
Finding real help: vet, behaviourist or trainer, and how to tell them apart
Dr. Alastair Greenway
MRCVS
In the UK, "dog trainer" and "behaviourist" are not protected titles. That surprises almost every owner I tell it to. Unlike "vet" or "doctor", anyone at all can print "behaviourist" on a business card tomorrow, charge you for advice, and lay hands on your frightened or aggressive animal, with no training, no assessment, and no accountability (ABTC). It isn't a reason to despair, because a clear, credible structure sits on top of this unregulated market and lets you find genuinely qualified help. But the responsibility to check falls on you.
The right first move for a real behaviour problem is not a trainer at all, it's your vet. Pain and illness are such common, hidden drivers of behaviour change that ruling them out is the genuine first step, which our guide on whether it is behaviour or medical covers in full, and the very best behaviourists insist on it, working only once your vet has been involved.
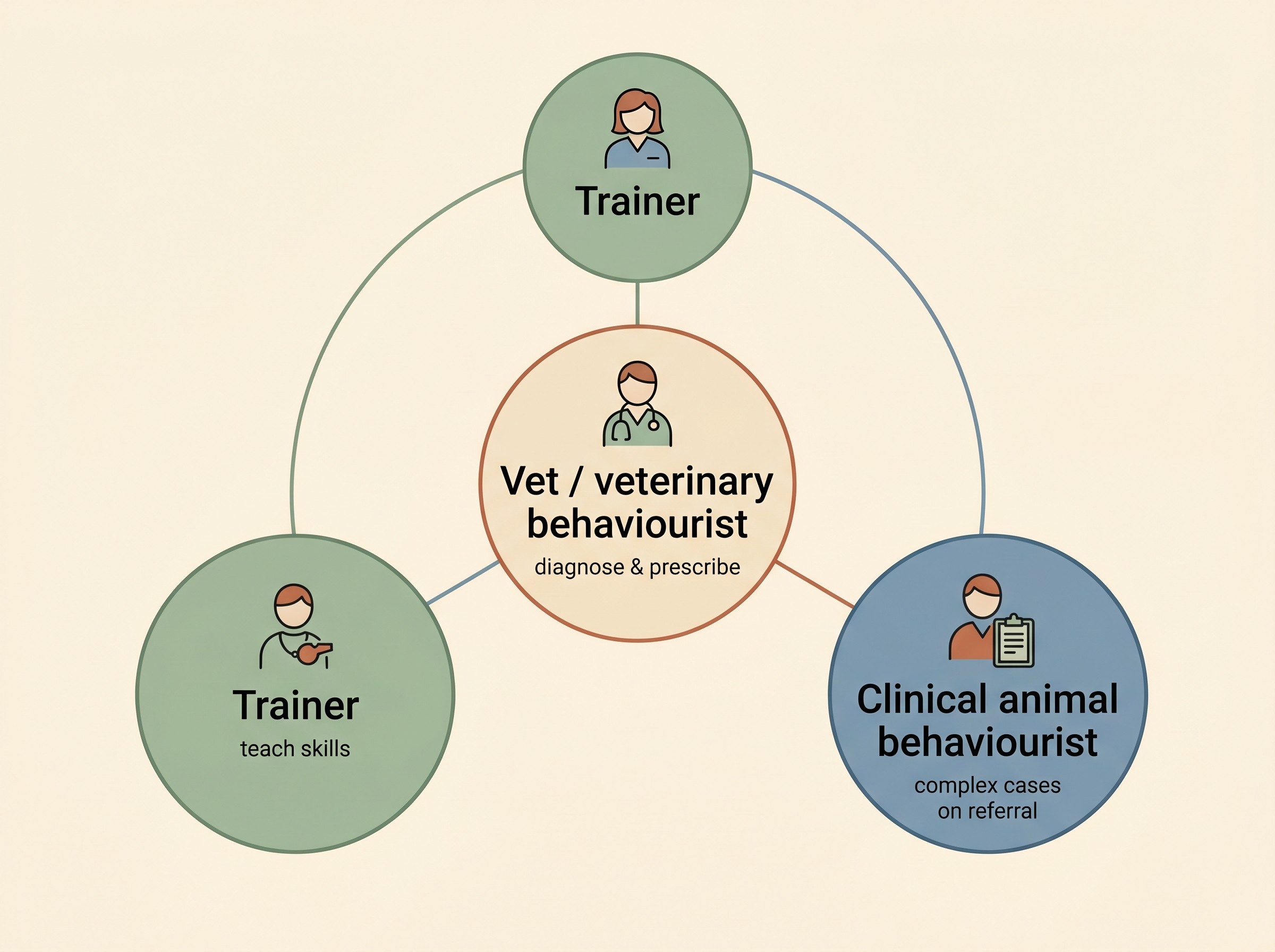
Vet, behaviourist, trainer: who does what
These three roles overlap in people's minds and get used interchangeably, which is how owners end up with the wrong help. They are genuinely different jobs. A trainer, or more precisely an animal training instructor, teaches skills: recall, lead walking, settling, a solid "leave it", building a nervous dog's everyday confidence. A good reward-based trainer is the right first call for ordinary training and prevention (ABTC). What a trainer is not is the right person for a clinical problem like aggression, panic at being left, or a phobia: those are not training gaps but emotional and sometimes medical problems that need a different level of expertise.
A clinical animal behaviourist is that next level: the role for serious, distressing problem behaviour such as aggression, separation-related problems, severe fears and phobias, and compulsive disorders. Importantly, a properly qualified one works on veterinary referral, so your vet is involved first and any underlying illness, injury or pain is screened and treated alongside the behaviour (ABTC; APBC, 2024). That requirement is not bureaucracy; it stops a sore, sick animal being treated as a behaviour case when it needed a diagnosis.
A veterinary behaviourist is a vet who has gone on to specialise in behaviour, which matters for one reason above all: only a vet can diagnose medical disease and prescribe medication. The Royal College of Veterinary Surgeons recognises two tiers, the Advanced Practitioner in Companion Animal Behaviour and, above it, the Specialist in Behavioural Medicine, and there are remarkably few of either; at the time of writing the RCVS Find a Vet register listed just 11 Specialists in Behavioural Medicine and 7 Advanced Practitioners in the whole country (RCVS Find a Vet, 2026 retrieval). They handle the most complex cases, where medication and behaviour modification often need weaving together by one clinician.
This is genuinely a team model, and the law explains why: managing a behaviour problem does not legally count as an act of veterinary surgery unless it involves diagnosis or prescription-only medicines (BSAVA), which is what lets a qualified non-vet behaviourist take a case on referral while the diagnosis and any medication stay firmly the vet's job.
Accreditation that actually means something
If titles are not protected, what do you look for instead? The single most useful answer in the UK is the Animal Behaviour and Training Council, the ABTC: the umbrella body setting standards and holding a national register of practitioners independently assessed against them. The register spans a ladder of roles, from Animal Trainer and Animal Training Instructor through Animal Behaviour Technician and Clinical Animal Behaviourist up to Accredited Animal Behaviourist and Veterinary Behaviourist, so the title someone holds tells you what they have been assessed to do (ABTC).
What makes ABTC registration meaningful, beyond the assessment, is the methods condition attached to it. Registered practitioners must use science-led, compassionate and non-punitive methods and equipment, and the council's standards require that training and behaviour programmes are not based on positive punishment or on creating fear or anxiety in the animal (ABTC). The accreditation does not only confirm someone has been checked; it tells you the approach they are committed to.
Several other memberships map onto these same standards, so you do not need to memorise the alphabet soup. Full membership of the Association of Pet Behaviour Counsellors (the APBC) is assessed against the ABTC's clinical criteria, and every member works on veterinary referral and completes at least thirty hours of professional development a year (APBC, 2024). The CCAB (Certificated Clinical Animal Behaviourist) scheme, run by the independent CCAB Certification, is another rigorous route that combines a relevant degree with a separate clinical-skills assessment (ASAB; CCAB Certification). The owner-facing shortcut is simple: look for ABTC registration plus one of these memberships, and check the person works on veterinary referral. The RSPCA's own guidance points owners down exactly this path, the vet first and then an ABTC-registered behaviourist (RSPCA).
When you genuinely need to refer up
Most everyday wobbles do not need a clinical referral: a dog that pulls, a puppy still learning the house rules, a cat that needs more enrichment. A good trainer and a sensible plan usually suffice. The signal that you have crossed into clinical territory is the emotion and the stakes, not the species or the surface behaviour. If the problem involves real fear, panic or aggression, if your animal is suffering rather than simply untrained, or if anyone's safety is at risk, that is a clinical problem and it deserves a vet and very probably a referral. Aggression is the clearest example, and where the team model earns its keep: the medical rule-out, behaviour modification, and sometimes prescribed medication often all belong in the plan together, which only this level of help can deliver safely. Where medication is needed it is a vet's decision and never something to source or dose yourself, and the route to it always runs through your vet, with the detail in our medication guides.
One situation overrides all of this. If a dog has actually bitten, or you are in an acute moment where someone could be hurt, do not start ringing round for a behaviour appointment first. Make everyone safe, then use our guides on behaviour emergencies and safety and, after a bite specifically, on the safety, law and qualified-help pathway, which cover the high-stakes steps this article deliberately does not.
This is just as true for cats, worth saying because so much behaviour advice is written as though only dogs have problems. Behaviourists take feline cases such as house soiling, inter-cat conflict and overgrooming on the very same vet-referral model, and if anything the medical rule-out matters even more in cats, where so many "behaviour" signs turn out to be pain or illness.
Red flags: advice that can make things worse
In an unregulated market you will inevitably meet advice that is not just unhelpful but actively harmful, and a handful of red flags protect you from most of it. The biggest is the use of pain or fear. Best-practice bodies are unambiguous: only reward-based methods should be used for all training and behaviour work, there is no evidence aversive methods are more effective, and good evidence they harm welfare and the relationship between you and your animal (AVSAB, 2021). So treat prong (pinch) collars, choke or slip chains, electronic shock collars, and physical force as a clear signal to walk away; a UK trial even found e-collars no more effective than reward-based training for recall, while showing more signs of stress (China, Mills & Cooper, 2020). The deeper evidence on why punishment backfires is in our guide on how pets actually learn; here, aversive tools are simply your cue to keep looking.
The law on shock collars is also worth knowing, and worth dating because it is in flux. They have been banned in Wales since 2010 (Animal Welfare (Electronic Collars) (Wales) Regulations 2010); in England a ban was drafted for 1 February 2024 but was never made into law and, as of the 2026 check, remains unenacted, though the government has since included a shock-collar ban in its animal welfare plans and is consulting on it (Defra, 2023; 2026). Scotland discourages their use through guidance rather than a statutory ban, an approach its own animal welfare commission has recommended hardening into a prohibition (gov.scot, 2023). Whatever the law in your nation, a kind professional would not use one anyway.
Be wary, too, of anyone who frames everything around "dominance", being the "pack leader" or the "alpha", a model formally rejected on the evidence that force-and-rank-based methods are less effective and risk dangerous fallout behaviour (AVSAB, 2008). Be wary of "guaranteed" results, because no good professional promises outcomes for a living animal. And be wary of "flooding", forcing a frightened animal to face the full-strength version of what scares it until it supposedly gets over it: a recognised way to make fear worse, quite distinct from proper desensitisation, which builds up gently. If you are unsure whether you are facing a training issue or something clinical, our behaviour check tool can help you triage it before you spend a penny.
What a referral involves, and what it costs
A behaviour referral is not free and usually not a quick fix, so be a little suspicious of anyone who implies otherwise. A full clinical behaviour consultation in the UK commonly costs several hundred pounds, often a long session of two or more hours followed by a written plan and follow-up support; the figure varies widely by region and seniority (RSPCA). What you get for it is a proper assessment of a problem that has been distressing your whole household, from someone genuinely qualified working with your vet.
Two things soften the cost. Many pet insurance policies cover behaviour fees, but usually only when the behaviourist holds recognised accreditation such as ABTC or APBC and the case has been referred by your vet, one more reason to take the accredited, vet-referred route; check your policy wording, and the excess, before you book (RSPCA). And reduced-cost and charity options exist, for example the free Behaviour Support Line run by Dogs Trust, a good place to start if cost is a real barrier (Dogs Trust).
Before you commit to anyone, two questions cut through almost everything. Borrowing the spirit of the "least intrusive, minimally aversive" principle the profession holds itself to, ask: what will happen to my animal when it gets the behaviour right, what will happen when it gets it wrong, and are there gentler alternatives to anything you are proposing? A good professional answers clearly and is glad you asked; vagueness, defensiveness, or talk of corrections and dominance is your answer, and it is to keep looking. Pair those two questions with a check of the register, and you have what you need to find help that makes your animal's life better, not worse.
References
- Animal Behaviour and Training Council. The ABTC Register of practitioners and standards of practice. ABTC, 2024.
- Association of Pet Behaviour Counsellors. About the APBC: full membership, veterinary referral and continuing professional development requirements. APBC, 2024.
- Royal College of Veterinary Surgeons. Find a Vet: register of Advanced Practitioners and Specialists in Companion Animal Behaviour / Behavioural Medicine. RCVS, 2026 (retrieved 2026).
- British Small Animal Veterinary Association. Behaviour and the law: when behaviour work constitutes an act of veterinary surgery. BSAVA.
- Association for the Study of Animal Behaviour. CCAB accreditation: the Certificated Clinical Animal Behaviourist scheme. ASAB.
- CCAB Certification Ltd. Who are CCAB Certification: academic and clinical-skills standards for the Certificated Clinical Animal Behaviourist (CCAB). CCAB Certification.
- RSPCA. Help with dog behaviour care costs: using a vet and an ABTC-registered behaviourist. RSPCA.
- American Veterinary Society of Animal Behavior. AVSAB Position Statement on Humane Dog Training. AVSAB, 2021.
- China L, Mills DS, Cooper JJ. Efficacy of Dog Training With and Without Remote Electronic Collars vs. a Focus on Positive Reinforcement. Frontiers in Veterinary Science, 2020;7:508.
- The Animal Welfare (Electronic Collars) (Wales) Regulations 2010 (W.S.I. 2010 No. 943 (W.97)). legislation.gov.uk, 2010.
- Department for Environment, Food and Rural Affairs. The Animal Welfare (Electronic Collars) (England) Regulations 2023 (laid before Parliament; ban not enacted). Defra / legislation.gov.uk, 2023 (status as of 2026).
- Scottish Animal Welfare Commission. Dog training: use of handheld remote-controlled training devices (e-collars) - report. Scottish Government (gov.scot), 2023.
- American Veterinary Society of Animal Behavior. AVSAB Position Statement on the Use of Dominance Theory in Behavior Modification of Animals. AVSAB, 2008.
- Dogs Trust. Behaviour Support Line: free specialist behaviour advice. Dogs Trust.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing behaviour & anxiety. Free to join.
Join PetsLikeMine