Tooth resorption in cats: the painful problem you can't prevent
Claire Greenway
BVM&S MRCVS
The vet turned the screen towards you, pointed at a tooth that looked, to your eye, completely normal, and said a word you'd probably never heard before: resorption. Then came the part that made your stomach drop. She needs teeth out. And somewhere underneath the worry there was a quieter, harder feeling. How did I miss this? She's been eating. She's still purring on my lap every evening. What kind of owner lets this happen to their cat?
If that's roughly where you are, please take a breath, because the most important thing I can tell you comes first. You did not let anything happen. Tooth resorption is not caused by neglect, it is not caused by the wrong food, and it is not something you could have brushed away or spotted sooner at home. It's one of the most common dental problems cats get, we still don't fully know why it happens, and there is currently no way to prevent it. So let's take the guilt off the table, and I'll walk you through what this actually is, why it hurts even though she's still eating, and why taking the tooth out really is the kind thing to do.
What tooth resorption actually is
Here's the strange and slightly unfair part. This isn't decay in the way we think about a human cavity, where sugar and bacteria eat a hole in the enamel from the outside. In tooth resorption, the tooth destroys itself from the inside out.
Cells called odontoclasts, whose normal job is to remodel and break down dental tissue, become abnormally active and start dissolving the mineralised structure of the tooth (FelineVMA, 2025). It usually begins on the root, hidden below the gumline, and works its way up. The body is quite literally resorbing the tooth, dismantling it and replacing it with scar-like tissue or bone. That's why the word is resorption rather than decay, and it's why there's nothing to "fill". There's no cavity to plug, because the tooth material itself is disappearing.
Any tooth can be affected, but the small cheek teeth on the lower jaw, the mandibular premolars, are the ones we see it in most often (FelineVMA, 2025). Frequently it turns up in more than one tooth, and cats who've had it in one tooth often go on to develop it in others, which is why we keep an eye on the whole mouth rather than just the one that got treated.
How common is this, actually?
Common enough that most cat owners will meet it eventually, and most have simply never heard the name. Reported prevalence in cats ranges from around 28.5% to 67%, depending on how the cats were examined and their average age (FelineVMA, 2025). The figure climbs steadily as cats get older. Cornell's feline health specialists put it at close to three-quarters of cats aged five and over (Cornell Feline Health Center), and in older cats the numbers are higher still.
So if you're sitting there feeling like the only person whose cat has developed some rare, terrible problem, you're not. This is one of the bread-and-butter conditions of feline dentistry. It's just one that lives below the gumline and behind that famously stoic cat face, which is exactly why so few owners have heard of it until the day a vet points at the screen.
Why it isn't your fault, and why you couldn't have prevented it
I want to spend a moment here, because this is the bit that keeps owners up at night.
Despite decades of study, the cause of tooth resorption is still unknown (FelineVMA, 2025). There have been theories over the years, including ideas about dietary vitamin D, about diet texture, and about chronic inflammation, but none of them has held up as the answer. The honest position from the profession is that we don't yet know what triggers it.
And this is the line I most want you to hold on to. No means of preventing tooth resorption has been found, and there is no way to stop the progression of a lesion once it has started (FelineVMA, 2025). That is not a gap in your care. It's a gap in veterinary science. Brushing her teeth every night, feeding a "dental" diet, booking annual check-ups, none of it would have stopped this particular process, because we don't have anything that stops this particular process. Owners of cats who brush religiously get this diagnosis too.
I don't say any of that to talk you out of home dental care. Brushing and regular check-ups genuinely matter, because they protect against periodontal (gum) disease, which is preventable, and because a cat who's used to having her mouth looked at is a cat whose resorption gets caught earlier. But catching it early and preventing it are two different things. You can do everything right and still end up in this room. That is not failure. That is bad luck meeting an ordinary cat.
Why she's still eating when it hurts this much
This is usually the hardest thing for owners to square. If it's so painful, why is she still clearing her bowl?
Because she's a cat. Cats are hard-wired to hide pain, an instinct inherited from ancestors for whom showing weakness meant becoming prey. A cat in real oral pain will very often keep eating anyway, because the drive to eat is stronger than the urge to stop. Which means "she's still eating" tells you almost nothing about whether her mouth hurts. It's one of the most misleading reassurances there is, and if it fooled you, it's fooled thousands of us, vets included. (There's more on this in our piece on why cats hide oral pain.)
Tooth resorption is described in the feline dental guidelines as a common, progressive and often painful condition (FelineVMA, 2025). When the resorption reaches the sensitive inner layers of the tooth, it can be genuinely, sharply sore. Cornell's specialists describe cats showing what looks like excruciating pain when they bite down on an affected tooth (Cornell Feline Health Center).
The tells, when they show at all, are quiet. The classic ones are:
- Jaw chattering or trembling, especially when eating or when the sore spot is touched
- Dropping food from the mouth, or tilting the head to chew on one side
- Swallowing food whole, or suddenly preferring soft food and turning down biscuits she used to love
- Drooling, sometimes with a fleck of blood
- Pawing or rubbing at the face, and becoming head-shy or grumpy when you go near her cheek
- A small red spot at the gumline where the tooth meets the gum, which is often the only visible clue
None of these is dramatic, and any one on its own is easy to explain away as "she's getting older" or "she's just fussy". That's exactly the trap. If you've noticed even one or two of these, you weren't being careless. You were reading a cat who's very good at keeping secrets.

Why an x-ray is the only way to see it properly
Here's why this so often comes as a shock. The part of the tooth you can see, the crown, can look completely normal while the tooth is being destroyed at the root below the gum. You cannot judge this by looking, and neither can we, not reliably.
That's why a proper assessment needs dental x-rays. Full-mouth intraoral radiography is considered essential for feline dentistry, both to find early lesions that only affect the root and to work out exactly what type of resorption a tooth has (FelineVMA, 2025). The World Small Animal Veterinary Association makes the same point for every dental: without x-rays and probing under anaesthetic, you are guessing at what's below the gumline (WSAVA, 2020). A great many resorptive lesions are simply invisible to the naked eye and only show up on the film.
This is also why a cheaper "scale and polish" that skips the x-rays can miss resorption entirely, and why the anaesthetic that owners often fear is actually what makes a thorough, honest assessment possible. We go into this in more detail in why a "clean" without dental x-rays misses disease. The short version: the x-ray isn't an upsell. For resorption, it's the whole diagnosis.
Type 1 and type 2: why the plan is different
When your vet talks about the "type" of resorption, they're describing what the x-ray shows about the root, and it genuinely changes the treatment. This distinction is at the heart of the updated 2025 feline dental guidelines (FelineVMA, 2025), so it's worth understanding.
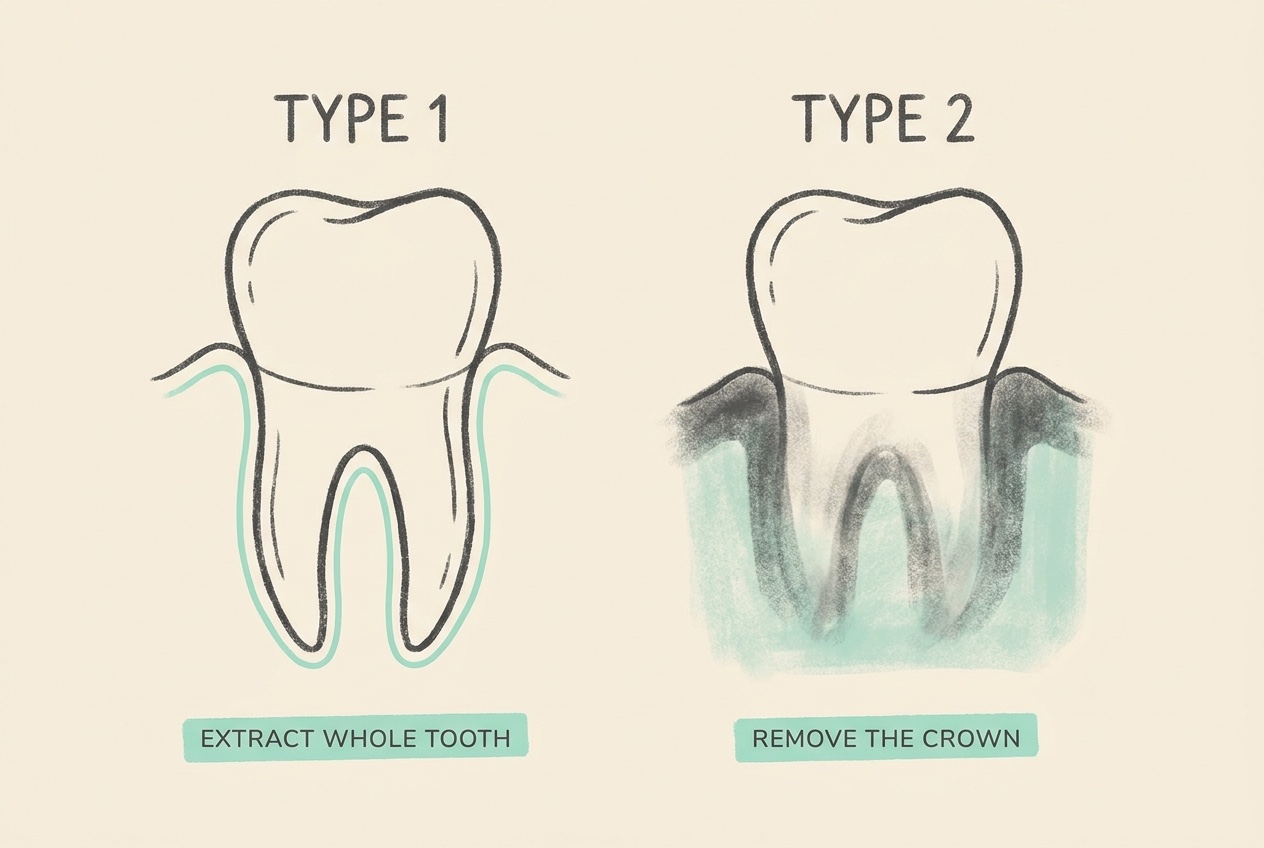
Type 1. On the x-ray, the root still looks like a root. It has a normal density and you can still see the thin dark line of the periodontal ligament, the space between root and jawbone. The crown may be crumbling, but the root is essentially intact. When that's the case, the whole tooth, crown and roots, needs to come out (FelineVMA, 2025). The root is still a solid, potentially sore structure with a normal attachment, so leaving any of it behind would leave a problem behind.
Type 2 (replacement resorption). Here the root is dissolving and being replaced by bone. On the x-ray it looks faded and blurry, blending into the surrounding jaw, and that thin ligament line has disappeared. The root, in effect, is turning into bone. In these cases the ideal is to remove only the crown, a procedure called crown amputation or coronectomy, and let the gum heal over the remnant (FelineVMA, 2025). Trying to dig out a root that's already merging with the jaw would mean cutting away healthy bone for no benefit.
Some teeth show a mix of both, which is called type 3.
Now, one really important safeguard, because crown amputation can be misused. Removing the crown and leaving the root behind is only appropriate for type 2 replacement resorption confirmed on x-ray, and only when there's no periodontal disease, no endodontic (root canal) infection, and no chronic gingivostomatitis in that mouth (Clinician's Brief; FelineVMA, 2025). If x-rays aren't available, or any of those other problems are present, the correct treatment is full extraction of the tooth, not a shortcut. Crown amputation is a considered clinical decision made from the film, never a quicker, cheaper way to avoid a full extraction. If your vet has recommended it, it's because your cat's x-rays fit that specific picture.
Why taking the tooth out is the kind thing, not a failure
I know that "she needs teeth out" can sound like something has gone badly wrong, or like a drastic last resort. It isn't. With resorption it's the treatment, and here's the logic.
The tooth is being destroyed and there is no way to reverse that, no way to stop it, and nothing to fill (FelineVMA, 2025). We can't save a tooth that's dismantling itself. As long as it's still there, it's a source of pain, and every time she bites down on it she feels it. Simply monitoring a painful resorbing tooth and hoping it settles isn't kindness, it just prolongs the ache. Removing the tooth, or the crown in the case of type 2, removes the pain at its source. That's the point of the whole procedure.
So the extraction isn't the sad part of this story. It's the good part. It's the thing that finally lets her stop hurting.
Life after her teeth come out
This is the reassurance owners most need and least expect, so let me be plain about it. Cats do remarkably well after dental extractions, even a lot of extractions. They eat well, they're comfortable, and they very often seem brighter and more themselves within a week or two, because a source of chronic pain has finally gone.
Cats don't chew their food the way we imagine anyway. They tend to bite, crush and swallow, and a cat with missing teeth manages this perfectly happily. Most eat normal food, including dry food, once the gums have healed. In the first week or so after surgery she'll usually be on soft food and pain relief while everything settles, and we'll talk you through exactly that at discharge. There's more on the recovery itself in eating after extractions, and on what an extraction day actually involves in the extraction phone call.
Because resorption tends to affect more than one tooth over time, we'll usually recommend keeping an eye on the rest of the mouth, with a check-up and often repeat x-rays down the line to catch any new lesions early. That's not because anything went wrong, it's just how this condition behaves. And if your cat has widespread painful inflammation on top of the resorption, it's worth reading about feline chronic gingivostomatitis, a related condition that's managed along similar, extraction-led lines.
One practical note before you go. If your cat stops eating altogether, becomes withdrawn, or you see persistent bleeding from the mouth, don't wait for the next routine appointment, ring your vet. A cat who goes off food entirely needs to be seen promptly whatever the underlying cause.
For now, the thing to carry out of that consult room isn't guilt. It's this: you spotted something, you took her in, and you're about to fix the one thing that was quietly hurting her. Book the treatment, ask every question you've got, and let yourself off the hook. This was never yours to prevent.
References
- Feline Veterinary Medical Association (FelineVMA). 2025 FelineVMA feline oral health and dental care guidelines. Journal of Feline Medicine and Surgery, 2025.
- Cornell Feline Health Center. Tooth Resorption. Cornell University College of Veterinary Medicine.
- World Small Animal Veterinary Association (WSAVA). Global Dental Guidelines. WSAVA, 2020.
- Crown amputation for feline tooth resorption. Clinician's Brief. [author/date to confirm at integration]
- American Veterinary Dental College (AVDC). Tooth Resorption classification (Types 1–3). AVDC Nomenclature.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing teeth & mouth. Free to join.
Join PetsLikeMine