Reactive, Structural and Idiopathic Seizures Explained
Dr. Alastair Greenway
MRCVS
A seizure sends most owners home with one word ringing in their head: why. Why my pet, why now, and is this something that can be fixed or something we have to live with?
The honest starting point is that "seizure" is a symptom, not a diagnosis, much as a cough is a symptom rather than a disease. A burst of abnormal electrical activity in the brain can come from very different causes, and the cause decides everything that follows: which tests make sense, what the treatment looks like, and what the outlook is. None of this is guesswork for your vet. There's a clear, internationally agreed framework that sorts the causes into three buckets, and once you understand them the picture starts to make sense.
That framework comes from the International Veterinary Epilepsy Task Force, a group of veterinary neurologists who in 2015 published a consensus on how seizures should be classified (Berendt et al., 2015). It's the backbone of how your vet is thinking. Below I'll explain what each category means and how your pet's age and breed shift the odds between them. What I won't do is walk you through the tests themselves, or explain why "all the results were normal" can still be an answer. Those have homes of their own, and I'll point you to them as we go.
The three categories
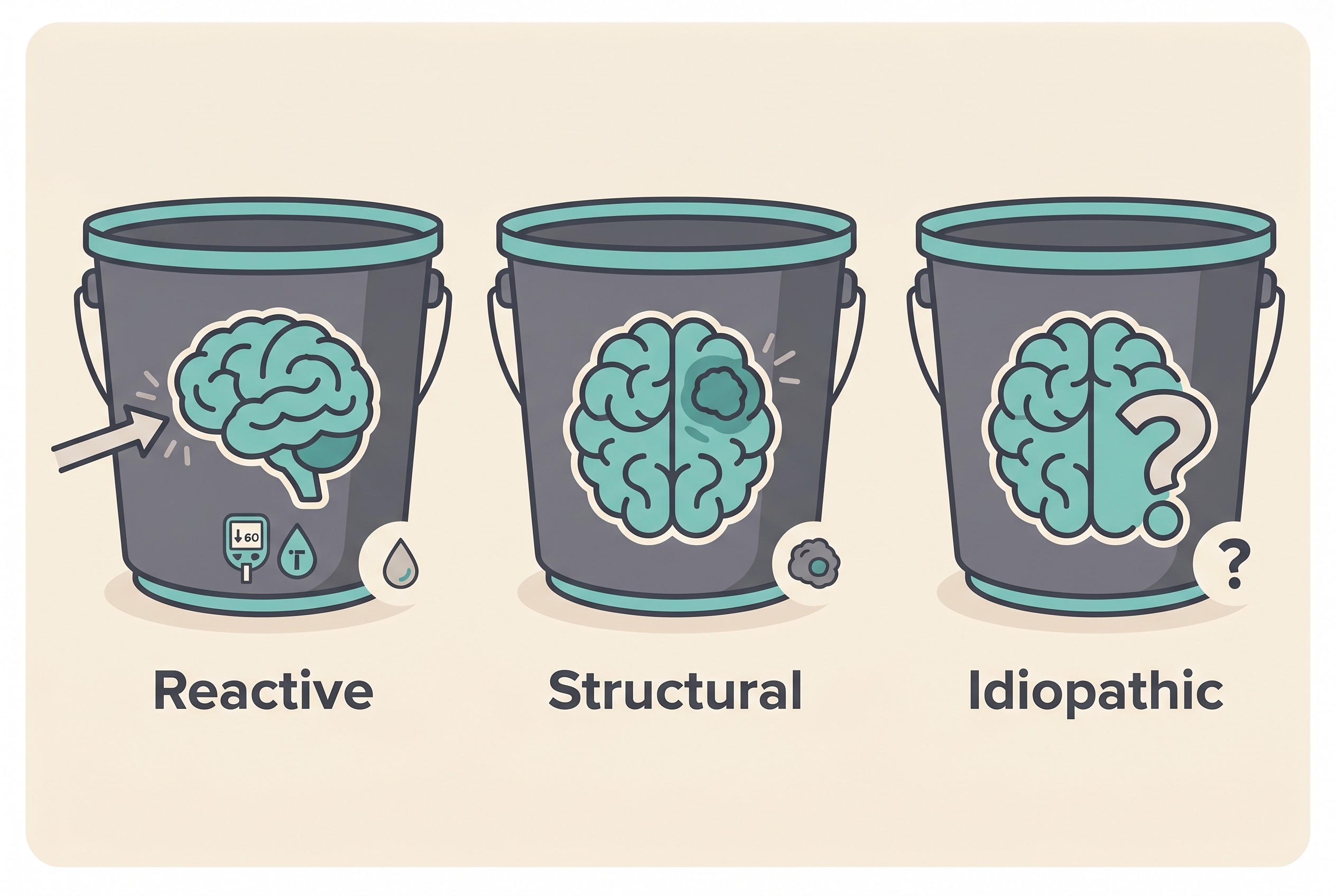
Reactive seizures: a normal brain reacting to a problem elsewhere
Start here, because this is the most hopeful category and the single most useful idea for a frightened owner. A reactive seizure is, in the Task Force's own words, "a natural response from the normal brain to a transient disturbance in function (metabolic or toxic in nature) which is reversible when the cause or disturbance is rectified" (Berendt et al., 2015).
The word that matters is reversible. In a reactive seizure the brain itself is healthy. It's seizing because something elsewhere in the body has temporarily upset it. This is not epilepsy. Fix the underlying problem and the seizures stop, with no lifelong brain disorder to manage.
The usual culprits are metabolic or toxic. On the metabolic side, dangerously low blood sugar (hypoglycaemia), a liver that isn't clearing toxins properly (hepatic encephalopathy, which a portosystemic liver shunt can cause), kidney failure letting waste build up in the blood (uraemia), and disturbances in the body's salts and electrolytes can all tip a normal brain into a seizure (Berendt et al., 2015). On the toxic side, a wide range of poisons can do it, and in cats one toxin stands so far above the rest that it gets its own section below.
So if your vet suspects a reactive cause, they'll be looking outside the brain: blood tests, blood sugar, bile acids, electrolytes, and a careful history of anything your pet might have eaten. The aim is to find and fix the cause, not to commit your pet to anti-seizure drugs for life.
Structural epilepsy: a physical abnormality in the brain
Structural epilepsy means recurrent seizures caused by an identifiable physical abnormality in the brain itself. Unlike a reactive seizure, there genuinely is something wrong inside the head, and you can often see it on a scan.
The causes span a fairly broad list: a tumour (neoplasia), inflammation or infection of the brain (encephalitis), a vascular event such as a stroke, head trauma, a developmental malformation the pet was born with, and degenerative disease (Berendt et al., 2015; De Risio et al., 2015). What ties them together is that the seizures are a symptom of an underlying structural problem, and it's that problem, not just the seizures, that drives both the treatment and the outlook. Confirming it usually means advanced imaging, an MRI of the brain, sometimes with a sample of the fluid around it. When that's warranted, and what it costs, belong to the diagnostic workup guide rather than here.
Idiopathic epilepsy: recurrent seizures with no cause found
Most owners have heard this third word, even if it's unfamiliar. Idiopathic epilepsy means recurrent seizures with no identifiable metabolic or structural cause. The brain looks normal, the blood tests are normal, and yet the seizures keep coming. It's presumed to be genetic, or simply of unknown cause (Berendt et al., 2015).
A piece of logic trips a lot of owners up here. Idiopathic epilepsy is a diagnosis of exclusion, meaning it's reached by ruling the other two categories out rather than by a single positive test (Berendt et al., 2015; Cornell University Riney Canine Health Center). So when your vet says the results are all normal and the diagnosis is idiopathic epilepsy, those normal results aren't a failure to find the answer. In this case, they are the answer. That idea deserves a whole piece of its own: why epilepsy is a "diagnosis of exclusion".
The Task Force splits idiopathic epilepsy into three finer subgroups depending on how strong the genetic evidence is, from a proven causative gene at one end to epilepsy of genuinely unknown cause at the other (Berendt et al., 2015). The breed and gene side of that story has its own home in breeds, genetics and age of onset. The headline here is that idiopathic epilepsy is the most common cause of recurrent seizures in dogs, and it has a very recognisable signature, which brings us to the practical core of all this.
How age and breed shift the odds
Epilepsy is one of the most common chronic neurological diseases in dogs, affecting an estimated 0.6 to 0.75% of the general dog population, or very roughly 1 in 130 dogs seen in practice (Volk, 2015). Most of those dogs have idiopathic epilepsy, and it has a classic profile worth committing to memory: onset between 6 months and 6 years of age, a median onset around 2.5 years, and a dog who is completely normal between seizures (Berendt et al., 2015; De Risio et al., 2015; Cornell University Riney Canine Health Center).
Age genuinely does shift the odds. In a study of 900 dogs that all had an MRI to investigate seizures, idiopathic epilepsy accounted for 53.8% and structural epilepsy for 45.1%, and dogs aged 6 months to 6 years were significantly more likely to have the idiopathic form (Hall et al., 2020). So a young adult dog who is normal between episodes really is the textbook idiopathic candidate. Watch the caveat, though: in that same study, over 31% of the dogs eventually diagnosed with idiopathic epilepsy were 6 years or older (Hall et al., 2020). Age tilts the probability. It never settles the question on its own. The same study found other patterns too: small breeds were over-represented for inflammatory brain disease, and large entire (un-neutered) dogs more often had tumours sitting outside the brain tissue itself (Hall et al., 2020).
Skull shape matters as well, and this is the finding I'd most want a flat-faced-breed owner to hear. In a study applying the Task Force guidelines, brachycephalic (short-nosed) dogs had structural lesions far more often than non-brachycephalic dogs, 61.8% against 22.1% (Prodger et al., 2025). Here's the part that surprises: even among dogs aged 6 months to 6 years with a normal neurological exam, 33.3% of the brachycephalic dogs still turned out to have structural epilepsy, against 0% of the non-brachycephalic ones (Prodger et al., 2025). In plain terms, a young flat-faced dog with normal bloods is a stronger candidate for an MRI than the simple rule of thumb would suggest.
How should you read all this as an owner? A young adult dog (6 months to 6 years) with a normal examination and normal blood tests is the classic idiopathic picture, and your vet may reasonably treat on that basis. Onset that is very young (under 6 months) or later in life (over 6 years), an abnormal neurological exam between seizures, or a brachycephalic breed all raise the suspicion of a structural or reactive cause and tilt the conversation towards imaging (De Risio et al., 2015; Hall et al., 2020; Prodger et al., 2025). These factors guide how far to investigate. They don't replace the tests.
Your phone earns its keep here too. Seizures almost never happen in front of the vet, so a video of the event, plus an accurate record of how often it's happening in the Seizure Diary, genuinely helps your vet judge which category fits.
A note on cats: the balance is different

The same three categories apply to cats, but the balance between them does not, and for a cat owner this is the thing to understand above all. In cats, structural and reactive causes are relatively more common, and idiopathic epilepsy comparatively less common, than in dogs. In one series of 91 cats with seizures, the causes broke down as roughly 50% structural, 22% reactive and 25% idiopathic or presumed idiopathic, with the small remainder cardiac (Schriefl et al., 2008). A feline review puts it simply: only about 1 in 4 cats with seizures meet the criteria for idiopathic epilepsy (Moore, 2014; Pakozdy et al., 2014).
That shift in the odds is why a cat with seizures usually warrants prompt investigation rather than a wait-and-see approach. On the reactive side, the headline cause in cats is permethrin (pyrethroid) toxicity, a common and entirely preventable emergency. It classically happens when a flea "spot-on" product made for dogs is applied to a cat. Cats can't efficiently break pyrethroids down, so the chemical causes tremors, twitching and seizures, and it can be fatal without prompt treatment (Pakozdy et al., 2014; Moore, 2014). So please never use a dog flea product on a cat, and treat any tremoring after such exposure as an emergency. Other reactive causes include hepatic encephalopathy, low blood sugar, an overactive thyroid and kidney disease (Moore, 2014). On the structural side, cats have a characteristic entity of their own called hippocampal necrosis, alongside tumours such as meningioma and lymphoma, and infections including FIP and toxoplasmosis (Pakozdy et al., 2014; Moore, 2014).
That's the brief version. The full feline cause picture, which differs enough to deserve its own treatment, lives in what causes seizures in cats.
What each category means for the road ahead
Each bucket points down a different road. Reactive heads towards finding and fixing a problem outside the brain rather than lifelong medication. Structural heads towards imaging and treating the underlying disease. Idiopathic heads towards confirming the diagnosis by careful exclusion. The detail of what each test shows, when it's needed and what it costs lives in the diagnostic workup guide.
The reactive category is the one to remember. Among three frightening possibilities, it's the one where the seizures may be entirely fixable, and it's the reason your vet starts by looking at the whole body rather than reaching straight for a brain scan. Knowing which bucket your pet falls into turns an overwhelming "why" into a set of answerable questions. Worked through with your vet, and with a good record of what you've actually seen, those questions are how you move from frightened to in control.
References
- Berendt, M., Farquhar, R. G., Mandigers, P. J. M., Pakozdy, A., Bhatti, S. F. M., De Risio, L., Fischer, A., Long, S., Matiasek, K., Muñana, K., Patterson, E. E., Penderis, J., Platt, S., Podell, M., Potschka, H., Pumarola, M. B., Rusbridge, C., Stein, V. M., Tipold, A., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research, 11, 182.
- Cornell University College of Veterinary Medicine, Riney Canine Health Center. Idiopathic epilepsy in dogs (educational reference page).
- De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Mandigers, P. J. M., Matiasek, K., Packer, R. M. A., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M. P., Rusbridge, C., & Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11, 148.
- Hall, R., Labruyere, J., Volk, H., & Cardy, T. J. (2020). Estimation of the prevalence of idiopathic epilepsy and structural epilepsy in a general population of 900 dogs undergoing MRI for epileptic seizures. Veterinary Record, 187(10), e89.
- Moore, S. A. (2014). Seizures and epilepsy in cats. Veterinary Medicine: Research and Reports, 5, 41-47.
- Pakozdy, A., Halasz, P., & Klang, A. (2014). Epilepsy in cats: theory and practice. Journal of Veterinary Internal Medicine, 28(2), 255-263.
- Prodger, A., et al. (2025). Prevalence of structural and idiopathic epilepsy in brachycephalic and non-brachycephalic dogs in the context of the International Veterinary Epilepsy Task Force guidelines. Journal of Small Animal Practice, 66(8), 540-546.
- Schriefl, S., Steinberg, T. A., Matiasek, K., Ossig, A., Fenske, N., & Fischer, A. (2008). Etiologic classification of seizures, signalment, clinical signs, and outcome in cats with seizure disorders: 91 cases (2000-2004). Journal of the American Veterinary Medical Association, 233(10), 1591-1597.
- Volk, H. A. (2015). International Veterinary Epilepsy Task Force consensus reports on epilepsy in companion animals (editorial). BMC Veterinary Research, 11, 174.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing epilepsy. Free to join.
Join PetsLikeMine