
When Pain Needs a Specialist: The Veterinary Pain Clinic
Dr. Alastair Greenway
MRCVS, 25 years clinical experience
Some owners managing a pet with arthritis reach a particular crossroads. The medication that worked beautifully for a year isn't quite holding any more. The dose has been increased, a second drug added, and still there are bad days that don't make sense. And then the vet says something that lands with a small jolt: "I think it might be worth referring her to a pain specialist."
For a lot of owners, that sentence is frightening. It sounds like an admission that things are serious, that ordinary treatment has failed, that we're approaching some kind of end of the road. Let me start by saying clearly: that is almost never what it means.
Referral to a veterinary pain specialist is good news disguised as worrying news. It means there is more that can be done. It means there is a deeper level of expertise to bring to your pet's problem, a wider set of tools, and a clinician whose entire focus is the thing you most want solved. In twenty-five years of practice I have referred many animals for specialist pain management, and the common thread is not that those animals were beyond help. It is that they needed more than first-line care could offer, and that more was available.
So here is what veterinary pain specialists and pain clinics actually are, when referral happens and why, what a specialist does differently, what treatments they might introduce, and what to expect practically. I hope the word "referral" comes to feel less like a door closing and more like one opening.
Pain management is a discipline of its own
Most owners don't know this, and there's no reason they would: pain management is a recognised area of veterinary specialisation. There are veterinary surgeons who have devoted their careers specifically to understanding and treating pain, particularly the complex, chronic, stubborn pain that doesn't respond neatly to standard approaches.
This matters because chronic pain is genuinely complicated. It isn't simply a matter of "more pain means more painkiller." Pain that has been present for months or years changes the nervous system itself. The pathways that carry pain signals become more sensitive, more easily triggered, harder to switch off. Pain can stop being a straightforward signal of joint damage and become, in part, a problem of the nervous system being wound up. We covered this in our article on central sensitisation, and it's one of the central reasons specialist input can help: specialists are trained to recognise and treat the pain that has become its own problem.
A general practice vet is a generalist by definition, and a very skilled one. They manage arthritis, skin disease, heart conditions, dentistry, emergencies, and everything else, all in a typical day. A pain specialist does one thing, and does it with a depth that a generalist simply doesn't have time to develop. When your pet's pain has moved beyond the straightforward, that depth is exactly what's needed.
When referral happens, and why
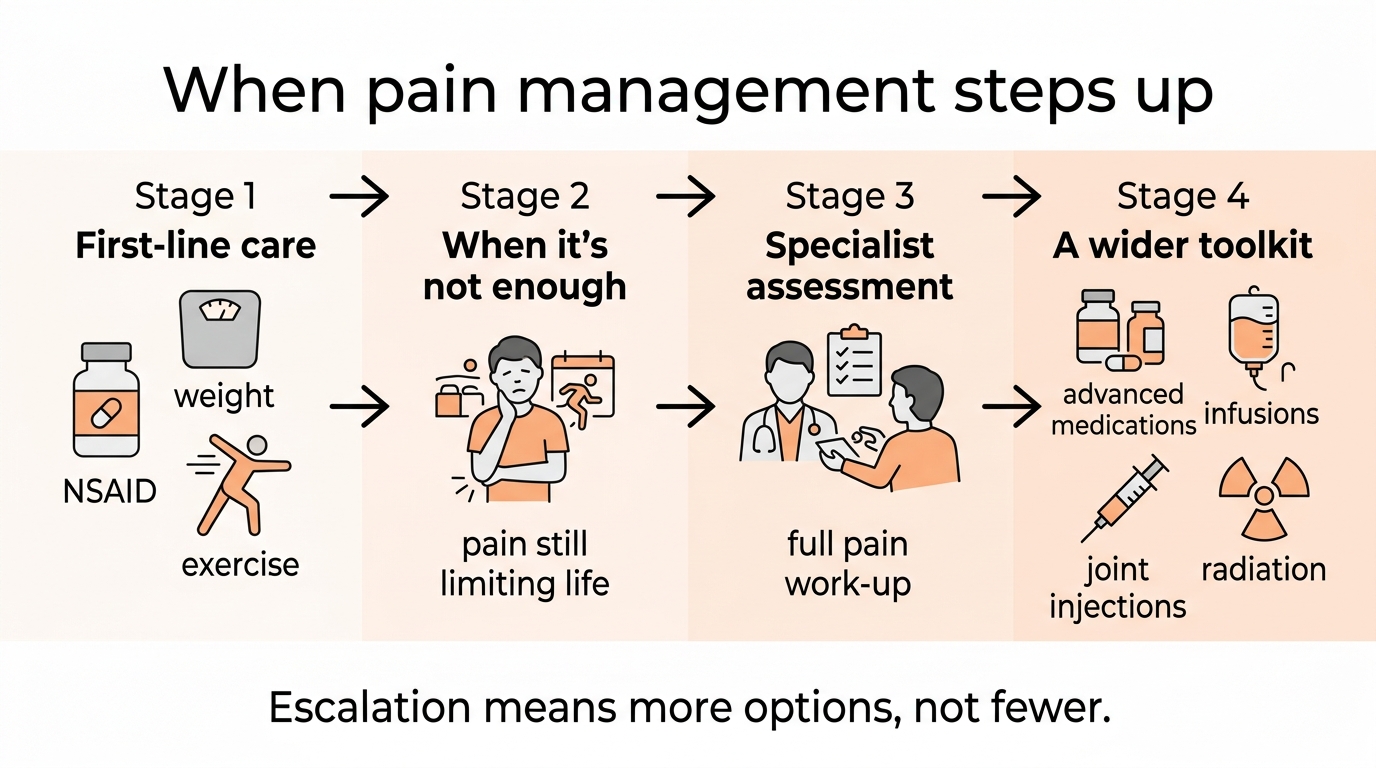
Referral for specialist pain management typically arises in a few recognisable situations. None of them mean something has gone wrong. All of them mean the situation has reached the edge of what first-line care comfortably handles.
First-line management is no longer holding. Your pet was well controlled on an NSAID, perhaps with a second medication added, and that control has slipped. The obvious next steps have been tried. The pain is breaking through in ways that the current plan isn't catching.
The pain looks more complex than simple joint pain. Some pets show signs that suggest the nervous system has become involved beyond the joints themselves. Pain that seems out of proportion to the imaging, sensitivity in areas away from the affected joints, a pet that flinches or reacts in ways that don't fit a simple mechanical picture. These features point toward the kind of pain specialists are particularly good with.
Your pet can't take the usual medications. Some animals can't tolerate NSAIDs because of kidney disease, liver problems, or gut sensitivity. When the foundation drug is off the table, the picture becomes more complicated, and a specialist's wider toolkit becomes valuable.
Multiple joints or multiple problems are involved. A pet with arthritis in several joints, or arthritis alongside other painful conditions, presents a more tangled problem than a single arthritic hip. Specialists are comfortable with that tangle.
Nobody is quite sure what's going on. Sometimes the referral is as much diagnostic as therapeutic. A specialist may identify components of the pain that hadn't been recognised, and that recognition opens up treatments that weren't previously on the table.
In all of these, the referral is an escalation of expertise, not an admission of defeat. Think of it the way you'd think about being referred from your GP to a consultant in human medicine. It isn't that your GP failed. It's that your problem warranted the specialist.
What a specialist does differently

When you take your pet to a specialist pain consultation, several things tend to be different from a standard appointment, and the differences are the point.
More time. A specialist pain consultation is typically much longer than a standard appointment, often forty-five minutes to an hour, sometimes longer. That time allows a depth of assessment that a fifteen-minute consultation cannot.
A deeper pain assessment. Specialists use structured approaches to characterise pain that go well beyond "does it hurt here?" They assess how the pain behaves, where it is, what type it appears to be, and crucially whether features of nervous-system involvement are present. They're looking for the difference between pain that's coming straight from a damaged joint and pain that has taken on a life of its own in the nervous system, because those two things are treated differently.
Recognition of neuropathic and centralised pain. This is perhaps the single biggest thing a specialist brings. The pain that arises from the nervous system being wound up, rather than directly from tissue damage, is easy to miss and responds to a different set of treatments. A specialist is trained to spot it, name it, and treat it specifically.
A willingness to combine treatments thoughtfully. Specialists are comfortable building sophisticated multimodal plans, layering several treatments that each act on a different part of the pain system. Where a general practice might reasonably use one or two medications, a specialist may construct a more elaborate combination, precisely tuned to the individual animal. Our medication explainer tool, which shows where each treatment acts in the pain pathway, includes the specialist-tier treatments for exactly this reason.
Access to treatments not used in general practice. Some of the tools in the specialist's kit simply aren't used at the first-line level, either because they require specific expertise, because they're given in the clinic rather than at home, or because they're reserved for difficult cases. More on these below.
The treatments a specialist might introduce

If your pet is referred, you may encounter treatments your usual vet never mentioned. Let me walk through the main ones at the level of "what this is and why it's used," and then point you to our medication explainer tool for a more interactive view of each, including where they act in the pain system.
Additional nerve-pain medications. Beyond gabapentin, which many general practices use, specialists may reach for pregabalin, a close relative with more predictable absorption. They may add amitriptyline, an older medication that boosts the body's own pain-dampening signals, for pain that has become entrenched. These are the medications that target the nervous-system component of chronic pain.
Amantadine and the NMDA story. Amantadine is increasingly used in general practice too, but it sits squarely in specialist territory conceptually. It works on central sensitisation, the wound-up nervous system, by blocking a receptor called NMDA. It does little on its own but contributes meaningfully as part of a combination. A landmark RCT by Lascelles and colleagues in the Journal of Veterinary Internal Medicine (2008) showed that adding amantadine to NSAID therapy significantly improved owner-assessed physical activity in dogs whose arthritis pain wasn't being adequately controlled by the NSAID alone. The current WSAVA and AAHA pain guidelines both reflect this evidence.
Ketamine infusions. For severe, entrenched pain, a specialist may use a ketamine infusion, given as a slow drip in the clinic over a period of hours. It targets the same NMDA receptor as amantadine but far more powerfully, with the aim of calming a pain system that has become stuck on high. This is borrowed from human chronic-pain medicine, where it's better established. The veterinary evidence is still developing: a 2025 preliminary study by Fry and colleagues in Veterinary Anaesthesia and Analgesia reported on outpatient ketamine infusions for chronic pain in dogs, but there is no full randomised controlled trial yet. It remains reserved for difficult cases where standard treatment has been inadequate.
Joint injections. Rather than treating the whole body, a specialist may inject a single problem joint directly. Several types exist: steroids to reduce inflammation, hyaluronic acid to improve the joint's lubrication, or a newer option using a tiny dose of a tin-117m colloid (sold as Synovetin OA) that delivers very short-range, low-energy electron emission to the joint lining, causing the inflamed synovium to be calmed over time. Synovetin OA is licensed specifically for the canine elbow, with published dose-finding work (Lattimer et al., Veterinary Radiology & Ultrasound, 2023) and a clinical-response study in grade 3 elbow OA (Donecker et al., PLOS ONE, 2021). Injecting one joint directly can be ideal when a single joint is the main source of trouble.
Radiation therapy. A few referral centres offer a short, targeted course of low-dose radiotherapy to a painful arthritic joint. A 2018 preliminary case series by Rossi and colleagues in Frontiers in Veterinary Science reported clinical improvement in 92% of dogs treated with three fractions of 2 Gy, with median benefit of around twelve months after the first course and slightly longer after a second. This is the same tool used in cancer treatment, here used at much lower doses purely to reduce arthritis pain. It's a small, uncontrolled preliminary experience rather than randomised controlled evidence, and the option is available only at certain centres, but for individual dogs whose pain hasn't responded to medication it has produced meaningful benefit.
None of these is a magic bullet. What they represent, collectively, is a deeper bench. When the first-line options aren't enough, there is genuinely more that can be tried, and a specialist knows how to choose and combine them for your individual animal.
What to expect practically

A few practical realities worth knowing before you go.
The referral process. Your general practice vet initiates the referral, sending the specialist a history, examination findings, and any imaging. You don't arrange it yourself. The specialist's clinic will then contact you to arrange the appointment. Bring everything you have, and don't assume the specialist has received every record; gaps in forwarded information are common, so it's worth bringing copies.
The cost. Specialist care costs more than general practice. A specialist pain consultation, with the longer appointment time and the deeper assessment, is a larger fee than a standard consultation, and any advanced treatments add to that. If your pet is insured, specialist referral is usually covered, but check your policy's terms, including any limits on referral or complementary treatments, before you go. We cover the insurance side in detail in our article on funding long-term care.
The relationship with your own vet. Specialist referral doesn't mean leaving your regular vet behind. In the usual model, the specialist assesses, recommends, and often initiates treatment, then communicates the plan back to your general practice vet, who continues the day-to-day management. You keep your existing vet relationship; you've simply added expertise to the team. Our article on building your dog's care team explains how this coordination works.
Ongoing management. Some specialist treatments are one-off or occasional, given at the clinic. Others become part of the daily routine your own vet then oversees. The specialist's job is often to work out the right plan; your vet's job is to help you run it. Expect the specialist to want to review progress, at least initially, to see whether the plan is working and adjust it.
The real possibility that not everything works. A specialist brings more options, but not guarantees. Some treatments will help your pet enormously; some may not do much; finding the right combination can take some trial and adjustment. A good specialist is candid about this, and frames the work as a process of finding what helps your individual animal rather than a single definitive fix.
Reframing what referral means

When your vet suggests a pain specialist, the instinct is to hear it as bad news. Your mind goes to the question you're most afraid of. But the logic runs the other way. A vet suggests specialist pain management precisely because they believe there is more worth trying, and because they want your pet to have access to expertise beyond their own. It is an act of advocacy for your animal, not a surrender.
I've seen dogs who could barely settle at night, whose owners were starting to have the hardest conversations with themselves, transformed by a specialist getting the pain plan right. Not cured, because arthritis isn't curable, but comfortable. Engaged again. Sleeping. The dog the family remembered. That transformation is what the specialist tier of pain management exists to deliver, and it's why referral, far from being the end of the road, is often the thing that gives an animal a good stretch of road still to travel.
If your vet raises the possibility, my advice is to take it as the opening it is. Ask what the specialist might be able to offer. Ask about the cost and the practicalities. Use our medication explainer tool to understand the treatments you might encounter. And go into it understanding that the referral itself is a sign that your pet's situation is taken seriously and that there is more good care still to come.
The pain can almost always be helped. Sometimes helping it well needs a specialist. That isn't a failure of anyone's care. It's the system working as it should, bringing the right expertise to bear at the moment it's needed.
References
- Lascelles BDX, Gaynor JS, Smith ES, Roe SC, Marcellin-Little DJ, Davidson G, Boland E, Carr J. Amantadine in a multimodal analgesic regimen for alleviation of refractory osteoarthritis pain in dogs. Journal of Veterinary Internal Medicine, 2008;22(1):53-59.
- Lattimer JC, Fabiani M, Gaschen L, Aulakh K, Selting K. Clinical effectiveness and safety of intraarticular administration of a 117mTin radiocolloid (Synovetin OA) for treatment of early and intermediate grade osteoarthritis of the elbow in a dose finding study conducted in 44 dogs. Veterinary Radiology & Ultrasound, 2023;64(2):351-359.
- Donecker J, Fabiani M, Gaschen L, Aulakh KS. Treatment response in dogs with naturally occurring grade 3 elbow osteoarthritis following intra-articular injection of 117mSn (tin) colloid. PLOS ONE, 2021;16(7):e0254613.
- Rossi F, Cancedda S, Leone VF, Rohrer Bley C, Laganga P. Megavoltage radiotherapy for the treatment of degenerative joint disease in dogs: results of a preliminary experience in an Italian radiotherapy centre. Frontiers in Veterinary Science, 2018;5:74.
- Fry L, Rychel J, Tearney C, Guedes A. Preliminary study of intravenous ketamine infusions for the management of chronic pain in dogs. Veterinary Anaesthesia and Analgesia, 2025;52(1):124.e3-124.e4.
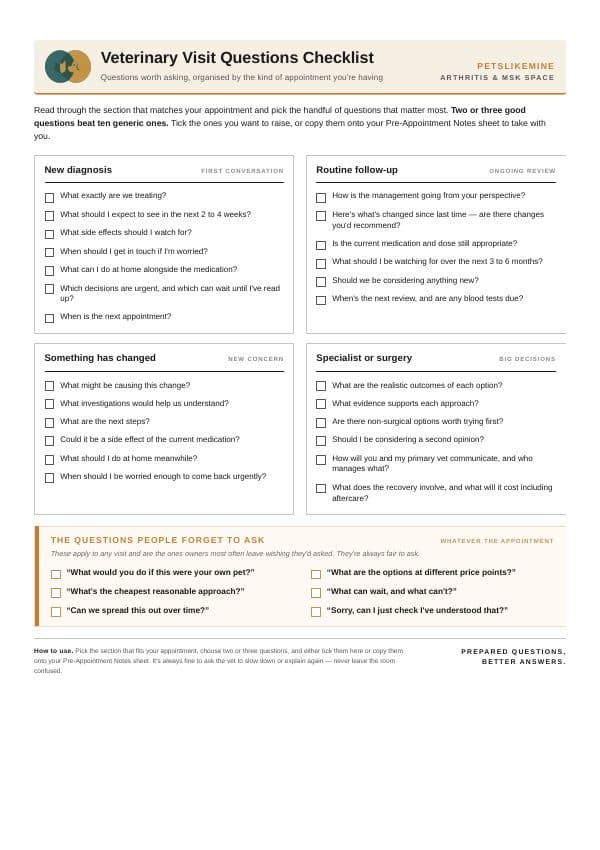
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentSee where your pet stands today
Tracking is the other half of managing arthritis. Take the 2-minute Mobility Check to see your pet's stage, then watch it shift as treatment takes effect.
Take the Mobility CheckYou're not doing this alone
Compare treatment journeys and talk to owners managing arthritis. Free to join.
Join PetsLikeMine