Here is why I take regurgitation seriously rather than shrugging it off. The oesophagus runs right alongside the windpipe. When it cannot clear material reliably, that material can be inhaled into the lungs, causing aspiration pneumonia, the main threat to life when regurgitation becomes a chronic problem (Washabau & Day, 2013; McBrearty et al., 2011).
The figures make the point. In dogs with generalised megaoesophagus (a gullet that has lost its tone), aspiration pneumonia seen on chest X-rays was strongly associated both with dying before discharge and with a shorter survival overall, with a median survival of around 90 days and roughly a quarter of dogs dying before they ever left hospital (McBrearty et al., 2011). That is the disease behind a lot of chronic regurgitation, and the condition itself, its investigation, assisted feeding and outlook are all covered in megaoesophagus and chronic regurgitation.
That gives you a clear safety line. If a pet that brings food back up develops a cough, fast or laboured breathing, a fever, lethargy, or goes off its food, treat that as a ring-the-vet-now sign, because it can mean aspiration; when digestive signs become urgent is covered in the digestive red-flags you must not wait on. And it underlines the distinction that an anti-sickness drug such as maropitant (Cerenia) treats nausea and vomiting but does nothing for regurgitation, because there is no nausea reflex to switch off.
Some pets are built to bring food up
A few pets regurgitate or reflux more readily simply because of how they are made, and it is worth saying so plainly.
Flat-faced (brachycephalic) breeds such as French bulldogs, English bulldogs and pugs have a genuinely high background rate of upper-gut and oesophageal trouble. In a fluoroscopy study of these dogs, hiatal hernia and delayed oesophageal transit were common, every hiatal hernia in the series occurred in a French bulldog, and gastro-oesophageal reflux was significantly more common in flat-faced dogs than in others (Reeve et al., 2017; Eivers et al., 2019). So regurgitation, reflux and gulping in these breeds is common and worth taking seriously rather than dismissing as "just a Frenchie thing".
Cats regurgitate too, and the everyday trap is the hairball. Bringing one up is real, but "she's just being sick with a hairball" is badly over-used. Frequent bringing-up in a cat, hairball or not, is not automatically normal, because chronic vomiting in cats is so often a sign of treatable disease rather than grooming (Norsworthy et al., 2015). The feline side of chronic gut disease is covered in chronic vomiting and gut disease in cats.
What to film and note
This is the part that changes your next appointment. Owner history alone often does not settle it, which is precisely why specialists ask owners to video an episode on a phone, or feed the pet in the consulting room to watch one (Armstrong, n.d.). It is not a failing on your part; it is the recommended approach.

Five things are worth catching:
- Was there effort? Did your pet heave, brace and contract its belly (vomiting), or did the material just come up (regurgitation)? Film the whole episode, including the lead-up.
- Was there a warning? Drooling, lip-smacking, restlessness or repeated swallowing beforehand all suggest nausea, and so vomiting.
- How long after eating? Note it, while remembering that timing alone proves nothing.
- What came up? Undigested or partly digested, any yellow or green bile (as opposed to white froth), a tube-shaped plug, and roughly how much.
- The breathing afterwards. Any coughing or fast, laboured breathing is the aspiration flag to act on.
The wider craft of describing and photographing signs well lives in the how to describe it to your vet guide, which pairs with the Faecal Score Tracker. A short diary there, logging effort, timing and what came up each time, turns a vague "he keeps being sick" into a pattern a vet can act on. And if you are unsure whether this is one to watch or to act on right now, particularly with that breathing flag, our Vomiting & Diarrhoea Triage walks you through the same questions I would ask on the phone.
The single most useful thing you can do before your appointment is to catch one episode on video. A ten-second clip showing whether there was a heave or an effortless bring-up tells your vet, in seconds, which half of the body to investigate first, and you do not need to label it yourself. Just capture it, and let the picture do the talking.
References
- Armstrong, P. J. (n.d.). GI intervention: approach to diagnosis and therapy of the vomiting patient. Today's Veterinary Practice.
- Eivers, C., Chicon Rueda, R., Liuti, T., & Salavati Schmitz, S. (2019). Retrospective analysis of oesophageal imaging features in brachycephalic versus non-brachycephalic dogs based on videofluoroscopic swallowing studies. Journal of Veterinary Internal Medicine, 33(4), 1740-1746.
- Gallagher, A. (2012). Regurgitation or vomiting? Clinician's Brief, June 2012.
- Hall, E. J., Williams, D. A., & Kathrani, A. (Eds.). (2019). BSAVA manual of canine and feline gastroenterology (3rd ed.). BSAVA.
- McBrearty, A. R., Ramsey, I. K., Courcier, E. A., Mellor, D. J., & Bell, R. (2011). Clinical factors associated with death before discharge and overall survival time in dogs with generalized megaesophagus. Journal of the American Veterinary Medical Association, 238(12), 1622-1628.
- Norsworthy, G. D., Estep, J. S., Hollinger, C., et al. (2015). Prevalence and underlying causes of histologic abnormalities in cats suspected to have chronic small bowel disease: 300 cases (2008-2013). Journal of the American Veterinary Medical Association, 247(6), 629-635.
- Reeve, E. J., Sutton, D., Friend, E. J., & Warren-Smith, C. M. R. (2017). Documenting the prevalence of hiatal hernia and oesophageal abnormalities in brachycephalic dogs using fluoroscopy. Journal of Small Animal Practice, 58(12), 703-708.
- Washabau, R. J., & Day, M. J. (Eds.). (2013). Canine and feline gastroenterology. Elsevier Saunders.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine