
Why Epilepsy Is a "Diagnosis of Exclusion"
Dr. Alastair Greenway
MRCVS
Your dog has had a seizure, maybe more than one. You've been to the vet, perhaps had blood taken, perhaps been quoted for an MRI. Then the verdict comes back: "the tests are all normal, it's most likely epilepsy." And the obvious question lands: how can anyone know what's wrong if nothing showed up? It's exactly the right question to ask, and the answer is more reassuring than it sounds.
The most common form of canine epilepsy, idiopathic epilepsy, is what's called a diagnosis of exclusion. It's reached not by one positive test but by carefully ruling out the other things that cause seizures, until what's left, in the right dog, is epilepsy itself. So those normal results aren't a dead end. In the right context, they are the answer. This article is about that reasoning: why ruling things out is the diagnosis, how vets grade their confidence in it, and why a clean set of results should reassure rather than unsettle you. The three categories of cause are covered in reactive, structural and idiopathic seizures explained; the tests and what they cost live in the diagnostic workup; and the breed and genetics side belongs to idiopathic epilepsy: breeds, genetics and age of onset.
What "diagnosis of exclusion" actually means
Some conditions announce themselves. A broken leg shows on an X-ray; an infection grows on a culture. Idiopathic epilepsy isn't like that. There's no blood test and no scan that says "this dog has idiopathic epilepsy" in so many words. Instead, the diagnosis is built.
The international veterinary epilepsy task force, the specialists whose consensus guidelines most vets work from, put it plainly: the diagnosis of idiopathic epilepsy "is one of exclusion and is made based on the age at epileptic seizure onset, unremarkable inter-ictal physical and neurological examinations, and exclusion of metabolic, toxic and structural cerebral disorders" (De Risio et al., 2015). Unpick that sentence and you have the whole method: the right age, a normal dog between seizures, and the absence of the other things that could explain it. Clean results aren't a failure to find a cause. They're the alternatives being cleared one suspect at a time, and the conclusion is no weaker for it.
The approach rests on two questions, in order: first, were these events genuinely epileptic seizures at all, rather than fainting or a movement disorder that can look alarmingly similar; and second, once you're satisfied they were, what's the cause (De Risio et al., 2015)?
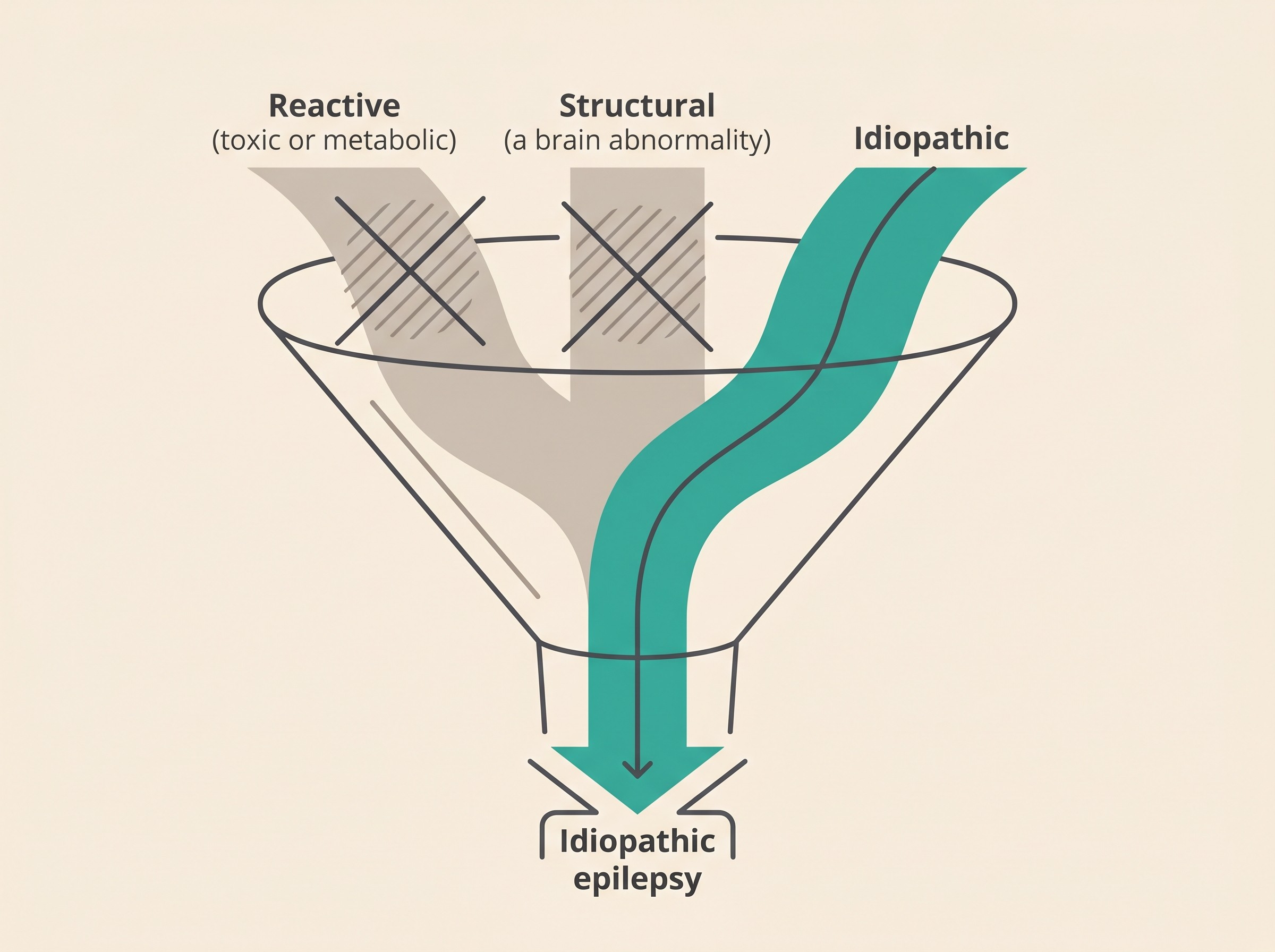
Broadly, there are three reasons a pet seizes: a reactive seizure (a normal brain reacting to a transient toxic or metabolic upset, which isn't epilepsy at all), structural epilepsy (an identifiable brain abnormality), and idiopathic epilepsy, which is what remains once the first two are excluded (Berendt et al., 2015). Those categories are the whole subject of the next article. What matters here is simply that idiopathic epilepsy sits at the bottom of that funnel: it is the conclusion you reach when the streams above it have been ruled out.
The pattern that fits: age, history and a normal exam
A vet's confidence here isn't blind faith in normal results. It's that idiopathic epilepsy has a recognisable shape, and clean results in a dog who fits that shape mean something specific. The single most useful clue is age: the classic window for idiopathic epilepsy to first appear is between six months and six years (Berendt et al., 2015; De Risio et al., 2015). A young adult who starts seizing inside that window, and is completely normal in between, is the textbook idiopathic picture. Seizures that begin well outside it, in a very young puppy or for the first time in an older dog, are more likely to have a reactive or structural cause, and raise suspicion accordingly (De Risio et al., 2015).
The other half of the pattern is what your vet finds between seizures, in the time vets call inter-ictal. A dog with idiopathic epilepsy is, by definition, neurologically normal when not actively seizing, so a normal physical and neurological examination between episodes fits the diagnosis (De Risio et al., 2015). Persistent abnormalities, a wobble that never quite goes, a head tilt, a lingering change in behaviour or vision, point instead towards something structural. So the diagnosis isn't "we found nothing, so it must be epilepsy". It's "this dog is the right age, is normal between seizures, and the tests for other causes are clear", three things lining up rather than one thing missing.
The three tiers of diagnostic confidence
A diagnosis of exclusion isn't all or nothing, trustworthy only once every conceivable test has been run. The task force set out three tiers of diagnostic confidence, so a vet, and you, can know how solid the diagnosis is at any stage (De Risio et al., 2015). Knowing which tier you're at takes much of the anxiety out of "but are we sure?"
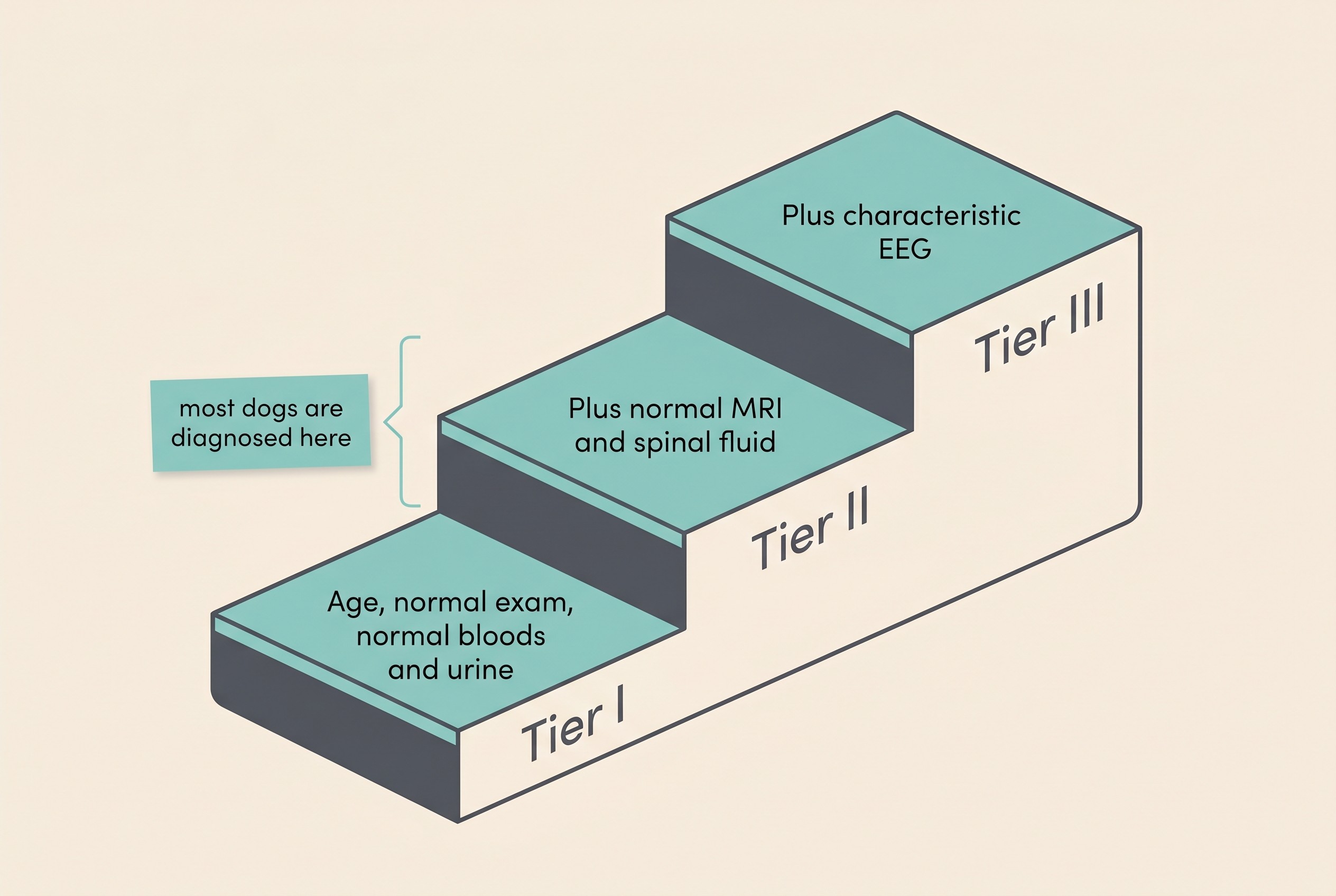
Tier I is the confidence a vet can reach in general practice, without advanced imaging. It needs a history of two or more unprovoked seizures at least 24 hours apart; an age at onset between six months and six years; an unremarkable physical and neurological examination between seizures; and a clear "minimum database" of first-line tests, a complete blood count, serum biochemistry and a urinalysis, all unremarkable, along with bile acids and/or ammonia to check liver function (De Risio et al., 2015). It's the pattern described above, confirmed with routine blood and urine tests, and for a great many dogs it's where the diagnosis reasonably sits.
Tier II is higher confidence. It adds three things to Tier I: unremarkable fasting and post-prandial bile acids (a fuller liver check), an unremarkable brain MRI using an epilepsy-specific protocol, and unremarkable analysis of the cerebrospinal fluid, the fluid around the brain and spinal cord (De Risio et al., 2015). This is the level you reach when imaging and a fluid sample have actively looked inside the head and found nothing structural or inflammatory.
Tier III is the highest level, used mainly in research and referral. It's everything in Tiers I and II plus an EEG, an electroencephalogram, recording the characteristic electrical abnormalities of a seizure disorder (De Risio et al., 2015). EEG is rarely available in routine practice, so most pets are confidently diagnosed at Tier I or II and never need it. See it as the academic gold standard, not a box your dog has failed to tick.
A Tier I diagnosis isn't second-rate, and that's worth saying plainly. The tiers exist precisely so a vet can hold a confident, well-grounded diagnosis in a dog who fits the pattern, without every owner being told they must spend thousands on an MRI before anyone will name what's wrong. What pushes towards Tier II, towards MRI and a spinal fluid sample, is anything that doesn't fit: an atypical age of onset, an abnormal neurological examination between seizures, or seizures that don't respond as expected to treatment (De Risio et al., 2015). Any of those raises the realistic possibility of a structural cause, worth ruling in or out properly. The practicalities, and the frank conversation about anaesthetising a dog for an MRI, belong to the diagnostic workup article.
Why "normal results" are the point, not a problem
When your vet says the bloods are normal and the MRI is clear, it's natural to hear "we still don't know what's wrong." For a diagnosis of exclusion, that's the wrong way round. Those tests aren't searching for a positive marker of epilepsy. They're searching for the other causes, the metabolic, toxic and structural ones, that would mean it isn't idiopathic epilepsy (De Risio et al., 2015). When they come back clear, in a dog of the right age and normal between seizures, they confirm the diagnosis rather than undermining it (De Risio et al., 2015).
There's quiet good news folded into this, too. A normal MRI means no brain tumour, no encephalitis, no malformation; normal bloods mean no liver shunt and no metabolic crisis driving the seizures. Those are reassuring findings in their own right. And for scale: idiopathic epilepsy is the most common chronic neurological disorder seen in dogs (De Risio et al., 2015), affecting roughly 0.6 to 0.75% of the general dog population. Your dog is far from alone, and this is a condition the profession knows well.
What this means for treatment
The most practical consequence surprises people, in a good way: you do not have to reach Tier III, or even Tier II, before treatment can begin. A confident Tier I diagnosis is enough to start the conversation, when the seizure pattern warrants it. The task force's criteria for when to begin medication include two or more seizures within six months, any episode of cluster seizures or status epilepticus, post-ictal signs that are especially severe or last more than 24 hours, or seizures clearly increasing in frequency or severity over time (Bhatti et al., 2015). None of those requires an MRI first.
The decision itself belongs to when treatment should start, and the realistic framing of what success looks like, control rather than cure, to realistic goals. For now, two things are worth carrying forward. The goal is reduction, not a complete end to seizures: a "responder" usually means at least a halving of seizure frequency, and complete freedom, while wonderful when it happens, is uncommon (Bhatti et al., 2015). And once an anti-seizure medication is started, it's never stopped abruptly, because sudden withdrawal can itself trigger clustered or prolonged seizures.
Whichever path you take, the single most useful thing you can do from today is keep a clear record of every seizure: date, time, duration, what it looked like and how your dog recovered. That record is the evidence base for the whole decision, the way you and your vet will see whether the pattern crosses the threshold to treat and, later, whether treatment is working. Our seizure diary is built for exactly this, turning scattered, frightening moments into the clear picture your vet needs. Knowing the emergency line matters here too: a seizure lasting more than five minutes, two or more in twenty-four hours, or fits running into one another without recovery means a vet or emergency clinic now. A single short seizure with a normal recovery is frightening, but it is not, by itself, an emergency.
A brief word on cats
The same exclusion logic applies to cats: idiopathic epilepsy is still diagnosed by ruling out reactive and structural causes. The balance differs, though. In cats, structural causes and reactive ones, particularly toxic and metabolic upsets, are relatively more common than in dogs, which raises the index of suspicion and means investigation is often pursued sooner.
"The tests were normal" is not the brush-off it can feel like at the worst moment. For a diagnosis of exclusion, normal results in the right dog are the diagnosis doing exactly what it should. The next sensible step is to understand the three categories those tests were sorting between, and reactive, structural and idiopathic seizures explained is where that picture, in dogs and cats alike, comes properly into focus.
References
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Löscher, W., Mandigers, P. J. J., Matiasek, K., Pakozdy, A., Patterson, E. E., Platt, S., Podell, M., Potschka, H., Rusbridge, C., & Volk, H. A. (2015). International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- Berendt, M., Farquhar, R. G., Mandigers, P. J. J., Pakozdy, A., Bhatti, S. F. M., De Risio, L., Fischer, A., Long, S., Matiasek, K., Muñana, K., Patterson, E. E., Penderis, J., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Tipold, A., & Volk, H. A. (2015). International veterinary epilepsy task force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research, 11, 182.
- Bhatti, S. F. M., De Risio, L., Muñana, K., Penderis, J., Stein, V. M., Tipold, A., Berendt, M., Farquhar, R. G., Fischer, A., Long, S., Mandigers, P. J. J., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11, 176.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine