Megaoesophagus and chronic regurgitation: the condition behind bringing food back up
Dr. Alastair Greenway
MRCVS
By Dr Alastair Greenway MRCVS | Reviewed by Claire Greenway BVM&S MRCVS
Megaoesophagus is uncommon but serious, and the internet tends to handle it with either breezy false cheer or a wall of frightening numbers. This page aims for the measured middle: what is going wrong, why aspiration pneumonia is the real worry, and the practical management you can start at home. If your pet keeps bringing food back up and someone has put that word in front of you, that is the ground we are going to cover.
One quick piece of groundwork. What your pet is doing is almost certainly regurgitation, the effortless, passive bringing-up that points at the oesophagus, rather than true vomiting. That distinction has its own guide, so if you are unsure which you are seeing, read vomiting versus regurgitation first.
What megaoesophagus actually is
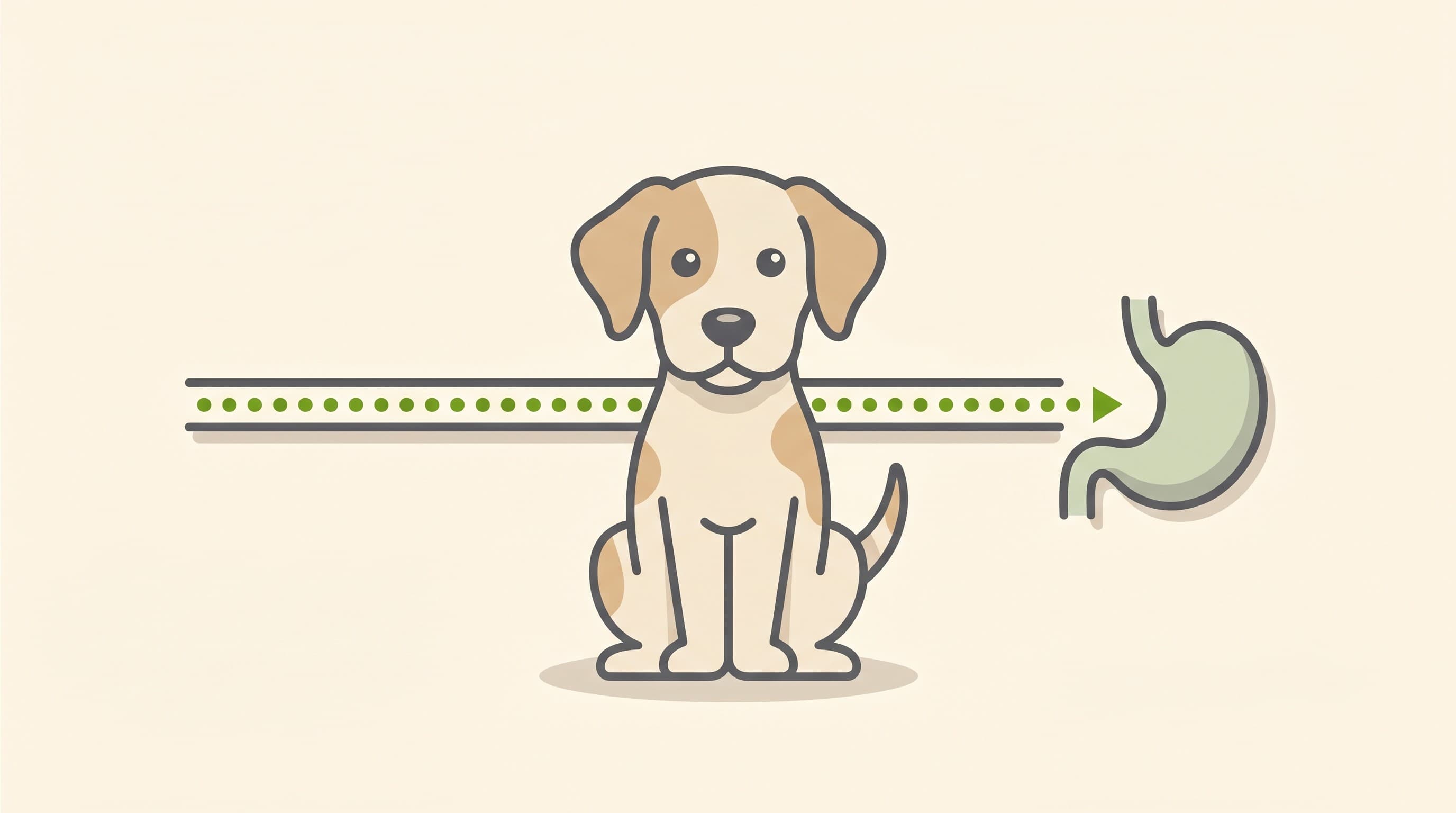
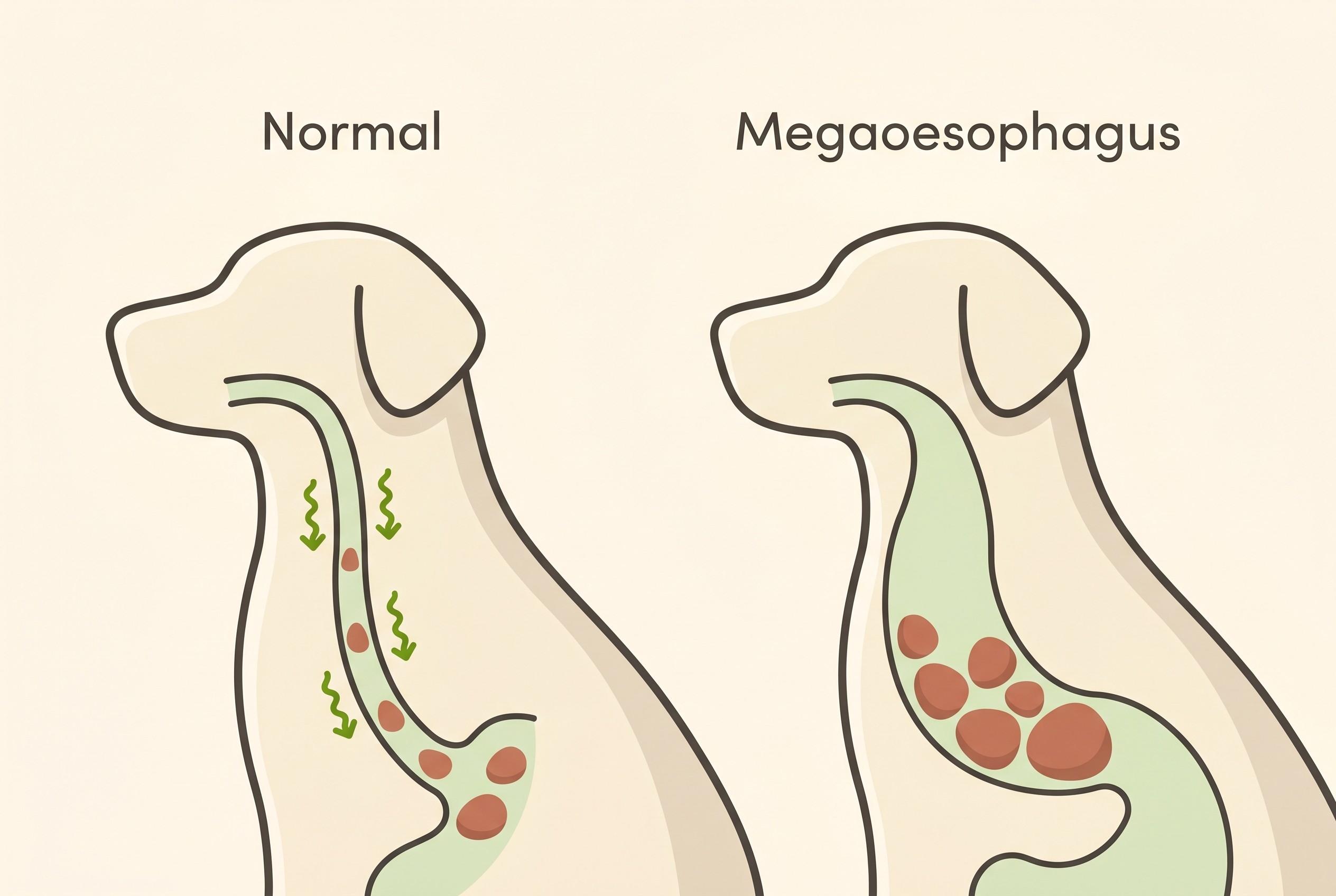
Think of the oesophagus as a muscular conveyor belt: each time your pet swallows, it should grip the mouthful and actively post it to the stomach in a wave called peristalsis. In megaoesophagus that belt has stopped working and stretched out. The formal definition is a diffuse dilation of the oesophagus with decreased peristalsis, so food, water and saliva pool in the floppy, widened tube and are later brought back up (Mace et al., 2012). Gravity becomes the only thing left to move a meal down, and that single idea explains both the regurgitation and the whole logic of the upright feeding I come to later. It is genuinely the most common cause of regurgitation in dogs (Mehain et al., 2022). One caveat: a mildly widened oesophagus can be an incidental finding in an excited, sedated or recently anaesthetised animal, which is why a good vet reads the radiograph alongside the clinical signs (Mace et al., 2012).
Born with it, or developed later
There are two quite different versions, and which one your pet has changes the outlook. Congenital megaoesophagus is present from birth and typically shows itself at weaning, as a puppy moves onto solid food, the suspected mechanism being delayed maturation of the nerves controlling the oesophagus (Mace et al., 2012). Several breeds are predisposed to the congenital form, among them Newfoundlands, Parson Russell terriers, Samoyeds, springer spaniels, smooth fox terriers and Chinese shar-peis (Mace et al., 2012). The German shepherd has its own well-studied congenital form: it is a sex-differentiated trait, with males about twice as likely to be affected as females, and is linked to a specific gene variant, so a genetic test now exists (Bell et al., 2022).
Acquired megaoesophagus develops later, classically in a dog of around seven to fifteen years, and splits into idiopathic cases, where no cause is ever found and which form the largest acquired group, and secondary cases driven by another disease (Mace et al., 2012). A different set of breeds, including Great Danes, Labrador retrievers and miniature schnauzers, shows a higher prevalence of the acquired form (Mace et al., 2012). One exception to the older-dog rule: in a young adult of around two years or under, the condition I describe next is a particular concern (Mace et al., 2012). Cats get megaoesophagus too, with a familial congenital form recognised in Siamese cats, but this is overwhelmingly a canine condition (Mace et al., 2012).
The cause worth chasing: myasthenia gravis (and why not to blame the thyroid)
A diagnosis of acquired megaoesophagus is not an endpoint but a prompt to look for what is driving it, because some causes are treatable. The one to find is myasthenia gravis, the most common identifiable cause, accounting for roughly a quarter of all acquired cases (Mace et al., 2012). It is an autoimmune disease in which antibodies block the acetylcholine receptors that let nerves tell muscles to contract, so muscles, the oesophagus included, become weak (Mace et al., 2012; Koos, 2024). The link runs the other way too: about 90% of dogs with the generalised form have megaoesophagus (Mace et al., 2012). A good vet rules it out first, because unlike idiopathic disease it can be treated and can even remit. Other secondary causes worth considering are Addison's disease and (debatably) hypothyroidism, both of which can cause a reversible megaoesophagus, muscle and nerve diseases such as polymyositis, toxins such as lead, and a physical obstruction like a vascular ring anomaly in a young dog (Mace et al., 2012).
Now the point worth getting right. A lot of online content tells owners "it's probably the thyroid". The truth is more measured: the link between hypothyroidism and megaoesophagus is not established, it occurs in only about 3% of hypothyroid dogs, and although there are reports of it resolving once the thyroid is treated, a causal connection has not been proven (Mace et al., 2012). There is also a trap: serious illness, including aspiration pneumonia, can depress thyroid results and fake a low reading (sick euthyroid syndrome), so check the thyroid by all means, but do not let "it's the thyroid" stop the search for the real driver, myasthenia gravis above all (Mace et al., 2012). If your vet does find a hormonal cause, treating it becomes the priority.
The real danger: aspiration pneumonia
Because the oesophagus sits right beside the windpipe and cannot clear material reliably, the pooled food, water and saliva can be inhaled into the lungs, causing aspiration pneumonia, the most common and most life-threatening complication of megaoesophagus and its usual cause of death (Mace et al., 2012; McBrearty et al., 2011).
The warning signs are the ones I most want you to carry in your head: a moist or productive cough, fast or laboured breathing, fever, lethargy, going off food, or nasal discharge (Mace et al., 2012). In an animal that regurgitates, a new cough or any change in breathing is not "a cold to keep an eye on", it is a "ring the vet now" sign, because it may be pneumonia. The act-now framing and the wider red-flags live in digestive emergencies; my job here is to explain why this sign turns a manageable condition into an emergency. Our Vomiting and Diarrhoea Triage tool helps you sense-check a worrying change, but if breathing is affected, do not wait on a questionnaire, phone your vet. The numbers explain why: in a study of 71 dogs with generalised megaoesophagus, median survival was about 90 days, roughly a quarter (26.7%) died before they even left hospital, and radiographic aspiration pneumonia was significantly linked to both dying before discharge and shorter survival (McBrearty et al., 2011). Those figures sit alongside genuinely hopeful facts below.
Getting the diagnosis
The diagnosis itself is usually more straightforward than owners fear. Megaoesophagus is most often confirmed on plain (survey) chest radiographs showing the dilated, air- or food-filled oesophagus, and most cases need nothing more (Mace et al., 2012). A barium swallow can be added when films are unclear or to look for an obstruction, but it carries its own risk of triggering aspiration, so it is used judiciously (Mace et al., 2012).
The more demanding half, in acquired cases, is the search for the cause. An acetylcholine-receptor (AChR) antibody titre is recommended in every acquired case; it is the standard confirmatory test for acquired myasthenia gravis, with high sensitivity and specificity (Mace et al., 2012; Koos, 2024). One practical point: a course of steroids can lower the AChR antibody level and mask the result, so the sample is ideally taken before any steroids are started (Mace et al., 2012). General bloods, and where indicated an ACTH stimulation test for Addison's and a blood lead level, fill in the rest (Mace et al., 2012).
Feeding for a megaoesophagus: upright, little and often, and finding the right consistency
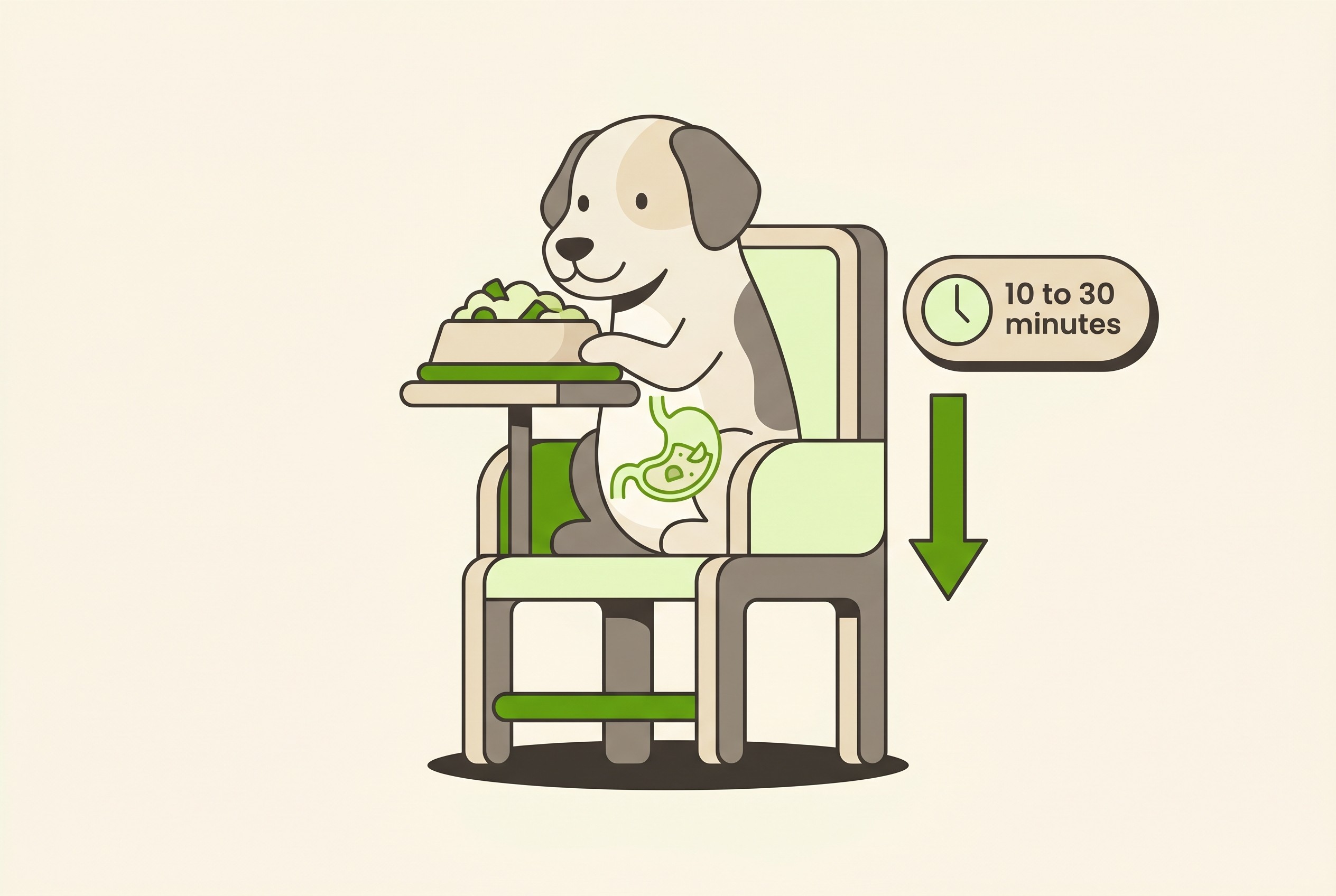
This is the part you can act on today. The cornerstone is feeding small, frequent, high-calorie meals with your pet held upright, and kept upright afterwards, so gravity does the job the oesophagus cannot (Mace et al., 2012). In dogs this is most reliably done with an upright feeding chair, often called a Bailey chair, in which the dog sits vertically to eat and stays there for roughly ten to thirty minutes afterwards to let everything drain into the stomach (Mace et al., 2012). It looks odd at first, but it is the single most important thing most owners do, and most dogs take to it quickly.
The second lever is food consistency, and here is the liberating truth: there is no single "right" texture, because the best one varies from pet to pet (Mace et al., 2012). Some do best on a thin gruel, others on meatball-sized lumps, others on a thicker porridge. One study used videofluoroscopy, a moving X-ray of swallowing, to tailor the diet to each dog with congenital idiopathic megaoesophagus, and found no single consistency cleared the oesophagus best for all of them; when feeding was personalised, regurgitation roughly halved, from about 5.5 to 2.5 episodes a week, and 95% of owners reported improved quality of life (Lyngby et al., 2022). So experiment methodically. You can repurpose our Faecal Score Tracker as a regurgitation diary, logging episodes alongside the consistency and feeding position you used, so the count, not an impression, tells you and your vet what works.
Where a cause is found, treating it is the real lever: anticholinesterase drugs such as pyridostigmine, with low-dose prednisolone or other immune-suppressing treatment if needed, for myasthenia gravis, or thyroid or Addison's treatment where relevant (Mace et al., 2012; Koos, 2024). And if regurgitation cannot be controlled and your pet cannot hold their weight, a feeding tube placed directly into the stomach (a gastrostomy tube) can bypass the oesophagus; it lowers the aspiration risk but does not abolish it, because saliva and reflux remain, so it is a support for harder cases, not a cure (Mace et al., 2012).
What helps, what does not, and the sildenafil question
This is where popular advice most often steers owners wrong. The common gut prokinetics metoclopramide and cisapride (the latter often specially imported or unlicensed here) have no documented benefit in canine megaoesophagus and are not advised in dogs. The reason is anatomical: a dog's oesophagus is striated, skeletal muscle along its whole length, whereas these drugs act on smooth muscle, and worse, they can tighten the lower oesophageal sphincter and so make regurgitation worse (Mace et al., 2012). One genuine dog-versus-cat difference: the lower part of a cat's oesophagus does contain smooth muscle, so cisapride may have a role in feline cases (Mace et al., 2012). What does help is treating oesophagitis (inflammation of the oesophageal lining), which commonly travels with megaoesophagus, typically with acid suppression such as omeprazole alongside the mucosal protectant sucralfate; unlike the prokinetics, that is supportive care that earns its place (Mace et al., 2012).
Then there is the one you have probably read about. Sildenafil, the "Viagra for megaoesophagus" story, is a real area of research, not a proven cure. It relaxes the lower oesophageal sphincter, which could in theory help material pass into the stomach, and one randomised controlled trial in dogs with congenital idiopathic megaoesophagus reported improved clinical signs and radiographic features (Quintavalla et al., 2017). But a later randomised crossover study of ten dogs found that, although sildenafil produced a statistically significant fall in regurgitation versus placebo, there was no improvement in oesophageal clearance or quality-of-life scores, and the authors concluded that clinically relevant improvements were not seen (Mehain et al., 2022). The fair summary: it is reasonable for a vet to trial in selected cases, but it is not a guaranteed fix and the jury is still out.
The realistic outlook
I will not pretend the prognosis is rosy, because it is genuinely guarded, and how your pet does depends heavily on the cause and on whether aspiration pneumonia and weight loss can be kept at bay (Mace et al., 2012; McBrearty et al., 2011). Older estimates put survival at one to three months and case mortality high, with death often from aspiration pneumonia or from owners struggling with the demanding daily care (Mehain et al., 2022). Those historical figures are the worst case, though, not your pet's destiny, because the picture is not uniform. Congenital megaoesophagus can improve as the puppy matures: because the suspected mechanism is delayed nerve development, roughly 20% to 46% of congenital cases studied in German shepherds resolve spontaneously by around a year of age (Bell et al., 2022; Mace et al., 2012). So a congenital diagnosis in a young pup is not an automatic death sentence, and careful upright feeding while you wait can be life-saving. Myasthenia gravis is treatable and can remit, on average within about six months in one body of work, with roughly a third of cases achieving clinical remission in another (Mace et al., 2012; Koos, 2024). The catch is that many myasthenic dogs are lost to aspiration pneumonia in the first month, so the early weeks are the dangerous ones (Mace et al., 2012). And many dogs with idiopathic megaoesophagus live a good quality of life once their owners commit to upright feeding, an individualised consistency and vigilant watching for aspiration (Lyngby et al., 2022).
The three things that move the needle most are also the three most within your hands: feeding upright, finding the food consistency that suits this particular pet, and treating a new cough or breathing change as an emergency rather than waiting. Put your energy there while you and your vet work out the cause, and you will find this condition, daunting as it sounds tonight, is one you can do a great deal about.
References
- Bell, S. M., Evans, J. M., Evans, K. M., et al. (2022). Congenital idiopathic megaesophagus in the German shepherd dog is a sex-differentiated trait and is associated with an intronic variable number tandem repeat in Melanin-Concentrating Hormone Receptor 2 (MCHR2). PLoS Genetics, 18(3), e1010044.
- Koos, L. D. (2024). Acquired myasthenia gravis in companion animals. Today's Veterinary Practice, Nov/Dec 2024.
- Lyngby, J. G., Haines, J. M., & Guess, S. C. (2022). Use of a videofluoroscopic feeding evaluation to guide management of dogs with congenital idiopathic megaoesophagus. Veterinary Medicine and Science, 8(4), 1434–1442.
- Mace, S., Shelton, G. D., & Eddlestone, S. (2012). Megaesophagus. Compendium: Continuing Education for Veterinarians, 34(2), E1–E8.
- McBrearty, A. R., Ramsey, I. K., Courcier, E. A., Mellor, D. J., & Bell, R. (2011). Clinical factors associated with death before discharge and overall survival time in dogs with generalized megaesophagus. Journal of the American Veterinary Medical Association, 238(12), 1622–1628.
- Mehain, S. O., Haines, J. M., & Guess, S. C. (2022). A randomized crossover study of compounded liquid sildenafil for treatment of generalized megaesophagus in dogs. American Journal of Veterinary Research, 83(4), ajvr.21.02.0030.
- Quintavalla, F., Menozzi, A., Pozzoli, C., et al. (2017). Sildenafil improves clinical signs and radiographic features in dogs with congenital idiopathic megaoesophagus: a randomised controlled trial. Veterinary Record, 180(16), 404.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing digestive health. Free to join.
Join PetsLikeMine